
Abstract
Background:
Hepatitis C virus (HCV) infection is commonly comorbid with opioid dependence (OD). We wanted to compare the neurocognitive functions of OD subjects with or without HCV [HCV (+), HCV (–)] and healthy controls (HC).
Methods:
We recruited 40 adult subjects (age 18–55 years) in each group. HCV(+) group had a detectable viral load. Subjects with HIV or hepatitis B infection, head injury, epilepsy, or comorbid mental illness were excluded. We administered Standard Progressive Matrices (SPM), Wisconsin Card Sorting Test, Iowa Gambling Task (IGT), trail-making tests A and B, and verbal and visual N-back tests (NBT) one week after opioid abstinence. The group differences in cognitive performance were adjusted for age and years of education. Effect size (ES) is expressed as Cohen’s D.
Results:
The HCV(+) and HCV(–) groups did not differ in potential effect modifiers (age and years of education) or confounders (age of opioid initiation, duration of use, dependence severity, tobacco use, and cannabis use) of neuropsychological functioning. HCV(+) showed significantly poorer performance than HCV(–) in SPM (P = 0.006; ES = 0.72). Both HCV(+) and HCV(–) performed worse than controls in IGT(P < 0.001; ES = 0.8) and visual NBT[P < 0.01 and ES > 1 for total errors]; HCV(+) had a larger ES of group difference than HCV(–). HCV(+) had higher error scores in verbal NBT than control.
Conclusion:
HCV(+) has poorer general intellectual ability and reasoning than HCV(–) persons and controls. Chronic HCV infection causes a higher magnitude of dysfunction in decision-making and visual working memory in opioid-dependent individuals.
Opioid-dependent patients with or without comorbid HCV infection have a widespread cognitive impairment. Opioid-dependent patients with HCV infection had poorer general intelligence, decision making, and visual working memory.Key messages:
Of Persons Who Inject Drugs (PWID), 50%–80% are seropositive with hepatitis C virus (HCV).1, 2 A substantial majority of PWID use opioids. 1 The prevalence of HCV in non-injection drug users (NIDU), of which a majority are opioid users, is also higher than that of the general population. 3
Heavy opioid use is associated with dysfunctions in executive decision-making, attention span, concentration, vigilance, recall, visuospatial skills, reaction times, and psychomotor speed. 4 Cognitive impairments in domains of impulsivity, cognitive flexibility, and memory were also observed in patients on treatment for opioid dependence (OD). 5 As the cognitive dysfunction is more severe in the untreated group, impairments may improve with treatment and abstinence.6, 7, 8, 9
Clinical and subclinical neurocognitive impairment has also been observed in up to 50% of patients with chronic hepatitis. 10 The impairments are more in patients with cirrhosis. Immunological mechanisms and altered gut microbiota may play a role in the pathogenesis.11, 12 The affected cognitive domains include attention, concentration, learning, cognitive flexibility, processing speed, and executive function.13, 14 The cognitive impairment negatively impacts functionality, quality of life, treatment adherence, and treatment outcome.13, 15
Pathophysiology of cognitive dysfunctions in HCV infection involves both direct viral invasion and perivascular inflammation and the indirect effects of neuro-inflammation, bile acid modifications, changed microbiome, and systemic inflammation. 16 The cognitive effects of opioids are likely to result from their direct action on the mu-opioid receptors in limbic and cortical areas. 17 The distinctive mechanisms raise the possibility of a synergistic or additive effect of OD and chronic HCV infection on neuropsychological functions. 18 Additional evidence is seen when treatment of HCV improves cognitive function after achieving sustained virological response. 19
Despite the high co-occurrence, significant evidence of involvement of cognitive functions in both disorders, and potential clinical implications, neuropsychological functioning in individuals with comorbid OD and HCV has not been studied.
Our study aims to compare the performance of three groups, that is, individuals with OD with hepatitis C [HCV(+)], individuals with OD without hepatitis C [HCV(–)], and healthy control (HC) on a battery of neuropsychological tests. We hypothesized that individuals with OD with HCV would have a poorer neuropsychological function in one or more cognitive domains than individuals without HCV and that both the groups would have a worse neurocognitive function in one or more domains than the HCs.
Methods
This cross-sectional comparative study was approved by the PGIMER (Intramural) Chandigarh Institutional Ethics Committee.
Setting
The sample was recruited from a tertiary care addiction treatment center in the northern part of India. The treatment team consists of qualified psychiatrists and addiction psychiatry specialists who perform detailed workups and diagnose cases according to the International Classification of Diseases 10th revision (ICD 10). Our clinic has a linkage service with the hepatology clinic of our tertiary care hospital.
Participants
The study sample consisted of 40 subjects in each of the three groups: HCV(+), HCV(–), and HC. The control group consisted of non-blood-related family and friends accompanying patients to the treatment center. The period of recruitment was between March 2017 and December 2019. We had to use nonrandom sampling because: (a) To include patients with OD; we excluded patients with other comorbid substance use disorders, except tobacco and cannabis. The latest data from our center showed that the prevalence of polysubstance use disorder was >13% in 2008 and that it had an increasing trend in the last three decades. 20 (b) We wanted to include patients with a definitive diagnosis of being HCV seropositive (by ELISA and viral loads). A large proportion (60%) of our patients drop out within a month of their first consultation; these test reports would not be available for them 21 and these essential selection criteria would not have been met for a large number of patients.
Selection Criteria
A qualified psychiatrist diagnosed OD as per ICD 10. The recruited participants were within the age range of 18–55 years and from both sexes. The diagnosis of OD, any other substance dependence, and/or any other psychiatric illness was confirmed by the Mini International Neuropsychiatric Interview (MINI). 22 The HCV(+) group was screened positive for anti-HCV antibody and had a detectable viral load in the blood sample. Patients were enrolled if they were treatment naïve and did not receive any treatment for HCV infection till the completion of the administration of neuropsychiatric battery, which was performed in a single sitting (it took around one and a half hours). They must not have had liver cirrhosis, documented by clinical examination and fibroscan or abdominal ultrasound. The HCV(–) and HC groups were screened negative for anti-HCV antibodies. The study groups did not have any other substance use disorders (except for cannabis and tobacco in the OD groups), HIV, head injury, epilepsy, major depressive episode, or severe mental illness. The participants were abstinent from illicit drugs for at least one week. They did not have any active opioid withdrawal symptoms (Clinical Opiate Withdrawal Scale [COWS] 23 score of ≤6) at the time of assessment. Urine chromatographic immunoassay was done to screen for recent use of illicit opioids. We had to exclude 12 participants because of these criteria.
Sample Size Calculation
We set the alpha value at 0.05. The amount of variance in cognitive impulsivity (dependent variables) attributed to the group effect (independent variable) was adjudged to be 0.70. This effect estimate was derived from a meta-analysis of studies comparing the neuropsychological functioning of chronic heavy opioid users and controls. 24 It was seen that a minimum of 40 subjects would be required in each group (a total of 120 subjects) to have 80% power (beta 0.2).
Assessments
Demographic Information
Questions were designed to collect data regarding age, years of education, income, and other related demographic variables.
Clinical Information
A clinical information sheet was specially devised for this study. The data included age of first use of opioids, duration of use, duration of dependence, and predominant type of opioid use. The severity of OD was assessed by the Severity of Opioid Dependence questionnaire (SODQ). 25 COWS was used to assess the severity of withdrawal symptoms. 23 Measurement of viral load, liver function test, ultrasound abdomen, and liver fibroscan were planned for the HCV (+) group.
Neuropsychological Assessments
Standard Progressive Matrices: We used the original version of Raven’s Progressive Matrices (SPM). 26 Based on inductive and deductive reasoning, SPM estimates fluid intelligence. It is unlikely to be affected by existing knowledge and years of formal education. In sum, SPM would assess the general factor of intelligence.
Iowa Gambling Task (IGT): It is a computerized task to assess the cognitive domain of decision-making. It can assess cognitive impulsivity or risk-taking behavior and decision-making. The parameters we used were net score obtained and total money earned. The net score is determined by the difference in the number of cards chosen from the advantageous versus the disadvantageous decks. 27
Wisconsin Card Sorting Test (WCST): We used the computerized version of the 64-item WCST to determine cognitive flexibility, working memory, attention, and executive function. The total errors and perseverative errors were used to measure cognitive flexibility. We measured the nonperseverative error to assess the ability to avoid distraction (sustained attention). The percentage of conceptual-level responses determined conceptual thinking or executive function. 28
N Back tests: Paper versions of verbal and visual 2 back tests were administered to assess the verbal and visual working memory and response inhibition. Commission errors were calculated to determine impulsivity. We recorded the accuracy of responses, which is suggestive of working memory and executive control. Omission errors were also measured for both tasks. The reason for assessing both omission and commission errors was that they tap different aspects of working memory. 29
Trail Making A and Trail Making B tests (TMT): TMTs are developed to assess attention, visual search, scanning, set-shifting, psychomotor speed, and flexibility. We measured the time taken to complete the TMT A and TMT B as variables of interest. 30
Description of the Neurocognitive Tests.
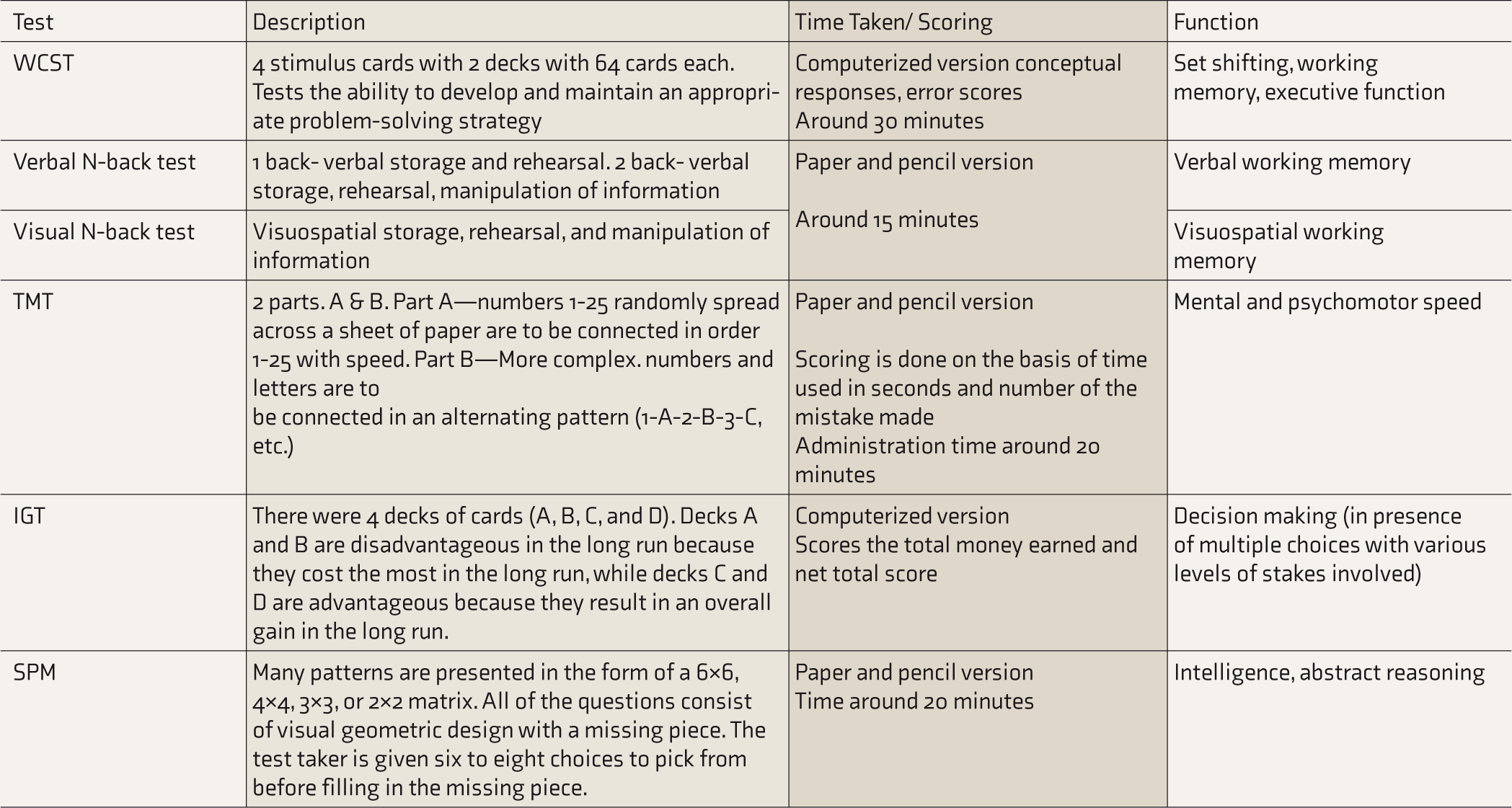
WCST: Wisconsin Card Sorting Test, TMT: Trail Making Test, IGT: Iowa Gambling Test, SPM: standard progressive matrices.
Procedure
Written informed consent was obtained from all the participants. MINI was used to confirm the diagnosis of OD and screen for major depressive episodes, severe mental illness, and other substance dependence.
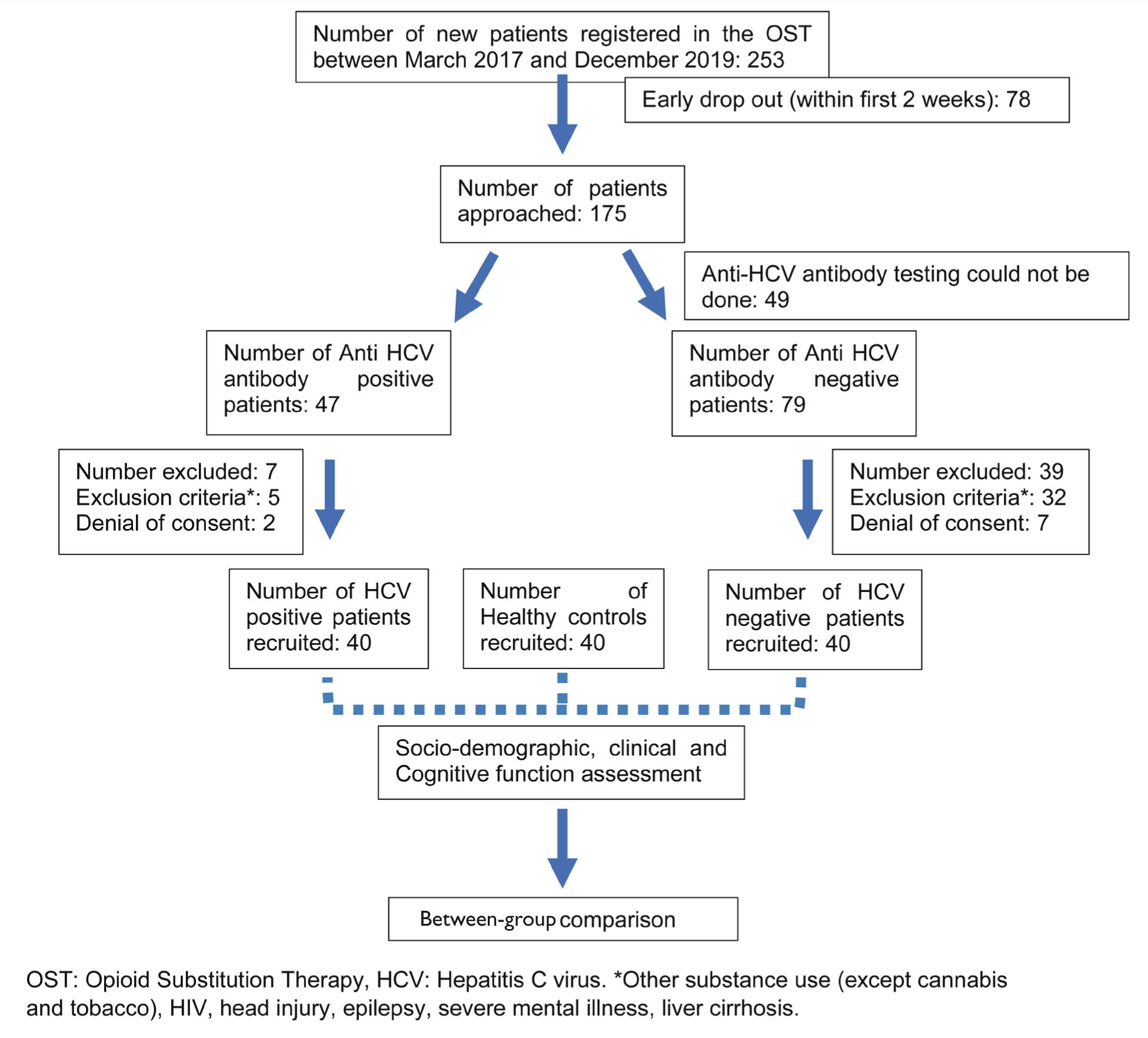
Our clinic has a linkage service with the hepatology clinic of our tertiary care hospital. All patients with opioid use disorders (with a history of injection drug use) are screened for anti-HCV antibodies, HIV, and hepatitis B as a routine clinical practice. Patients screened positive are linked to hepatology or antiretroviral (ART) clinic services for further medical care for those infections. Subjects with a positive anti-HCV antibody were tested for viral loads and other clinical parameters pertaining to hepatitis C. All participants were started on a buprenorphine-naloxone fixed-dose combination. The neurocognitive assessments were done after a minimum of seven days of abstinence from illicit opioids and at least three to four days after confirmation of HCV diagnosis. A psychiatrist performed the clinical evaluation in a single sitting. Cognitive assessments were conducted by a clinical psychologist (with a PhD in Clinical Psychology), who was unaware of the group allocation. Participants were not provided with any compensation or incentives for study participation. See Figure 1 for a detailed study flow.
Study Flow Diagram.
Statistical Analysis
Demographic and clinical variables are represented using descriptive statistics. We used independent sample t-tests and analysis of variance (ANOVA) to compare the demographic and clinical variables between the patient groups and between patients and controls, respectively. Comparison of the neurocognitive domains (dependent variable) of all the three separate groups (fixed factors) of participants was performed with the general linear model. We entered the age and years of education as covariates because these characteristics differed significantly between the groups. Levene’s test of equality was used to test for the homogeneity of variance of age across the groups. Pairwise comparisons were performed with the Bonferroni procedure. Finally, we adjusted the significance level by Benjamini–Hochberg correction, to minimize the alpha error. The effect size (ES) is expressed as Cohen’s D, and the cut-off values were 0.2, 0.5, and 0.8 for small, medium, and large ESs, respectively. Statistical Package for Social Sciences, 14th version (SPSS 14) was used for data analysis. 31
Results
A total of 40 OD patients, each with HCV(+) and without HCV(–) and 40 HC were enrolled, and their demographic, clinical, and cognitive functions were compared.
Demographic Characteristics
Mean age of HCV(+) and HCV(–) groups was significantly lower than that of the HC group (P < 0.001 and P = 0.005, respectively). Mean years of education in the HC group was significantly higher than in the HCV(+) and HCV(–) groups (P = 0.005 and P < 0.001, respectively).
Clinical Characteristics of HCV(+) and HCV(–) Groups
We did not find any group differences in the age of onset of opioid use, duration of opioid use or dependence, or SODQ scores. Heroin was the predominantly used opioid, and the intravenous route was the commonest mode in both groups (Table 2).
Comparison of Sociodemographic and Clinical Characteristics.
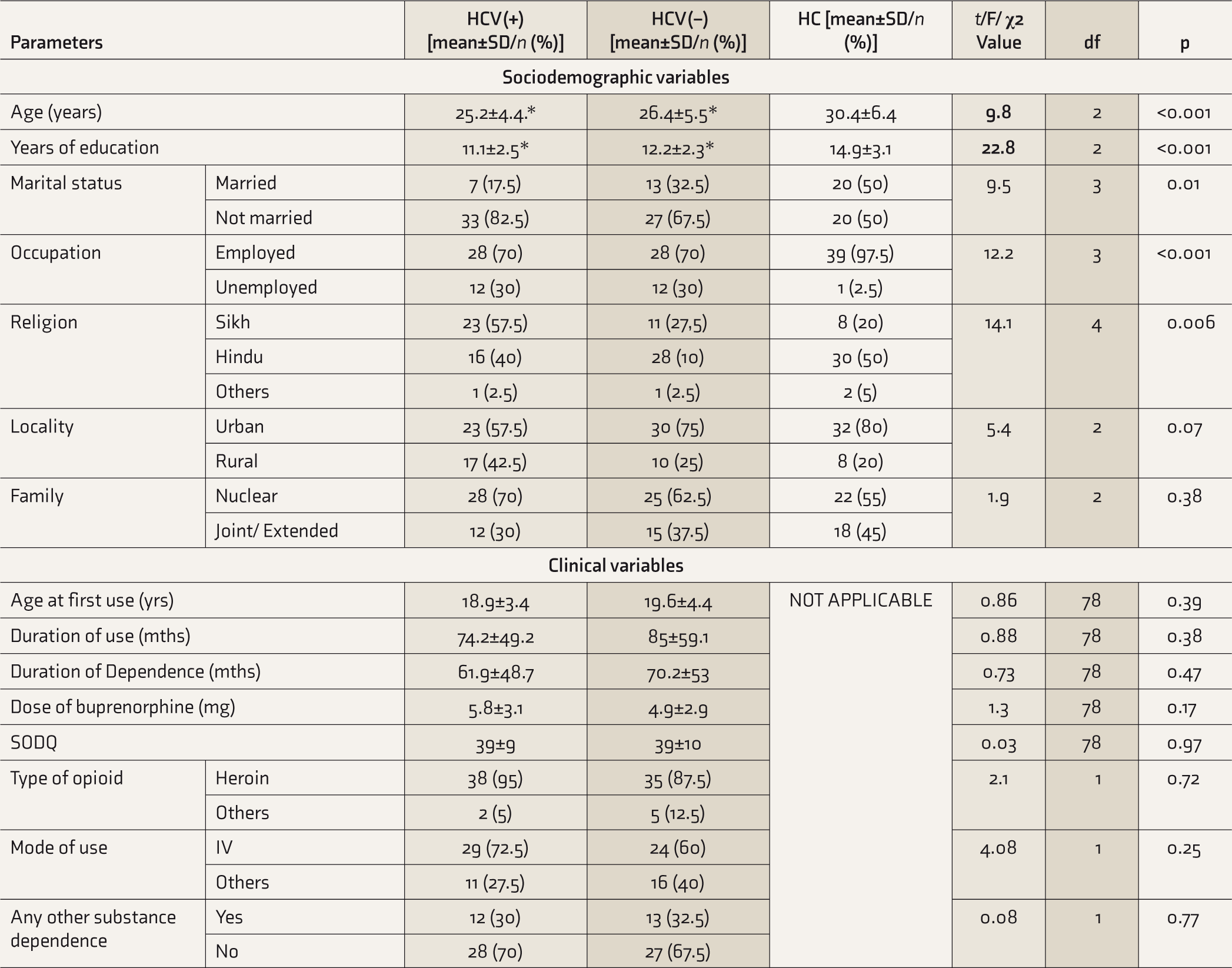
HCV(+): opioid dependence and active hepatitis C infection, HCV(–): opioid dependence without hepatitis C infection, HC: healthy control, SD: standard deviation, SODQ: Severity of Opioid Dependence questionnaire, IV: intravenous; df: degree of freedom,
HCV-Related Variables in the HCV(+) Group
HCV viral load was determined in all 40 HCV(+) participants, but the other tests were performed on fewer participants. The mean viral load was around 12×5 log copies/ml (SD = 25 lakh, range = 6.7×10 3 to 8.1×10 6 copies/ml). The Alanine Aminotransferase (ALT) level was available for 35 patients. The mean ALT level was 65.5 IU/L (range 15–195 IU/L; SD = 53.2). Liver stiffness measure of 17 patients was recorded (mean: 6 KPa; SD = 1.7; range: 3.6–9 KPa).
Pairwise Comparison of Neurocognitive Function Between the Three Groups
We compared the neurocognitive performance across the three groups after controlling for age and years of education.
Standard Progressive Matrices
The SPM IQ in HCV(+) patients was significantly lower in comparison to the HCV(–) (P = 0.006; ES = 0.72) and HC (P = 0.004; ES = 1.14), with moderate and large ES, respectively.
Wisconsin Card Sorting Test
Total correct and conceptual-level responses were higher in HC than the other groups. Moreover, the total error, perseverative and non-perseverative errors were lower in HC than the other groups. However, the intergroup comparison revealed no significant differences in the scores of various parameters in the WCST.
Iowa Gambling Task
The net total score of HCV(+) patients was significantly lower than that of HC, with a large ES (P < 0.001; ES = 0.82). The net total score of HCV(–) patients was significantly lower than that of HC, with a moderate ES (P < 0.001; ES = 0.78). The total money earned by HCV(+) patients was significantly lower than that of HC, with a moderate ES (P = 0.001; ES = 0.62). Total money earned by HCV(–) patients was also significantly lower than that of HC, with a moderate ES (P = 0.002; ES = 0.58). The net total score and total money earned by HCV(+) patients were lower than those in HCV(–) patients, but the differences were not significant.
Trail-Making A and Trail-Making B
HCV(–) patients took a longer time to complete TMT A than HC, with a large ES (P < 0.001; ES = 0.91). There were no significant intergroup differences in the time taken to complete the TMT B test.
Verbal Working Memory 1 Back Test
Mean total correct response was the lowest, and omission, commission, and total errors (of omission and commission) were the highest, in the HCV(+) group. When compared with the other groups, none of the differences attained statistical significance.
Verbal Working Memory 2 Back Test
HCV(+) patients had significantly fewer correct responses than HC. ES of the group difference was large (P = 0.01; ES = 0.9). HCV(+) patients committed more omission errors than HC (P = 0.008; ES = 0.74). The mean number of commission errors showed a similar trend, although none of the intergroup comparisons reached statistical significance. HCV(+) subjects had more total error scores than HC (P = 0.01; ES = 0.9).
Visual Working Memory 1 Back Test
HCV(–) and HCV(+) groups had fewer correct responses than HC (P = 0.01 and <0.001; ES = 0.23 and 0.34, respectively). HCV(–) and HCV(+) groups committed more omission errors than HC (P = 0.007 and <0.001; ES = 1.26 and 1.52, respectively). HCV(+) group produced more commission errors than HC (P = 0.001; ES = 1.19). Mean number of total errors (omission and commission) was highest in the HCV(+) group, followed by the HCV(–) and HC. Pairwise comparisons showed significant group differences.
Visual Working Memory 2 Back Test
HCV(+) and HCV(–) groups produced fewer correct responses than HC (P < 0.001). Similar group differences were also observed in omission errors. HCV(–) group produced more omission errors than HC (P = 0.01; ES = 0.82). The total error scores were significantly higher in both the patient groups than in HC (Table 3).
Comparison of Neurocognitive Functions.
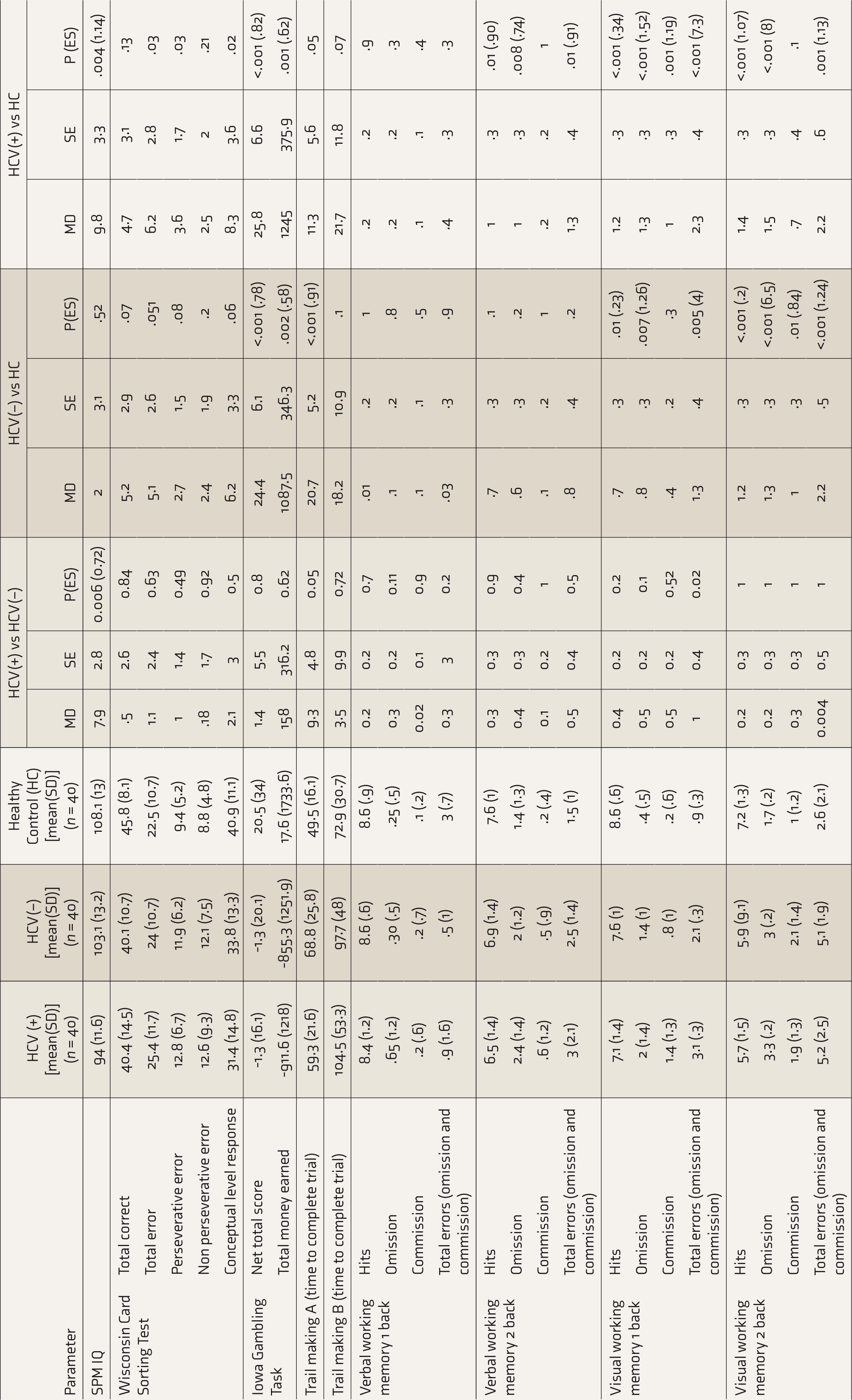
HCV(+): opioid dependence and active hepatitis C infection, HCV(–): opioid dependence without hepatitis C infection, HC: healthy control, SD: standard deviation, MD: mean difference, ES: effect size (Cohen’s D), SE: standard error; SPM IQ: intelligence quotient assessed using Standard Progressive Matrices. Bold values are significant after Benjamini–Hochberg correction.
Discussion
There was no published literature comparing the neuropsychological functioning of opioid-dependent patients with or without HCV infection. We have demonstrated the neurocognitive effects of chronic heavy opioid use by including HC subjects as a comparison group. The cognitive functions were assessed after at least seven days of abstinence from opioids to minimize the acute effects of the drugs or the withdrawal symptoms on neurocognitive functions. 16 We studied a wide range of cognitive functions: decision-making, cognitive impulsivity, cognitive flexibility, conceptual thinking, attention, and working memory. We controlled for age and years of education, which are effect modifiers for neuropsychological performance.32, 33 We dealt with potential confounders by excluding subjects with comorbid drug or alcohol use disorders (except for tobacco and cannabis), psychiatric disorders, epilepsy, and head injury. Other confounders that might influence cognitive functions in patients with OD, such as the severity of OD, the severity of opioid withdrawal, age of initiation, duration of opioid use and dependence, and the frequency of comorbid tobacco or cannabis use disorders, were also assessed. 15 We used Benjamini–Hochberg’s correction to address the possible inflation of alpha value owing to multiple pairwise comparisons. The clinical psychologist who applied the neuropsychological battery was not aware of the group of the participants; hence, we might have minimized the risk of assessment-related bias.
The HCV(+) and HCV(–) groups did not differ with regard to potential effect modifiers (e.g., age and years of education) and confounders (e.g., age of initiation of opioid use, duration of use, severity of dependence, comorbid tobacco and cannabis use) of neuropsychological functioning. Hence, the differences in the performance of the neuropsychological tests could be associated with the active and untreated HCV infection.
Direct comparison of the HCV(+) and HCV(–) groups revealed a significantly poorer performance of the HCV(+) subjects in SPM, suggestive of greater impairment in general intellectual ability and abstract reasoning. Moreover, SPM scores were significantly lower in the HCV(+) than HC. The magnitude of impairment (assessed by ES) was greater in HCV(+) vs HC than in HCV(+) vs HCV(–). However, there was no difference in SPM scores between HCV(–) and HC. These findings indicate that impairment in global intellectual functioning is unlikely to be attributed to chronic opioid use and is more likely to have resulted from HCV infection. HCV can cross the blood–brain barrier, infect the microglial cells, and consequently have a direct toxic effect on the brain or indirect effect due to neuro-inflammation.15, 34, 35 This synergistic or additive effect of HCV over and above chronic opioid use might explain the additional impairment in intellectual functioning. The presence of depression can also adversely affect cognitive functions in HCV(+) subjects; however, we excluded major depressive episodes in our sample. Our results reiterate that HCV independently contributes to cognitive dysfunctions, in line with the previous literature.12, 36
Both HCV(+) and HCV(–) subjects performed significantly poorer than HC in IGT and NBT for visual working memory, suggesting overlapping cognitive dysfunctions in the domains of cognitive impulsivity, decision-making, and visual working memory. Similar cognitive impairment has been reported among HCV patients (with or without substance use disorders).37, 38 Previous meta-analysis and reviews showed that patients with OD have a widespread cognitive impairment that affects attention, working memory, impulsivity, and decision-making.23, 39 The magnitude of impairment (measured by ES) was numerically higher in the HCV(+) than the HCV(–) group. This finding was consistently present across all parameters of IGT and NBT, supporting the reliability of the results. The higher degree of impairment in the HCV(+) could be due to the adverse synergistic effect of HCV on brain function, as mentioned above. The HCV(+) subjects committed more errors in the verbal N-2 back test (verbal-NBT) than the control, indicating a verbal working memory dysfunction. Although the HCV(–) group performed poorer than HC and better than HCV(+), these differences were statistically nonsignificant. Nevertheless, the trend of higher to lower cognitive dysfunction from the HCV(+) and HCV(–) to HC was also seen for verbal working memory.
Finally, HCV(–) required significantly more time than HC to complete TMT-A, reflecting poorer attention and working memory. This impairment is likely an effect of chronic heavy opioid use. 23 It was interesting to note that HCV(+) did not differ significantly from HC and that the usual trend of cognitive dysfunction was not observed in TMT-A. Except for general intellectual functioning, HCV(+) and HCV(–) did not differ significantly in any other cognitive domains. This null finding could be explained by the fact that both HCV(+) and HCV(–) had severe OD (as assessed by the SODQ) 40 and, consequently, had higher cognitive dysfunctions. Our study was not adequately powered to detect smaller group differences. Nevertheless, the degree of impairment compared to HC was more in HCV(+) than in the HCV(–) .
Our results should be read in light of the following caveats: (a) We did not consider the emotional reaction of the participants after knowing their HCV status and its possible effect on their motivation to participate in the study and their performance in the tests. Although the knowledge of contracting the infection may affect motivation and performance, we consider the possibility to be narrow, as many of the subjects were already aware of their HCV status before entering treatment. For the rest of the patients, the neurocognitive tests were applied after 3–4 days of confirmation of their HCV seropositivity. During this period, we counseled them on hepatitis C, treatment options, and prognosis. This should have allayed participants’ anxiety. (b) Our sample did not have females. This was not due to the design of the study but reflective of the very low prevalence of opioid use (4% in men vs 0.2% in women) and low treatment-seeking behavior of women in India.20, 41 However, we consider this as a major limitation for the generalizability of our results. (c) Ours was a cross-sectional comparison of different groups of subjects; hence, causal inference between HCV and neurocognitive dysfunction should not be drawn. (d) Our study may not be adequately powered to detect smaller difference between the HCV(+) and HCV(–) groups; we did not study the relationship between various HCV parameters (e.g. viral count, levels of ALT, level of liver fibrosis) and scores in cognitive tests because these parameters were available for only 30 subjects; hence, any statistical analysis in this sample would have been underpowered. (e) Most participants were heroin users; therefore, the results may not hold true for other forms of opioid use. (e) And if we had a group with HCV (without OD), we could have demonstrated the gradient of cognitive impairment among those with comorbid HCV and OD, only OD, only HCV, and HC.
Our study showed that opioid-dependent subjects with HCV have poorer general intellectual ability and abstract reasoning than subjects without HCV and HC. Although the opioid-dependent groups with or without HCV both performed poorly in decision-making and visual working memory tasks, the magnitude of dysfunction was higher in subjects with HCV. Moreover, the impairment in verbal working memory was seen only in HCV-positive subjects. These findings suggest greater neurocognitive impairment in comorbid OD and HCV infected patients. The untreated cognitive impairment may adversely affect treatment adherence and outcome.13, 14
Future research should ascertain the reversal of such impairment after successful treatment with directly acting antivirals under India’s national program wherein all oral antiviral therapy (Sofosbuvir plus NS5A inhibitor) is made available free of charge to the patient at a local government hospital. The linkage of opioid agonist treatment centers and HCV therapy will augment the improvement in neurocognitive impairment due to concurrent HCV infection and substance abuse, improving quality of life and health outcomes. 42 Future studies should also test the association between HCV parameters and cognitive functions in a larger sample and a longitudinal design to ascertain the potential causal association between HCV infection and neurocognitive dysfunctions in patients with OD. Studies should also investigate the effect of neurocognitive dysfunctions on functional and treatment outcomes among opioid-dependent patients with HCV.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.