
Abstract
Background:
Substance use disorder is a complex bio-psycho-social phenomenon affecting the intimate relationship of substance users with their wives. Marital adjustment may be affected due to the ongoing substance use involving the family unit. The present study aimed to compare marital adjustment between alcohol- or opioid-dependent patients and their spouses.
Methods:
The present cross-sectional observational study compared 25 dyads each of alcohol- and opioid-dependence syndrome taken from the outpatient department of an addiction treatment center in north India. Marital adjustment was compared using the Marital Adjustment Questionnaire (MAQ). Maudsley Addiction Profile and Eysenck’s Personality Questionnaire were also applied to the patients, and Social Support Questionnaire was applied to both patients and spouses.
Results:
There was no significant difference in the sexual, social, and emotional domains and total MAQ scores between patients with alcohol- and opioid-dependence syndrome or their spouses. There was a significant positive correlation between the sexual domain score of MAQ of alcohol-dependent patients and their spouses (r = 0.655, p < .001). The Maudsley Addiction Profile parameters, personality profile, and social support did not differ significantly across the two groups.
Conclusion:
Marital adjustment are probably equal in patients and spouses of alcohol and opioid dependence syndrome. A small sample size is a limitation of this study.
Marital adjustment are probably comparable among spouses of patients with alcohol and opioid dependence, though their stage and duration of marriage may be different. Neuroticism, extraversion and psychoticism are probably similar
among patients with alcohol and opioid dependence. Social support did not significantly correlate with the marital adjustment in both the groups.Key Messages:
The history of the use of psychoactive substances is centuries old. Substance use disorders (SUDs) and other addictive behaviors remain among the most crucial global issues and affect approximately 36 million people worldwide.1, 2 Alcohol dependence seems to be the most common substance use disorder worldwide. Among illicit use of drugs, opioid use disorders are the most common diagnoses for which individuals seek treatment. In 2019, 62 million people were estimated to have used opioids for non-medical reasons at the global level, which corresponds to 1.2% of the global population aged 15–64. 3 India is the second most populous nation in the world. The sheer number of individuals residing in the country makes it home to one of the largest substance-using populations. 4 According to a national survey in India, alcohol use disorder affects about 5% of the population, and opioid use disorder affects about 0.55% of the population. 5
The impact of alcohol not only affects the physical health of an individual but also affects the people around them.6–9 Owing to the intimate nature of their relationship, spouses are affected quite considerably due to the substance-using habit of their husbands.10–13 A majority of the spouses of substance-dependent individuals are also the primary caretakers of their husbands and are at risk of domestic violence as well. Overall, it also affects their conjugal life due to decreased communication, lack of understanding, unpredictable behavior of husbands, issues with intimacy, frequent altercations related to substance use, lack of responsibility in family matters, and financial strain owing to substance use of the husbands. Thus, marital life in such cases suffers a setback, and marital adjustment, quality, and satisfaction may be hampered.12, 14, 15
While there is substantive literature on marital aspects of patients with alcohol dependence, literature on marital aspects among the spouses of opioid-dependent individuals is limited. Previous studies have looked at marital satisfaction, distress, quality of life, and co-dependency among spouses of opioid-using individuals.16–18 No study has yet reported on the marital adjustment among spouses of opioid-using individuals. Furthermore, the role of perceived social support and personality of individuals with substance use disorder may have an impact on marital adjustment, and this has been studied less frequently. Hence, in this pilot study, we attempted to compare marital adjustment between patients and spouses of individuals with alcohol and those with opioid use disorder and assessed the relationship of marital adjustment with social support and personality characteristics of the husbands.
Methods
The Setting of the Study, Participants, and Procedure
This cross-sectional observational study was conducted at the outpatient department of an addiction treatment center. It is a tertiary care addiction treatment facility catering to a huge population of substance users. It provides both inpatient and outpatient services. Many facilities are available here, including detoxification, maintenance, community outreach center, specialty care, and aftercare. Most patients are accompanied by their family members, most commonly by spouses. Participation of family members is frequently sought in the treatment process for administering medications on an outpatient basis, providing support, and promoting abstinence.
Men dependent on either alcohol or opioids were recruited along with their spouses. Inclusion criteria of substance-dependent men were age between 25 and 50 years, diagnosed with alcohol dependence syndrome (ADS) or opioid dependence syndrome (ODS) as per ICD-10, received no treatment for substance use in the past three months, married for at least one year, having reading and understanding skill in written Hindi language, and willing and able to give consent. The inclusion criteria for spouses were cohabitation with husbands, with reading and understanding skills in the written Hindi language and willingness and ability to consent. Exclusion criteria for patients and spouses were any psychiatric illness or medical illness that precluded a detailed interview. Dyads were also excluded if the patient had a dependence on another substance (apart from tobacco dependence). For example, if a patient in the ADS group had cannabis dependence, then the dyad was excluded. The sample size was targeted to be 25 in each group to enable comparisons and correlational statistics and was based on feasibility. Matching was not done to ensure representation of the sample of patients coming to the outpatient services with their spouses.
Participants were selected and recruited after obtaining written informed consent. Socio-demographic information and clinical details were obtained from the participants. Maudsley Addiction Profile and Eysenck Personality Questionnaire were applied to the husbands. The Marital Adjustment Questionnaire (MAQ) and Social Support Questionnaire were applied to the husbands and spouses. Data collection was started after clearance from the Institutional Ethics Committee. Data collection took place from August 2021 to February 2022. One of the researchers (SB) did data collection, and adequate privacy was ensured for the participants. Sixty-eight couples were approached for inclusion in the study. Eighteen couples were excluded due to various reasons (seven patients had comorbid substance use disorder apart from tobacco use disorder, five patients and three spouses had comorbid psychiatric or medical illness, two were aged more than 50 years, and one spouse had a substance use disorder apart from tobacco use disorder). Hence, 50 couples were finally included (25 in the ADS group and 25 in the ODS group). The study was done following the principles enshrined in the Declaration of Helsinki.
Instruments
Maudsley Addiction Profile: This is a brief, interviewer-administered questionnaire developed in 1998. It measures problems in four domains: substance use, health risk behavior, physical and psychological health, and personal/social functioning. Test-retest reliability is good, with highly satisfactory concurrent validity. 19 It is a public domain research instrument, and individual domains can be applied. Based on the study’s requirements, the psychological part of the health symptoms and personal/social domains of functioning was applied.
Marital Adjustment Questionnaire: Kumar and Rohatgi developed this questionnaire in 1976 to provide a handy tool to identify couples with poor marriages who need help. 20 It consists of 25 highly discriminating yes-no-type items. Personality qualities, emotional factors, marital role and responsibility factors, in-law relationship, attitude toward family plan- ning and children, interpersonal relationships, and economic, religious, and social factors are included. Three questionnaire domains are described: sexual, social, and emotional.
Eysenck Personality Questionnaire: This questionnaire was developed by Eysenck et al. in 1985. It is a 48-item yes-or-no self-administered questionnaire to assess a person’s personality traits, usually called temperament. It includes four scales: psychoticism or tough mindedness, extraversion, neuroticism or emotionality, and lying. Reported reliabilities of the Hindi version are available. 21 The time required per person is about 30 minutes.
Social Support Questionnaire: The Hindi version of the original social support scale was tried out on an Indian population by Nehra et al. 22 The questionnaire has 18 items and takes about 10 minutes to administer. After due modification, its internal consistency, reliability, and concurrent validity were established. Relative reliability was highly significant and satisfactory (r = 0.59, p < .01).
Statistical Analysis
Frequencies, percentages, means, and standard deviations were used for descriptive statistics. The difference in MAQ scores between patients and spouses of patients with alcohol and opioid dependence syndrome was assessed using the Student’s t-test or Mann–Whitney U test (due to the low sample size). The correlation between the MAQ scores between patients and their respective spouses of the same group was assessed using Spearman’s rank correlation. A p value of less than .05 was considered significant.
Results
Table 1 shows the demographic and clinical characteristics of both groups. The mean age of patients and spouses in the ADS group was higher than in the ODS group. Patients and spouses in the ADS group were more likely to attain a higher educational status than those in the ODS group. A greater proportion of patients followed Hinduism in the ADS group.
Socio-demographic Characteristics of the Sample.
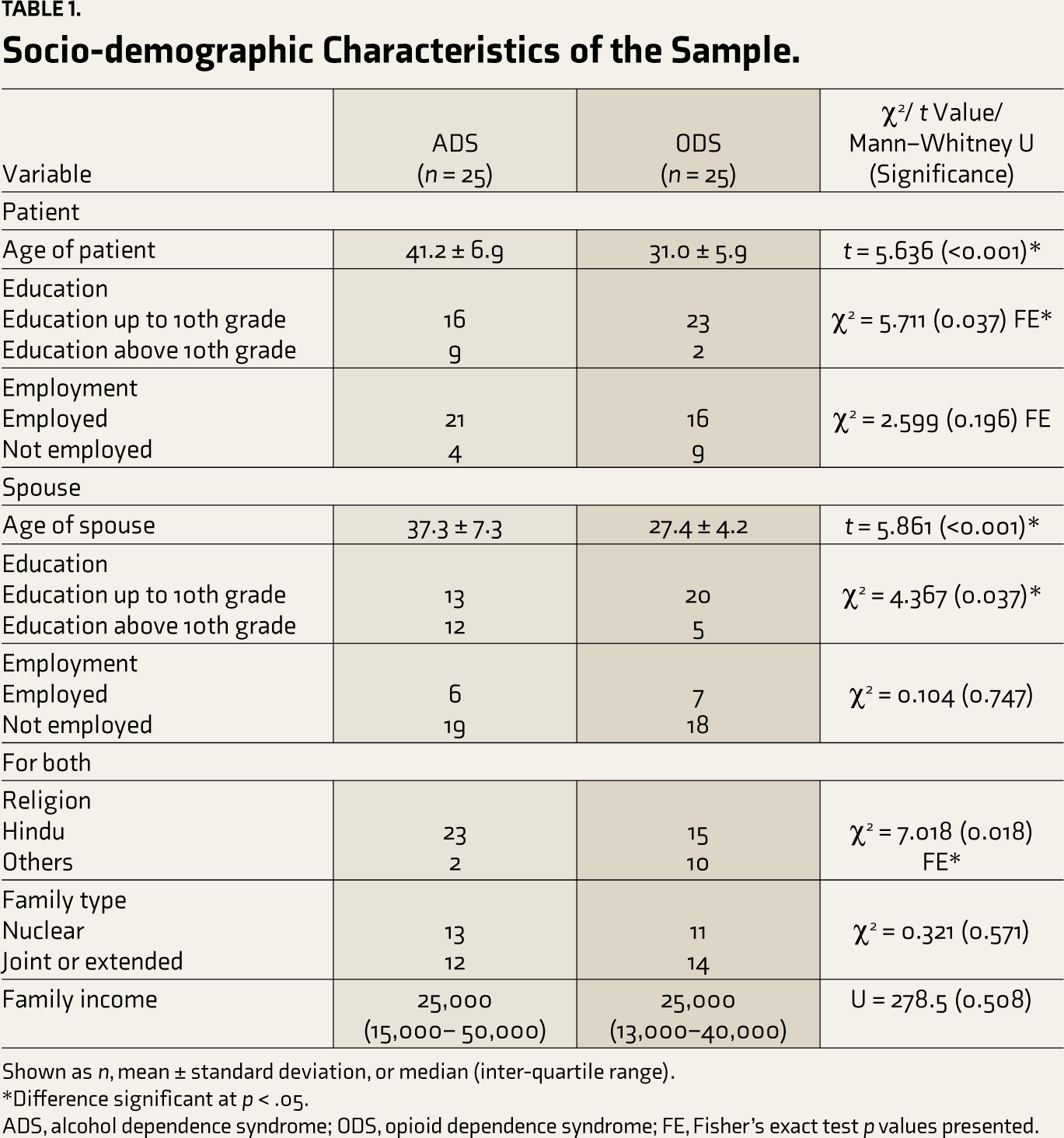
Shown as n, mean ± standard deviation, or median (inter-quartile range).
*Difference significant at p < .05.
ADS, alcohol dependence syndrome; ODS, opioid dependence syndrome; FE, Fisher’s exact test p values presented.
The substance use history of the participants is presented in Table 2. The duration of substance use and the interval between initiation of substance use and seeking treatment for the first time was longer by more than a decade in patients in the ADS group as compared to patients in the ODS group, with the difference being statistically different. In patients with ADS, more than two-thirds had comorbid tobacco use disorder, while all the patients in the ODS group had comorbid tobacco use disorder, with the difference being statistically significant between the two groups. The patients of ADS and ODS gave comparable answers to the questions regarding experiencing any emotional and psychological symptoms and personal or social functioning.
Substance Use Details and Maudsley Addiction Profile.
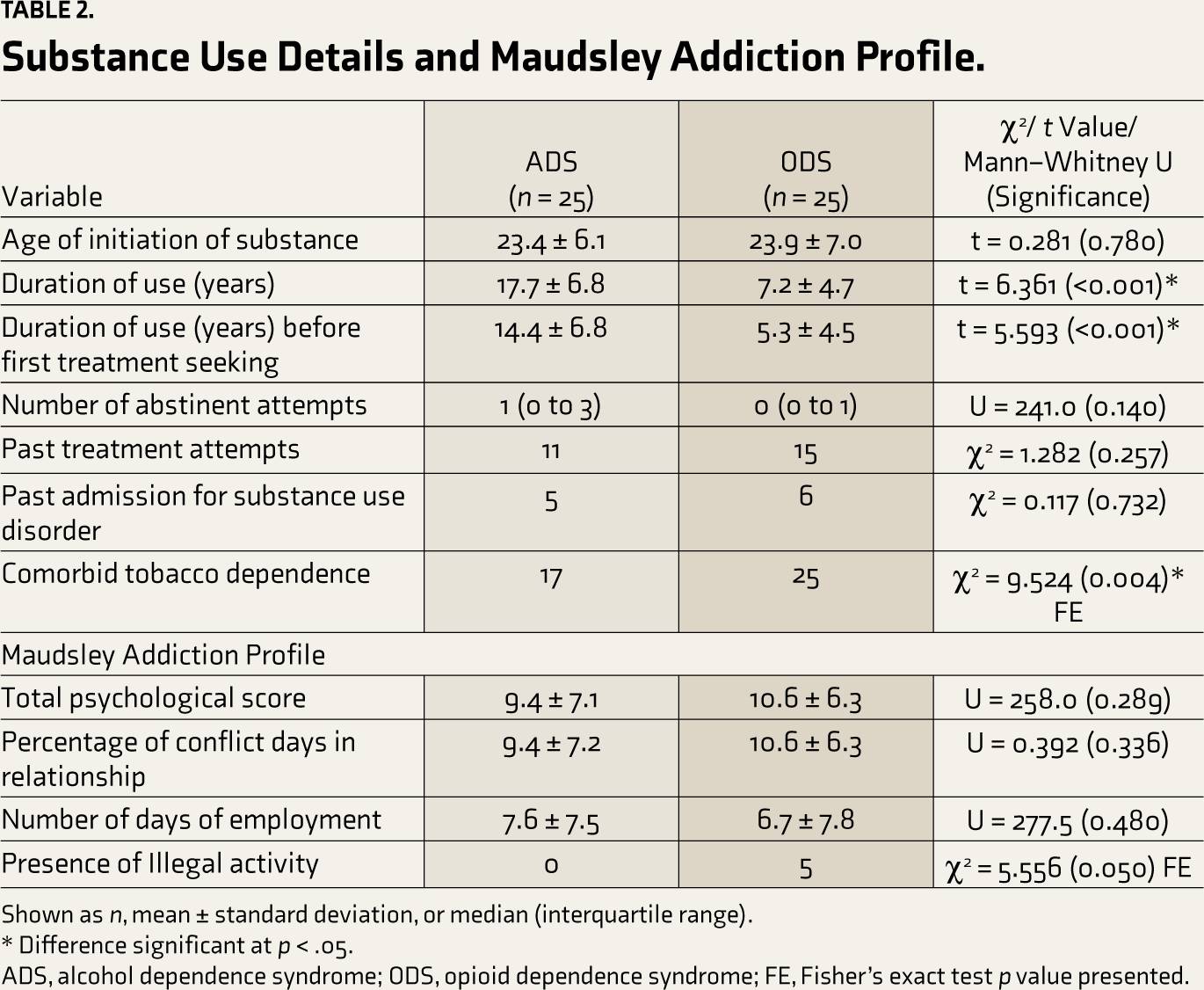
Shown as n, mean ± standard deviation, or median (interquartile range).
* Difference significant at p < .05.
ADS, alcohol dependence syndrome; ODS, opioid dependence syndrome; FE, Fisher’s exact test p value presented.
The marital aspects of the participants are presented in Table 3. The duration of marriage was significantly higher in the dyads of the ADS group than those of the ODS group. The MAQ scores of the patients and spouses of the ADS and ODS groups were comparable. The personality profile of the patients and the social support of the patients and spouses are presented in Table 4. There was no significant difference between the patients in the ADS and ODS groups, though the extraversion in the ODS group higher at a trend level significance. The social support perceived by the patients and spouses in the ADS and ODS groups was similar.
Marital Characteristics and Marital Adjustment Questionnaire.
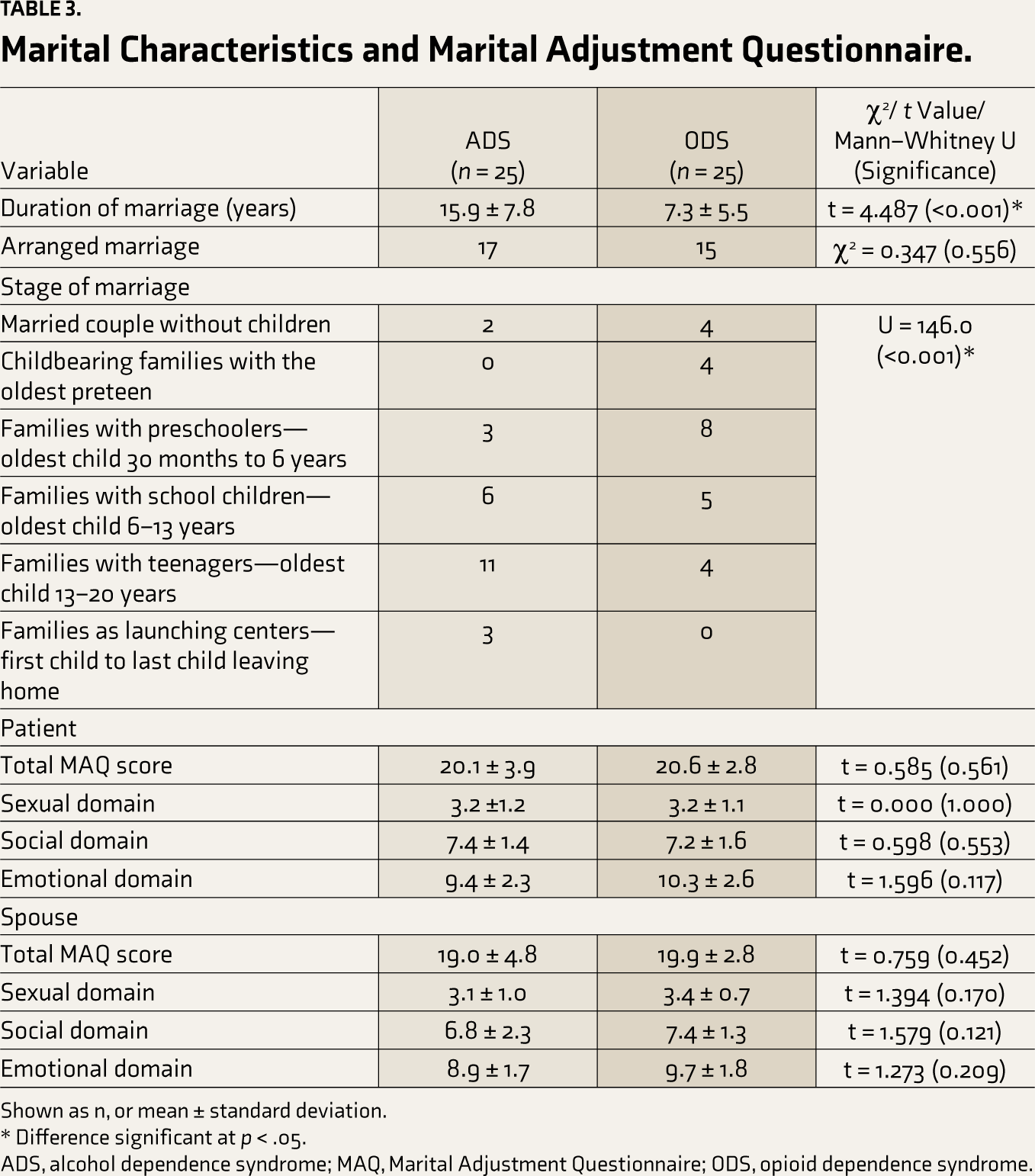
Shown as n, or mean ± standard deviation.
* Difference significant at p < .05.
ADS, alcohol dependence syndrome; MAQ, Marital Adjustment Questionnaire; ODS, opioid dependence syndrome.
Personality and Social Support Among Patients and Spouses.
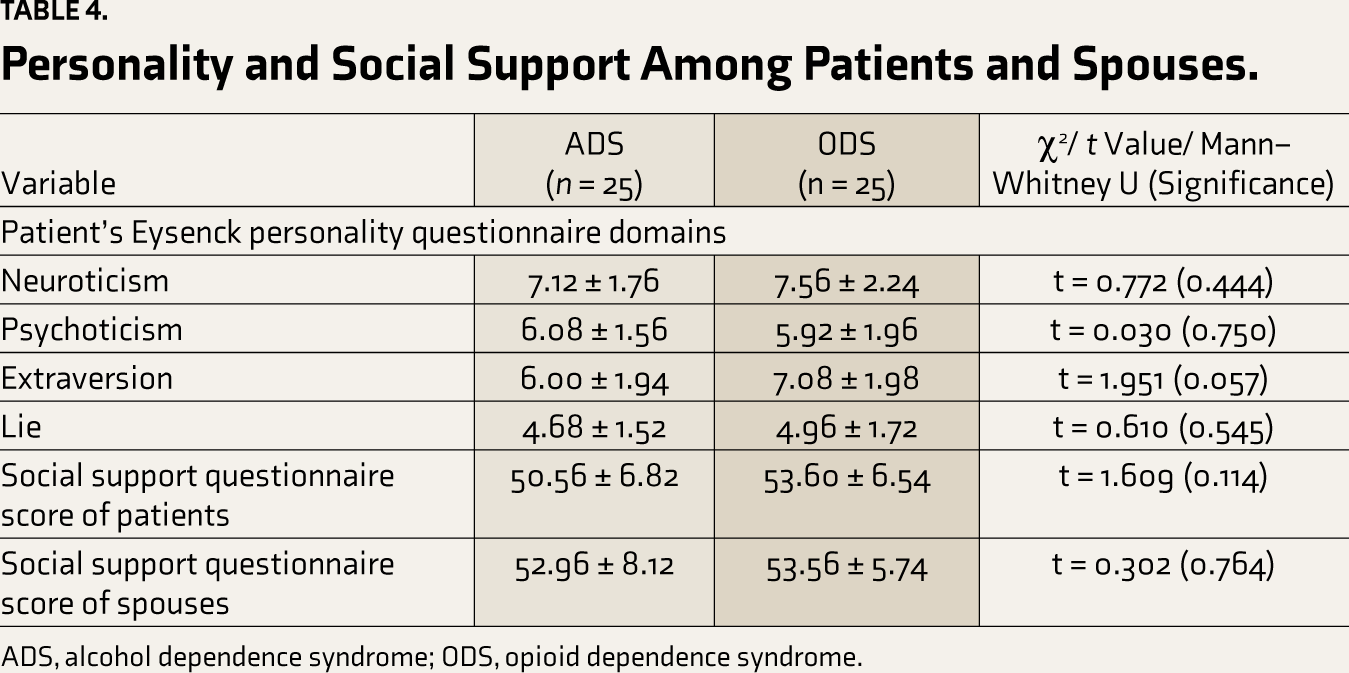
ADS, alcohol dependence syndrome; ODS, opioid dependence syndrome.
Patients’ total and domain-wise MAQ scores and those of their respective spouses were assessed for correlation. There was a statistically significant correlation between the scores of the sexual domain of MAQ of patients in the ADS group and their respective spouses (r = 0.655, p <0.001). Other correlations were not significant. The correlation between the MAQ total scores and other variables is shown in Table 5. The duration of substance use was associated with marital adjustment among spouses of opioid-dependent men. Otherwise, marital adjustment was not significantly associated with the patient’s or spouse’s age, duration of the marriage, personality profiles of the patient, and perceived social support.
Correlation of Marital Adjustment Questionnaire Total Scores and Other Variables.
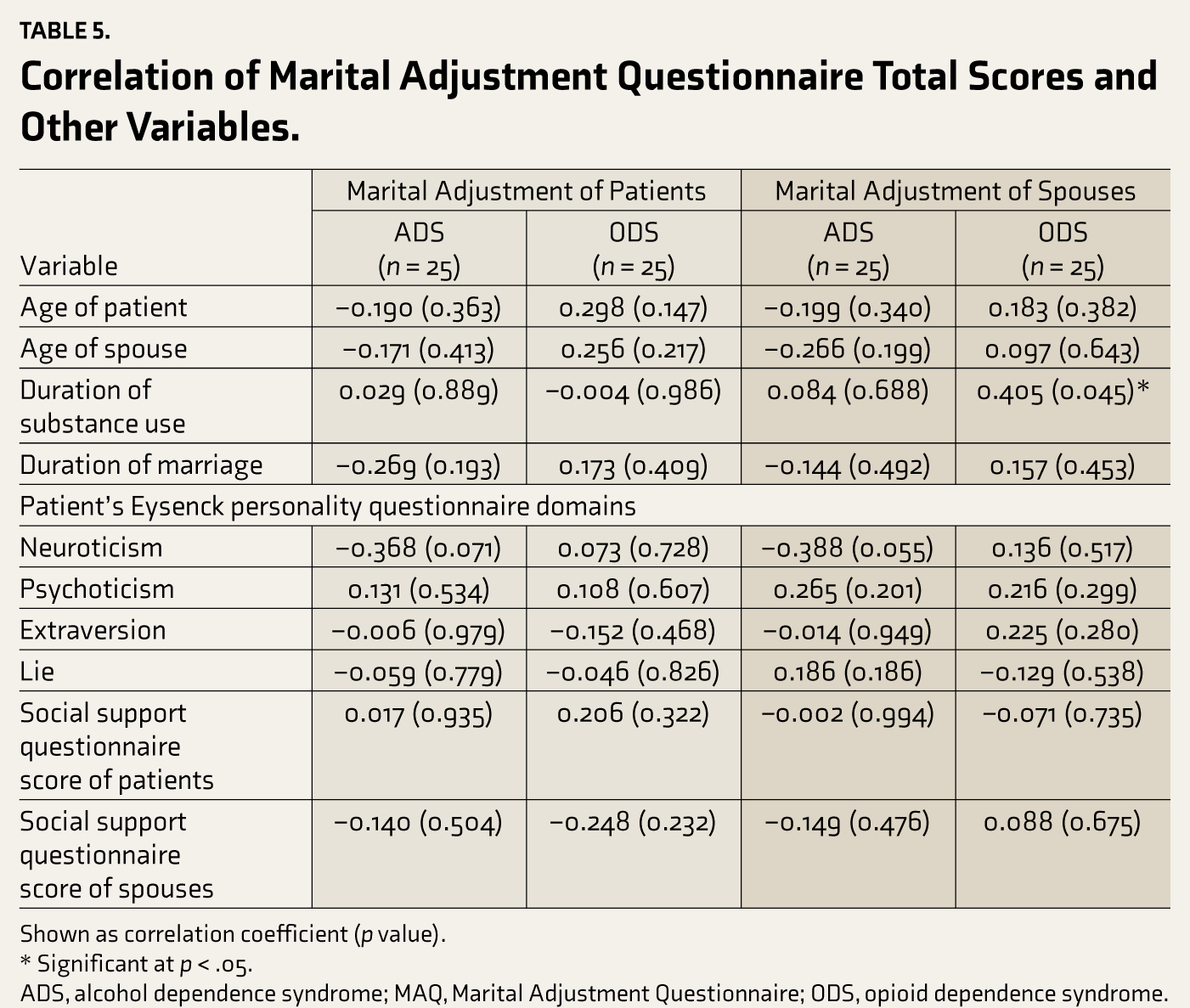
Shown as correlation coefficient (p value).
* Significant at p < .05.
ADS, alcohol dependence syndrome; MAQ, Marital Adjustment Questionnaire; ODS, opioid dependence syndrome.
Discussion
The present study suggests that the marital adjustment of patients with ADS did not significantly differ from that of patients with ODS. Additionally, the personality profiles of patients with ADS and ODS did not demonstrate a significant difference, and the personality did not have a significant relationship with marital adjustment. The mean total MAQ score of ADS patients in our study was 20.1; in ODS patients, it was 20.6 (as depicted in Table 3). The marital adjustment was much higher than those reported by Nayak and Singh, who reported a mean total MAQ score of 12.7 23 among alcohol-dependent individuals; Ranjan and Kumar, who reported a mean MAQ score of 12.4 among individuals with alcohol dependence; 24 Fatima et al., who reported a mean MAQ score of 12.5 among patients with alcohol dependence, 25 and Muke et al., who reported a mean total MAQ score of about 17.3 in a group of substance-dependent individuals. 26 Dhembare and Khan, on the other hand, reported a mean total MAQ score of 28.6 among individuals with alcohol dependence, which was much higher than reported in our study. 27 In comparative studies with alcohol-dependent individuals, the healthy control group had much higher marital adjustment than the control group.12, 23–25, 27 The adjustment scores were comparable to or slightly lower than those in the control groups or general populations, as reported in the studies of Saheba, 28 Khatri, 29 and Kumar and Trivedi. 30 We could find only one comparable literature providing quantitative estimates of marital adjustment among opioid-dependent individuals on methadone maintenance, where the authors reported a comparable mean marital adjustment score of 21.2. 31
The study provides a relationship of marital adjustment perceived by patients and their spouses. The mean scores of marital adjustments of patients and spouses were largely similar (as depicted in
The marital satisfaction was not related to the personality of the patient with substance use disorder as measured with the Eysenck Personality Questionnaire. There is evidence of the relationship between personality features (for example, neuroticism) and appraisal of marital adjustment. 33 However, the lack of a relationship in the present study may inform future researchers. Similarly, social support was unrelated to marital satisfaction, though it has been discussed as one factor affecting it. 34
Some aspects of the demographics of the sample deserve mention. The sample of patients comprised exclusively males (and spouses of females). This reflects the large proportion of treatment seekers being males in the present setting and the region.35, 36 Furthermore, the age of the patients with opioid dependence was much lower than the age of patients with alcohol dependence. This mimics the typical ages of the patient population in our setting, 37 which might be influenced by the longer time in the progression of alcohol dependence.
The implications of the present study lie in providing some guidance to clinicians about marital adjustment being similar among patients with alcohol dependence and opioid dependence. Also, appraisal of marital satisfaction is markedly different between the substance-using husband and the spouse, necessitating looking at marital adjustment from different lenses, including systemic approaches, role theory, equity theory, feminist perspective, and others. Researchers may look at marital adjustment cross-culturally and in the context of evolving societal perspectives and relationships. Marital adjustment may influence the efficacy of treatments (positively or negatively) and may be taken into cognizance in the therapeutic processes.
To the best of our knowledge, this is one of the few studies comparing marital adjustment between the two most common substance-dependent patients and their spouses nationally as well as globally. The study has a few limitations. The sample was convenient; thus, the possibility of selection bias cannot be excluded. The sample size needed to be bigger, which may have constrained the power of the study. A formal sample size estimation was not done for this exploratory study, and the sample size was based on feasibility. The present study was a single hospital-based research; only those patients who came for treatment were included, and thus, it may not represent the community-based population. The ages of the participants in the ADS and ODS groups were different. A healthy control group was lacking to compare the findings with the normal population. We did not control for multiple corrections while testing the correlations. There could be many other confounders that could not be controlled for, though we had checked for the association of marital adjustment with several variables in our exploratory analyses. Lastly, the study can provide insights about participants with an “intact” marriage. It is possible that many patients with ADS or ODS had difficult marriages and poor marital adjustment and consequently parted ways.
Within its limitations, the current study explores marital adjustment in patients with ADS or ODS as well as their spouses. The perception of marital adjustment may be quite different between patients with substance use disorders and their spouses. Also, the duration of marriage may not lead to better marital adjustment per se. The findings from this study can be utilized to develop future studies with larger sample sizes (based on present findings, the sample required to detect a difference would be 545 in each group using post hoc sample size calculation). Studies can also look at changes in marital adjustment with substance use parameters in follow-up naturalistic or interventional designs. The multiplicity of factors that may affect marital adjustment can also be assessed among individuals with substance use disorders.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The work was carried out after getting approval from the institutional ethics committee of AIIMS, New Delhi (Reference no IECPG-2/27.01.2021 dated 28.01.2021).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Participants were selected and recruited after obtaining written informed consent