
Abstract
Background:
Individuals with opioid dependence experience stigma and discrimination. Stigma can potentially reduce treatment-seeking and negatively affect treatment outcomes. We aimed to study the course of stigma and its correlates among patients receiving opioid agonist treatment (OAT).
Methods:
We recruited 51 subjects (aged between 18 and 45 years) registered in the OAT clinic from February to September 2019. We excluded subjects dependent on alcohol and other drugs (except for cannabis and tobacco), with severe mental illness, intellectual disability, and organic brain disease. We assessed the internalized and enacted stigma and quality of life at the treatment entry and after 3 months. Relationship of stigma with quality of life, socio-demographic, and other clinical variables were examined at the treatment entry.
Results:
Mean age of the subjects was 26.7 (± 5) years. At the end of three months, 33 (64.7%) patients were retained in the treatment. Internalized stigma correlated negatively with the social and environmental domains of quality of life. The strength of the correlations was modest. No significant correlation was found between demographic and clinical variables and internalized stigma and enacted stigma scores. Both internalized and enacted stigma scores reduced significantly at 3 months follow-up. The significance levels were retained even after controlling for the baseline quality of life scores. Stigma at the treatment entry did not predict early dropout.
Conclusion:
Despite higher severity at the treatment entry, the level of internalized and enacted stigma reduced significantly within three months of an outpatient-based OAT program.
Key Messages
Stigma and discrimination are common in individuals with opioid use disorder.
In patients on opioid agonist treatment (OAT), internalized stigma had modest negative correlation with the social and environmental domains of quality of life.
Internalized stigma and enacted stigma scores reduced significantly at the follow-up assessment in patients on the OAT, suggesting a possible role of OAT in stigma reduction.
The National Institute of Drug Abuse (NIDA) has included understanding and reducing stigma as one of the strategic plans to meet the public health challenges of drug use disorders (DUD). 1 Stigma can exist at the individual, institutional, and community levels. 2 At the individual level, stigma might affect the willingness to seek treatment or remain in the treatment; at the institutional level, it could reduce the motivation of policymakers and treatment providers to allocate resources and time; finally, at the community level, stigma might negatively influence the public perception and attitude toward people with DUD. 3 Stigma at the institutional and community levels gives rise to enacted stigma, that is, direct experience of discrimination and rejection from the broader community.4,5 Self or internalized stigma is a by-product of the public stigma and associated discriminatory practices. Social and economic structures and public awareness and perception differ significantly across countries. Hence, the level and nature of stigma might also vary accordingly. However, research on stigma in patients with DUD has been primarily limited to developed countries and most are cross-sectional studies. 3 Stigma for DUD might reduce, following the interventions. 6 However, the literature on the effect of the interventions is limited to self-stigma. All three published studies are from the USA, and two of these were published in the late 1960s.7–9 This research suggested that drug education, with the depiction of positive stories of recovery and therapy, conducted in a group setting, might reduce the level of stigma following treatment.7,8
Opioid use disorders account for more than 80% of the healthy life lost because of premature deaths and disability, and 66% of mortality attributed to DUD. 10 Opioid agonist treatment (OAT) or medication-assisted treatment for opioid use disorders could reduce the odds of mortality, morbidity, and relapse to illicit drug use.11,12 Despite the evidence of efficacy, OAT is grossly underutilized: globally, less than 10% of those in need of treatment receive OAT. 13 Reasons cited for this underutilization include stigma- impacting treatment-seeking, reluctance to use OAT by healthcare providers, and resistance from the patients' family or 12-step programs. 14
Research on correlates of stigma experienced by individuals with opioid dependence consistently demonstrated an association of stigma with the quality of life (QoL). The locality, socioeconomic and educational status, and the duration of drug use were some other demographic and clinical correlates of stigma.15–17
We hypothesized that over time, OAT would reduce the stigma among individuals with opioid dependence. The study’s primary objective was to examine the change in the levels of internalized and enacted stigma among patients with opioid dependence over three months of buprenorphine-based agonist treatment. The secondary objectives were to explore the correlates of baseline levels of stigma and sociodemographic variables (such as age, locality, education, and socioeconomic status) and clinical variables (such as duration of opioid dependence and presence of cannabis dependence and medical disorders), and to assess the relationship between baseline stigma and QoL with treatment dropout.
Methods
Study Sample and Design
Patients registered in the OAT clinic were recruited consecutively between February and September 2019. A written informed consent was obtained from all the participants. It was a prospective study and the participants were assessed twice: at the treatment entry (within one week of initiation of OAT) and at the end of three months (± two weeks) of OAT. The Institutional Ethics Committee approved this study.
Sample Size Calculation
The study’s primary objective was to examine the changes in the level of stigma. Hence, the sample size calculation was based on the changes in the scores on internalized stigma between the treatment entry and at the end of three months. The study would require a sample size of 27 (number of pairs) to achieve a power of 90% and a level of significance of 5% (two-sided) for detecting an effect size of 0.67 between pairs. The effect size was based on a previously published study. 9 Assuming 40% dropout, we intended to recruit 50 patients.
Selection Criteria
We included patients with opioid dependence aged 18 to 45 years. A total of 51 participants were recruited. We excluded patients with alcohol dependence but not those with tobacco and/or cannabis dependence. The reason for retaining tobacco and cannabis dependence was the high comorbidity of these disorders with opioid dependence; hence, excluding these participants would have compromised the study’s generalizability.18,19 Patients with HIV, hepatitis C, or other medical comorbidities were also included. However, patients with severe mental illness, intellectual disability, or organic brain disease were excluded. The study flow diagram is given in Figure 1.
Opioid Agonist Treatment Program
The multidisciplinary team of the OAT program consisted of two psychiatrists, a psychiatric social worker, a trained addiction counselor, and a nursing officer. The psychiatrists were responsible for initial evaluation, intake, and periodic monitoring of all patients. Comorbid psychiatric disorders and medical illnesses, too, were dealt with by the psychiatrists. We administered the buprenorphinenaloxone fixed-dose combination as the outpatient OAT program. Medications were dispensed for one week. We followed the principle of recovery-oriented OAT, aiming at the final goals of voluntary sobriety, citizenship, and personal health. All patients on OAT participated in weekly, open, group sessions of 45 to 60 minutes. The content of the group sessions consisted of psychoeducation on medical models of opioid dependence, management of craving, stress and anger management, and advice for positive lifestyle changes. Members were also encouraged to talk about their recovery goals, problems in achieving those, and experience with the OAT. The groups were led by trained psychiatric social workers or addiction counselors. Families of the patients were involved during the detailed evaluation and initiation of OAT. They were informed about the medical model of opioid dependence, OAT, and plan of treatment. They were encouraged to accompany the patients to the clinic at least once a month. During their visits, the counselors asked about their views of the patient’s improvement in clinical and functional status and discussed practical difficulties experienced by them and their solutions.
Assessment Tools
Sociodemographic Profile
The socioeconomic status was calculated according to the updated version of the Kuppuswamy’s scale, which involves the measurement of three parameters: occupation and education of the head of the family and income of the patient. 20
Internalized Stigma of Substance Abuse (ISSA)
The Internalized Stigma of Substance Abuse (ISSA) scale was adapted from the 29-item Internalized Stigma of Mental Illness scale, which has been used in the Indian context.21,22 It assesses internalized stigma and perceived public stigma. It has high internal consistency for three subscales assessing aspects of self-stigma (alienation, stereotype endorsement, stigma resistance) and two subscales assessing aspects of perceived public stigma (perceived discrimination and social withdrawal). Overall, the internal consistency reliability coefficient (alpha) is 0.90 and the test–retest reliability coefficient, 0.92. 21
The Substance Use Stigma Mechanism Scale (SU-SMS)
This was derived from the HIV Stigma Mechanism scale and has been validated in patients on methadone maintenance treatment. It measures enacted stigma in the context of the family and health care professionals and has high internal consistency (alpha = 0.90). 23 A theory-based scale, it was initially validated in a diverse sample, and later, its Turkish version, too, was developed with excellent psychometric property.23,24 Therefore, the application of SU-SMS is unlikely to have a cultural influence.
WHO Quality of Life-BREF (WHOQOL BREF)
Hindi version of this instrument was used to assess the QoL. The WHO-QOL-BREF contains 26 questions, four domains (physical health, psychological health, social relationship, and the environment), and 24 facets. 25
Statistical Analysis
Statistical analysis was carried out using SPSS version 21 (IBM Corp., Armonk, NY, USA). 26 Demographic and clinical variables were represented using descriptive statistics (e.g., frequencies and percentages for categorical variables and mean-standard deviation for continuous variables). The change in the levels of stigma (both subtypes) between baseline and after three months of OAT was compared using paired t-test. Pearson’s correlation coefficient was used to study the correlation between the QoL and stigma scores, while Spearman’s correlation coefficient was used to study the correlation between stigma and socioeconomic status and educational qualification. Correlations between stigma scores and locality, medical disorders, and cannabis dependence were tested by point-biserial correlation. General linear model analysis was performed with the follow-up stigma scores as dependent variables and WHOQOL-BREF score as a covariate. Finally, we tried to examine the relationship between baseline stigma scores and treatment drop out using binary logistic regression analysis. The tests were two-tailed. P-value of < 0.05 was set as the cut-off for the level of significance.
Results
Participants’ Demographic and Clinical Characteristics
A total of 51 participants were recruited. Thirty-three (64.7%) were retained at the end of three months. The mean (± SD) age of the participants was 26.72 (± 4.97) years (range: 18–41 years, median: 25 years). Heroin (80.4%) was the most commonly used opioid, and the predominant route of administration was intravenous (80.4%). Please see Table 1 for the detailed clinical and demographic characteristics.
Socio demographic and clinical profile of the participants
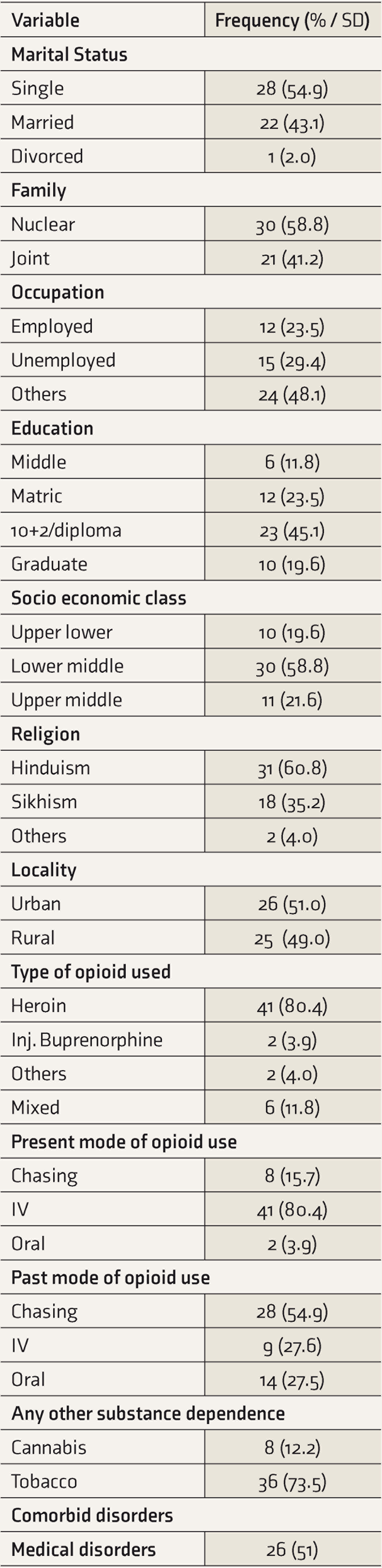
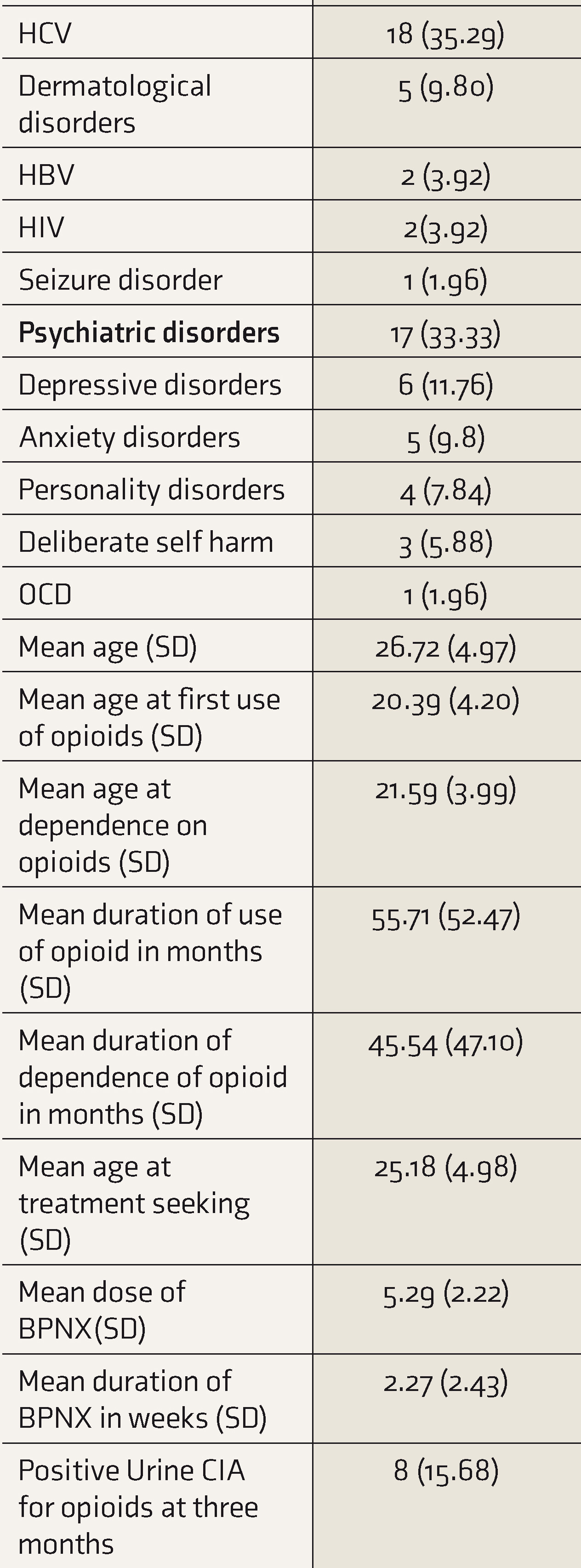
BNX: Buprenorphine-naloxone fixed dose combination; CIA: Chemiluminescence immunoassay HBV: Hepatitis B Virus infection; HCV: Hepatitis C Virus infection; HIV: Human Immunodeficiency Virus infection; IV: Intravenous; OCD: Obsessive Compulsive Disorder; SD: Standard Deviation
Correlation of participants’ level of stigma, domains of Quality of life, and other clinical variables (N=51)

QoL: Quality of Life, * Pearson correlation, ** Spearman’s correlation, # point bi-serial correlation
Change in the level of Stigma over the 3-months of treatment

(Multivariate analysis:- Dependent Variable: Follow up stigma scores, Covariate: baseline quality of life)
Stigma-Profile of the Participants at the Baseline and After Three Months of Treatment
The most frequently reported stigmatized experiences were seen in the alienation domain of the Internalized Stigma scale. This was followed by domains in stereotype endorsement, discrimination experience, and the least scores were in stigma resistance. At baseline, 96% reported that having a substance abuse problem spoiled their lives, and this reduced to 63.1% at the follow-up. On initial assessment, 84.3% of participants accepted that stereotype about people with Substance Use Disorders (SUD) applied to them, which reduced to 54.6% on follow-up. Initially, 82.7% of participants agreed that people with SUD could not live a good rewarding life, which reduced to 48.5% on follow-up. Also, 84.3% of patients agreed that people thought they could not achieve much in their lives, while 48.3% of participants reported being discriminated because of their substance use. At follow-up, both these statements were endorsed by 45.4% of participants.
For enacted stigma, at initial assessment, 64.7% agreed that their family members thought that they were not trustworthy, which reduced to 36.4% at follow-up. The baseline assessment revealed that 13.8% perceived that health care workers did not listen to their concerns. However, none of the participants endorsed this item at the follow-up assessment.
Correlation of Stigma and Demographic and Clinical Variables
As depicted in Table 2, there was no significant correlation between age of patients, duration of opioid dependence, presence of comorbid medical /psychiatric disorder, socioeconomic status, or locality with total ISSA score or enacted stigma scores. Internalized stigma scores of the patients correlated negatively with the social and environmental domains of QoL (r = –0.45, P = 0.001 and r = –0.43, P = 0.001, respectively).
Change in the Level of Stigma Over Three Months of Treatment
Stigma scores at the baseline and at three months were compared using paired t-test. At baseline, internalized stigma scores were 53.48 ± 11.62, which reduced significantly to 36.18 ± 15.11 at follow-up (P < 0.001). At follow-up, enacted stigma reduced significantly compared to baseline scores (14.94 ± 4.38 vs. 11.39 ± 36). The effect sizes measured by Cohen’s d were 0.93 and 0.74 for internalized and enacted stigma, respectively.
In the general linear model, follow-up stigma scores were entered as dependent variables, and the total baseline QoL score was entered as a covariate. The enacted and internalized stigma scores were entered into two different models. The results revealed that the reductions in both the internalized stigma as well as enacted stigma at the three months follow-up were statistically significant (P < 0.01 and P = 0.04, respectively). The effect sizes, measured by adjusted partial eta Squared, were small: 0.22 and 0.07, respectively, for internalized and enacted stigma.
The total QoL score at the treatment entry (71.07 ± 9.63) improved significantly (df = 32, t = –9.24, P < 0.001) at three month follow-up (90.36 ± 10.49).
We used binary logistic regression to examine the effect of baseline stigma on early dropout from treatment (those who dropped out within three months of starting OAT). Retention on treatment was entered as the dependent variable, while scores on stigma in various scales and QoL were included as independent variables. As shown in Table S1, none of these variables could predict the initial dropout.
Discussion
This was an exploratory study to examine the level of stigma experienced by patients with opioid dependence and to observe the change in stigma among this group of patients three months after the initiation of OAT. We also explored the sociodemographic and clinical correlates of stigma. We adjusted for possible confounding factors to discern whether the change in the level of stigma was independent of the QoL (which had a significant association with stigma-level at the treatment entry).
Our study revealed (a) high internalized (self) and public stigma among patients with opioid dependence, (b) a significant reduction of both self and public stigma after three months of OAT, the change in the level of stigma retaining statistical significance even after adjusting for the baseline QoL, (c) internalized stigma having a modest and significant negative correlation with social and environmental dimensions of the QoL, and (d) stigma during treatment entry not predicting early dropout from the treatment program.
The high level of internalized stigma spanned all five dimensions: alienation, stereotype endorsement, the experience of discrimination, social withdrawal, and stigma-resistance. Previous studies from elsewhere, too, showed high self or perceived stigma in patients with opioid dependence and DUD.5,27–31 Except for one study from China, all others were from the USA, Europe, and Australia. The only other study from India, with a mixed group of the substance-dependent population, also revealed that a substantial majority (more than 60%) of patients had “severe” internalized stigma. 16 Having a similar finding in our study from India suggests the cross-cultural occurrence of self-stigma among patients with DUD. In addition to internalized stigma, our patients experienced stigma at the level of family, society, and health care services. However, compared to studies from the developed countries, the severity of public stigma appeared to be less. 32 Possible reasons for this are (a) the Indian society is collectivistic and, therefore, might be more tolerant to deviation. All our patients, despite having interpersonal problems, lived with the family members. (b) Studies from different parts of India in primary health care settings revealed that more than 80 percent of the clients were satisfied with the general experience, behavior, and treatment provided by the health care workers. This positive rating was despite patients’ discontent with the physical environment.33,34 We could not find any published literature among patients with substance use disorders. Nevertheless, from our personal experience and extrapolating from the aforementioned research, we believe that the Indian patients, generally, might have lower expectations, higher tolerance, and a “less demanding” nature. Therefore, the lesser level of stigma from health care professionals should be interpreted in light of the patients’ expectations in the Indian context. The modest and significant positive correlation between self and public stigma shows the interdependent nature of these constructs. 35
The level of internalized (self) stigma correlated significantly with the social and environmental dimensions of the QoL, that is, patients with higher perceived social and environmental restrictions had higher internalized stigma. The absence of a significant correlation was reflective of the varying constructs of the physical health dimension of QoL and dimensions measured by the internalized stigma scale. A previous study, however, showed that opioid-dependent patients with severe internalized stigma had significantly lower scores in all dimensions of QoL. 16 Unlike those researchers, we did not classify the patients based on their level of internalized stigma. Besides, the other study assessed internalized stigma with the Internalized Stigma of Mental Illness Scale (ISMIS), whereas we used an instrument specific to stigma in patients with substance use disorders.
There was no correlation between the level of stigma and the duration of dependence or socioeconomic status. These results were similar to a previous study. 15
The level of self (internalized) and enacted stigma reduced significantly within three months of the OAT program. Previous studies on patients with SUD and mental illness had shown a reduction in the internalized stigma following acceptance-based treatment and psychoeducation.9,36 In addition to the pharmacological treatment with buprenorphine, the weekly group counseling sessions based on the medical model of opioid dependence, experience sharing, lessons on coping, and problem-solving might also have contributed to the improvement in the self-stigma. Nonetheless, in the absence of a controlled trial, the possibility of group sessions’ effect on self-stigma remains only speculative. Independent improvement in the public stigma was also an interesting finding. This could be explained by the following: (a) involvement of the families in the patients’ treatment, at least during the detailed intake and initiation of OAT, and periodic involvement as and when required, (b) all our health care workers were trained addiction professionals; the knowledge, training, and experience with patients on OAT could have helped reduce their negative attitudes towards patients, 37 and (c) the inter-relationship between self and public stigma, reduction of self-stigma, too, might have contributed to the improvement in the public stigma. Nevertheless, the effect size estimated for the reduction in public stigma was much less than that for self-stigma. The improvement in the QoL was in line with the existing literature that had shown that OAT improves the QoL, even in short term. 38
Finally, we wanted to see whether the patients with higher levels of stigma selectively dropped out from the treatment, spuriously suggesting the improvement of the stigma scores among retained participants. The logistic regression showed there was no relationship between the stigma at the treatment entry and dropout. Hence, the reduction of self and public stigma, shown in the results, was unlikely to be influenced by the dropout from treatment. A previous study from the USA also showed that retention in methadone maintenance treatment was not predicted by perceived stigma. 39
To the best of our knowledge, this was the first prospective study from India among patients on OAT. This has become important in the backdrop of the magnitude of problem opioid users (7.7 million) in the country, accompanied by very poor coverage of OAT (less than 20 of 100 people who inject drugs receive OAT per year).40,41 Besides, ours was one of the few studies with the objectives of assessing internalized and enacted stigma at the treatment entry and observing their changes during an OAT program. Our study was adequately powered to detect changes in the level of stigma.
Our study had some limitations, which are listed as follows: (a) all our participants were men. This was not by design, but the predominant treatment-seeking population in India is men.15,16 (b) The outcome was assessed after three months. A longer follow-up might have informed us about the persistence of the improvement in stigma. (c) We could not examine the effect of stigma on treatment-seeking because our study was done on clinic-based patients. A study in the community, among nontreatment-seeking patients, may produce a different result. Future studies could be on a larger, community sample. (d) Our study was not designed to determine the effect of OAT (and or group intervention) on stigma reduction. Only a controlled clinical trial could answer this question. (e) The tools used for the assessment of stigma in our study were not translated and validated.
Conclusion
Our study showed that, despite the higher severity at the treatment entry, the level of self and public stigma reduced significantly within three months of an outpatient-based OAT program. Improvement in self-stigma might improve other treatment outcomes and treatment persistence and help achieve the final goal of recovery. Improvement in public stigma might change the attitude of society and family toward opioid dependence and OAT. A mixed-method, controlled study could inform us regarding the effect of treatment and help us understand the treatment-related factors on the reduction of stigma.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.