
Abstract
Background:
Postpartum depression (PPD) is the commonest mental health disorder post-childbirth, yet there is a paucity of data in rural areas regarding the actual incidence of PPD, which excludes pre-existing or antenatal depression. To estimate the incidence of PPD among rural women of south Karnataka and identify predictors of PPD, including antenatal psychiatric disorders.
Methods:
A longitudinal study in 25 villages in south Karnataka among 150 pregnant women in the third trimester of pregnancy using simple random sampling. Baseline data collected and revised Clinical Interview Schedule used to screen antenatal psychiatric disorders. Participants followed-up 6–8 weeks postpartum, end-line data collected, and Edinburg Postnatal Depression Scale administered. Chi-square and Fischer’s exact tests for association between PPD and covariates. Logistic regression to calculate adjusted odds ratios.
Results:
Prevalence of antenatal psychiatric disorders was 15.3%. The incidence of PPD was 11%. A significantly higher proportion of PPD was found among women with adverse events in the last year, low socioeconomic status, and perceived lack of care/support at home. Predictors of PPD were antenatal psychiatric disorders (AOR = 4.3, 95% CI = 1.22–5.11; P = 0.028), mothers reporting worry about their infant’s health (AOR = 7.7, 95% CI = 1.22–48.32; P = 0.012) and mothers receiving postpartum care by caregivers other than their own mother (AOR = 4.0, 95% CI = 1.13–8.09; P = 0.030).
Conclusions:
Our study found that one in ten rural women is developing PPD and there is a strong link between PPD and antenatal psychiatric disorders and family factors. This calls for capacity building of general physicians and village-level workers and strengthening of the Home-Based Newborn Care Program, where weekly postpartum home visits by ASHA are an opportunity for screening and counselling mothers.
Keywords
Post-partum depression has a strong linkage between antenatal psychiatric symptoms and family factors. Screening of antepartum mental morbidities in antenatal clinics helps in identifying women at risk of developing postpartum depression. Inclusion of simple and minimal tools in the maternal and child care programme will improve the psychological quality of life of pregnant women, thereby improving the health of newborn.Key Messages:
Postpartum depression (PPD) is the most common maternal mental health disorders in the six weeks following delivery. 1 A meta-analysis of 38 Indian studies reported the pooled prevalence of PPD as 22% (95% CI = 19–25), 2 with 11% in rural Tamil Nadu 3 and 12% in rural Gujarat. 4 The spectrum of postpartum depressive disorders range from postpartum blues to PPD to postpartum psychosis. 5 For the mother, PPD can be the precursor of chronic recurrent depression. For the child, a mother’s ongoing depression can contribute to emotional, behavioral, cognitive, and interpersonal problems in later life. 6 Predictors of PPD are psychiatric disorders during pregnancy, stressful recent life events, poor social-support, marital problems, a previous history of depression, and a family history of depression. Obstetric and pregnancy complications, single marital status, poor relationship with the partner, lower income, and unplanned pregnancy are also risk factors for PPD.7–10
Common antenatal psychiatric symptoms reported are depression, anxiety, obsessive compulsive disorders, phobic reaction, somatic disturbance, excessive fatigue or irritability, and insomnia.1–3 Antenatal psychiatric disorders are associated with poor attendance at antenatal clinics, substance misuse, hypertension, low birth weight and preterm delivery, difficult labor and delivery, as well as breastfeeding difficulties, cognitive delay, and future behavioral problems for the child.11–13 Studies have shown an association between antenatal psychiatric disorders and PPD.3,6,10,14,15
Although two-thirds of the Indian population reside in rural areas, there is a paucity of literature regarding PPD in this setting. Most Indian studies have looked at the prevalence of PPD without separating pre-existing depression from that which has developed only after birth. There are very few community-based studies on the incidence of PPD in the rural Indian setting and one of them was done in a village near Delhi, where it was found that PPD was 4.4% and associated only with antenatal depression. 16 Therefore, this study was conducted with the primary objective to estimate the incidence of PPD among rural women of south Karnataka. The secondary objective was to identify predictors of PPD, including antenatal psychiatric disorders. This would help develop targeted interventions during the antenatal period to focus on mitigating risk factors to prevent the development of PPD.
Materials and Methods
Study Setting
A longitudinal study in 25 villages under Sarjapur Primary Health Centre, Anekal Taluk, Bangalore Urban District, covering a population of around 30,000, was conducted in 2017, after Institutional Ethics Committee approval. These villages are included under medical college rural field-practice area.
Study Population
Pregnant women in the third trimester residing in the study area.
Sample Size
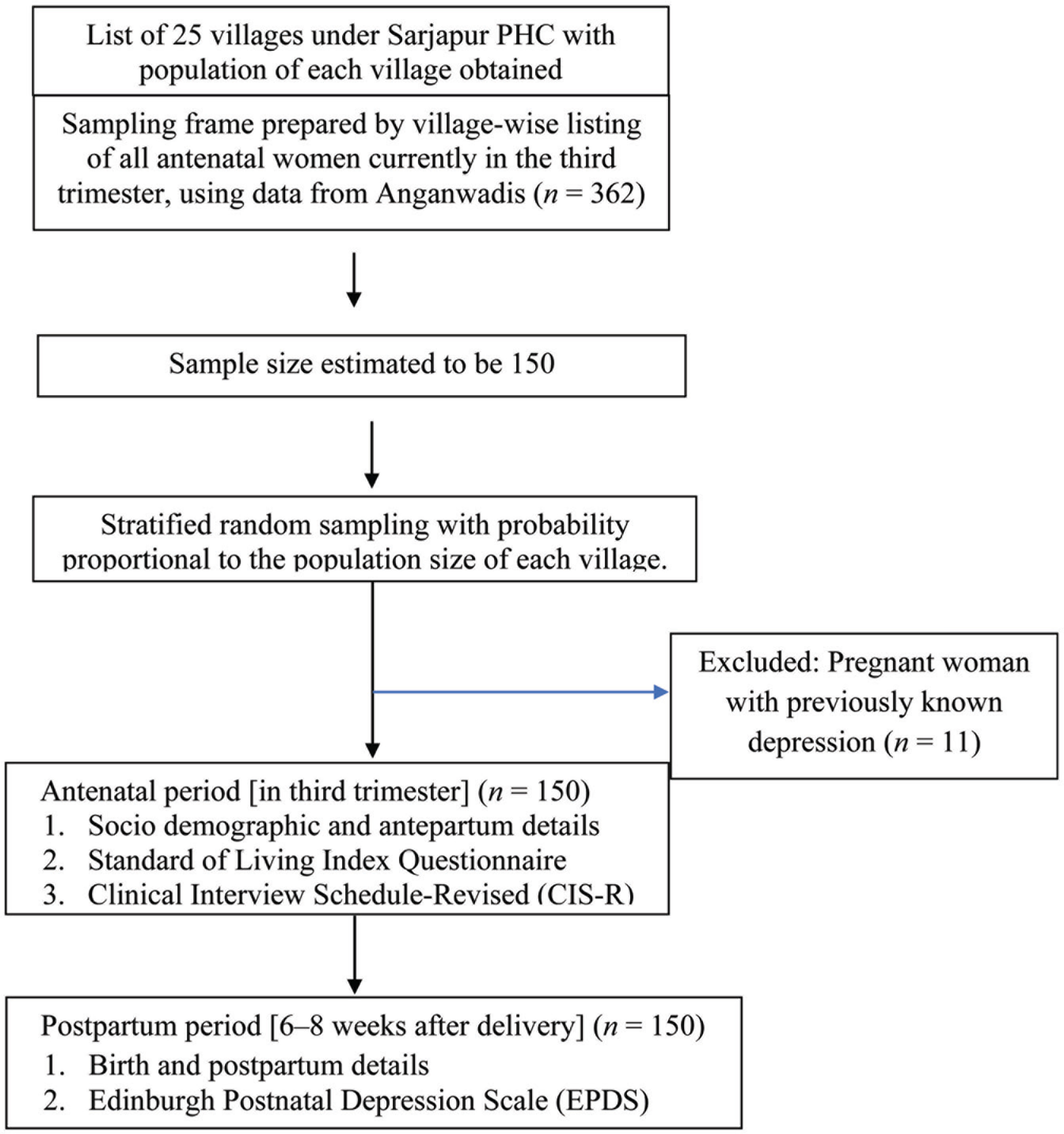
Based on a previous study in Vellore, South India, where the prevalence of PPD was found to be 11%, 3 with 5% margin of error and 95% confidence level, the sample size was calculated to be 150.
Sampling Method
Anganwadi worker in each village was contacted for the list of antenatal women currently in the third trimester, and a sampling frame was prepared. Using probability proportional to size, the study subjects were selected from each village using stratified random sampling from within this sampling frame.
Inclusion Criteria
Pregnant women who completed 28 weeks of gestation.
Exclusion Criteria
Women with a known history of depression or previously diagnosed depression; those who were seriously ill and could not comprehend the questions.
Study Tools
Structured interview schedule was prepared in the local language to capture information on sociodemographic details (age, education, occupation, and income), obstetric details (parity, mode of delivery, sex of the infant, and neonatal complications), and family factors (adverse event in last one year, perceived care and support, and caregiver other than own mother for pregnant women). It was face validated by two experts in perinatal psychiatry and pretested prior to use. Socioeconomic status was determined using Standard of Living Index. 17
Kannada-translated version of Clinical Interview Schedule-Revised (CIS-R), 18 with 14 subsections assessing common mental disorders: somatic symptoms, fatigue, concentration, sleep problems, irritability, worry about physical health, depression, depressive ideas, worry, anxiety, phobia, panic, obsessions, and compulsions, with scores for each subsection ranging from 0 to 4. The CIS-R screens for psychiatric disorder with a sensitivity of 88% and specificity of 96% at a total score of 12 or higher, 19 and has been extensively used in India.3,20 CIS-R total score of <12, but scoring on one or more subsections, may be termed as the presence of psychiatric symptoms.
The 10-item Edinburgh Postnatal Depression Scale (EPDS) 21 —Kannada-translated version screens for PPD, with a sensitivity of 100% and specificity of 85% at a score of ≥13. 22 A study in the UK has established concurrent validity of EPDS at score ≥13 with respect to CIS-R in diagnosing PPD (sensitivity 62.9%, specificity 95.7%). 23
Data Collection
Data were collected by a postgraduate student in Community Medicine, trained by a psychiatrist to administer the study tools. At the first home visit, the subject was recruited into the study with written informed consent, baseline data were collected, and CIS-R was used to screen for antenatal psychiatric disorders. The second home visit was made in the postpartum period at 6–8 weeks after delivery, at which time, birth details and postpartum history were obtained and EPDS was administered. Those who were not available for the second home visit as they had gone to their maternal home for delivery and postpartum care (10%) were contacted over the phone, and the second interview schedule was administered telephonically. Study participants with a suspected psychiatric disorder were referred to a psychiatrist for further evaluation and management at the weekly mental health clinic of the Medical College Rural Health Training Centre located in one of the study villages.
Statistical Analysis
The data collected were entered in Microsoft Excel and analyzed using IBM Statistical Package for Social Sciences version 20. The outcome variable in this study was PPD. Exposure variables were sociodemographic and obstetric factors and antenatal psychiatric disorders. The study variables were described using frequencies, proportions, mean, standard deviation, median, and interquartile range. Chi-square test and Fischer’s exact test as applicable were used to test for association between PPD and various exposure variables. Significantly associated variables were entered into a forward step type of a binary logistic regression model, and adjusted odd ratios were calculated with 95% confidence intervals. P value of <0.05 was considered significant for all statistical analyses.
Results
Sociodemographic Details
Among the 150 subjects, the women’s mean ±SD age was 23.31 ± 3.03 years. The majority 93 (62%) belonged to the age group 20–24 years (range = 18 to 36). Most 141 (94%) were homemakers and 91(60.7%) were educated up to high school, and 137 (95.3%) were Hindu by religion and belonged to middle socioeconomic status. The mean number of family members was 5 ± 3.32.
Obstetric Details
Mean gestational age was 31.17 weeks ±3.08. The majority of women, 108 (72%), reported no family pressure for a male child. Nearly 40% were primigravid. Out of 98 multigravidas, majority 89 (90.8%) had no complications in the past pregnancy and none reported a previous history of PPD. We were able to follow-up with all the 150 study subjects in the postpartum period. All the deliveries were full term (after 37 completed weeks of gestation) and singleton births. Most of the subjects 103 (68.7%) had a normal vaginal delivery, and 78 (52%) of the newborns were females. Mean birth weight was 2800 ± 320 g; 17 (11.3%) had low birth weight, i.e., <2500 g. None of the women in our study had a stillbirth, early neonatal death, or congenitally malformed baby.
Postpartum Care
No postpartum complications like postpartum hemorrhage, puerperal sepsis, postpartum eclampsia, mastitis/breast abscess, or deep vein thrombosis were experienced by the mothers. Neonatal complications, as per the Integrated Management of Neonatal and Childhood Illnesses, 24 were reported by 44 (29.3%) of the mothers, most commonly neonatal jaundice, difficult breathing, or difficulty in feeding. The majority of women, i.e., 115 (76.7%), had their own mother to take care of them in the postpartum period. Lack of care or support in the postpartum period was reported by 15 (10%) participants, and 53 (35.3%) reported being worried about the health of their infant, 47.2% of whose babies had neonatal complications.
Antenatal Psychiatric Disorders
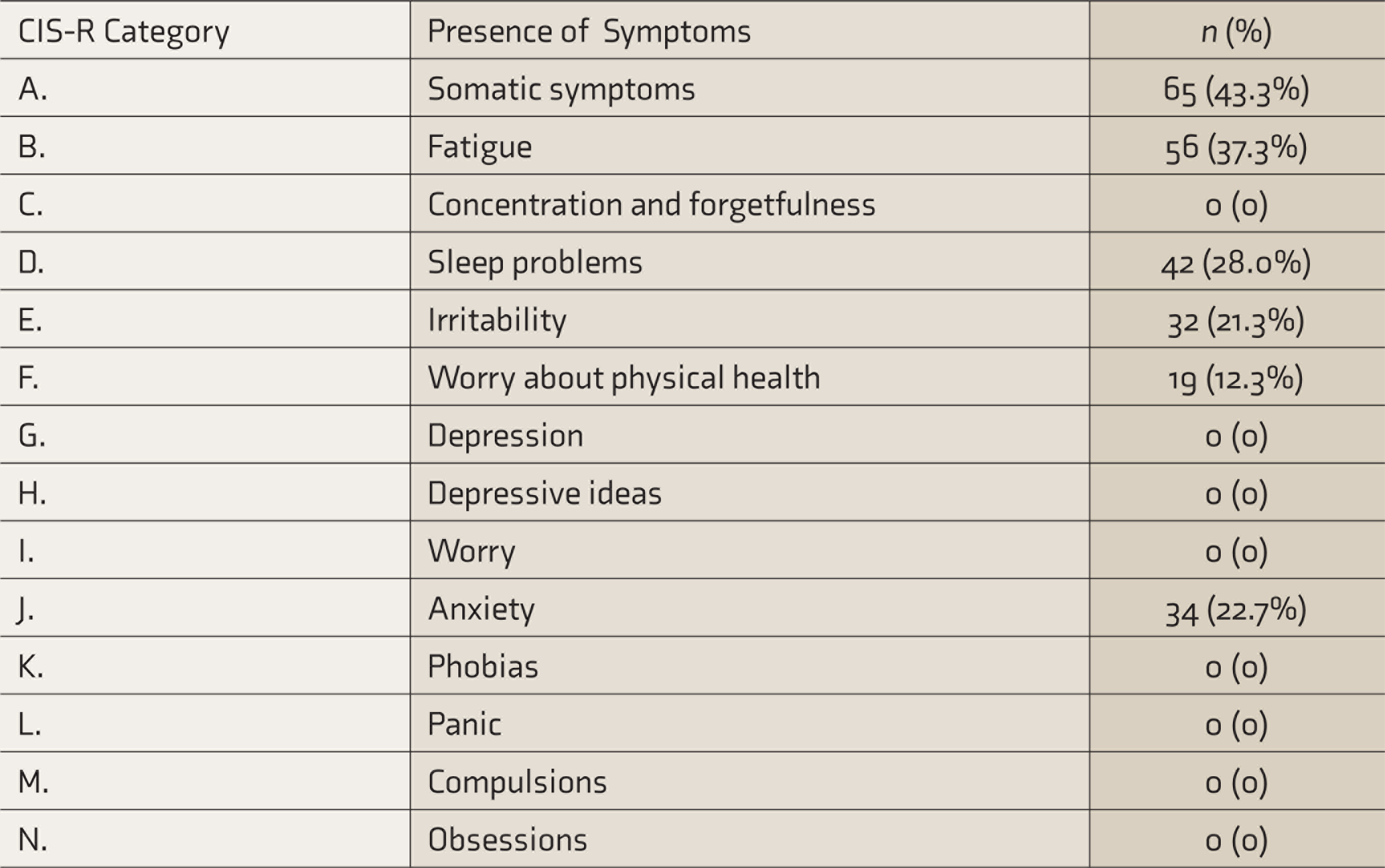
On screening with CIS-R, 23 (15.3%) participants were found to have an antenatal psychiatric disorder. The most common psychiatric symptoms found were the presence of somatic symptoms (43.3%), symptoms of fatigue (37.3%), and symptoms of anxiety (22.7%) (Table 1). None of the subjects were found to have symptoms of depression, depressive ideas, worry, phobias, panic, compulsions, or obsessions.
Presence of Psychiatric Symptoms in the Antenatal Period, According to Clinical Interview Schedule-Revised (CIS-R) (N = 150)
PPD and Associated Factors
Using EPDS, 17 (11.3%) screened positive for PPD. The proportion of PPD was significantly higher among those with an adverse event in the last one year (death in a close family, major illness in the close family, financial loss, or loss of livelihood) (P = 0.01) or low socioeconomic class (P = 0.04, Table 2). The proportion of PPD was also higher among those receiving postpartum care from a caregiver other than the subject’s mother (P = 0.01), those with perceived lack of care and support at home (P = 0.015), and those who reported being worried about their infant’s health (P = 0.01, Table 3). Mothers with antenatal psychiatric disorders had a significantly higher incidence of PPD (39.1%) as compared to mothers without antenatal psychiatric disorders (6.3%, P < 0.001). The proportion of PPD was significantly higher among mothers exhibiting symptoms suggestive of various psychiatric disorders during pregnancy (Table 4).
Association of Postpartum Depression With Sociodemographic Variables (N = 150)
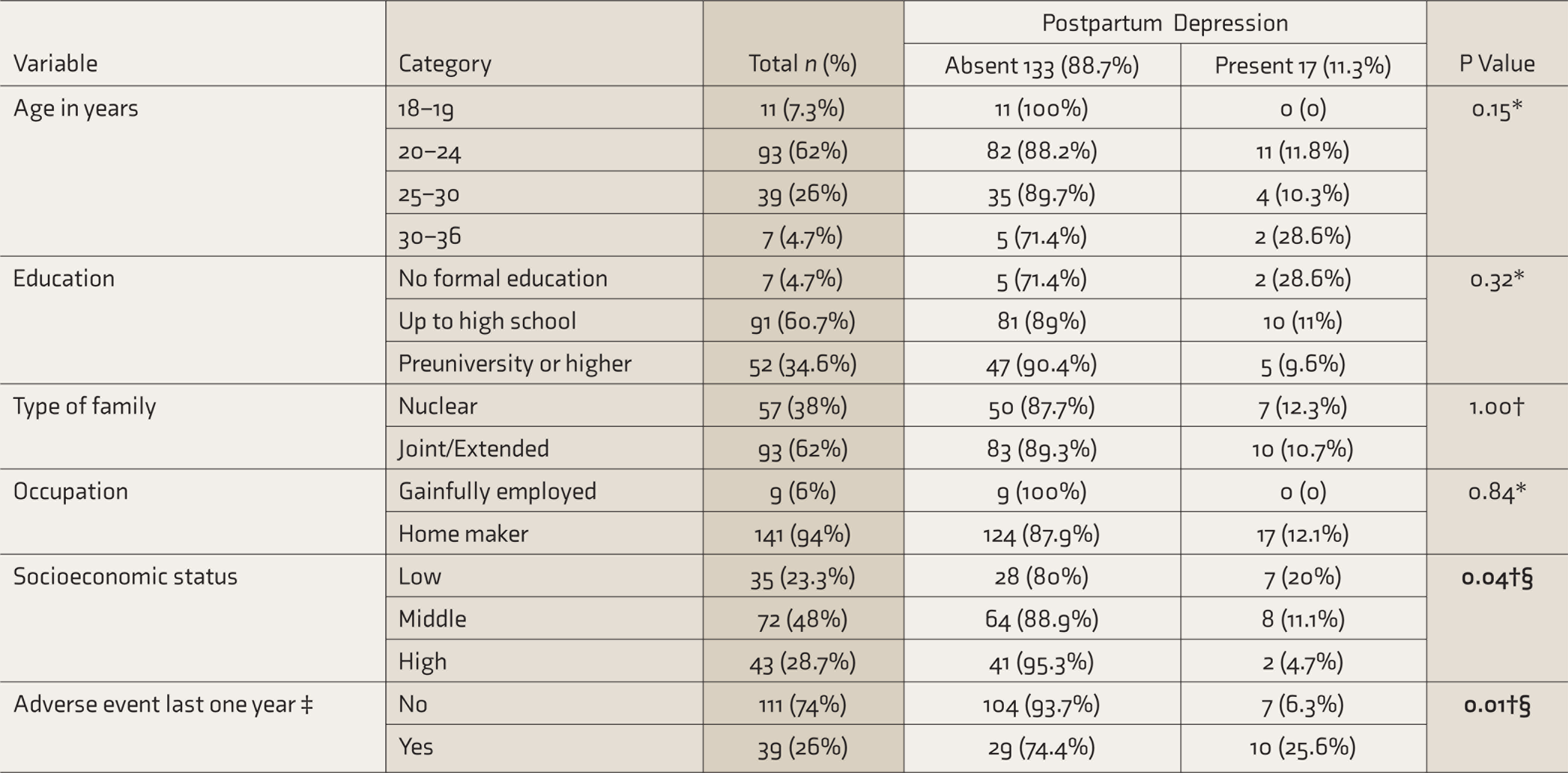
*Fischer’s exact test, † Chi-square test, § statistically significant at <0.05, ‡ death or major illness in close family, financial crisis, or loss of livelihood. The significant p value < 0.05 is depicted in bold.
Association of Postpartum Depression With Obstetric and Postpartum Factors (N = 150)
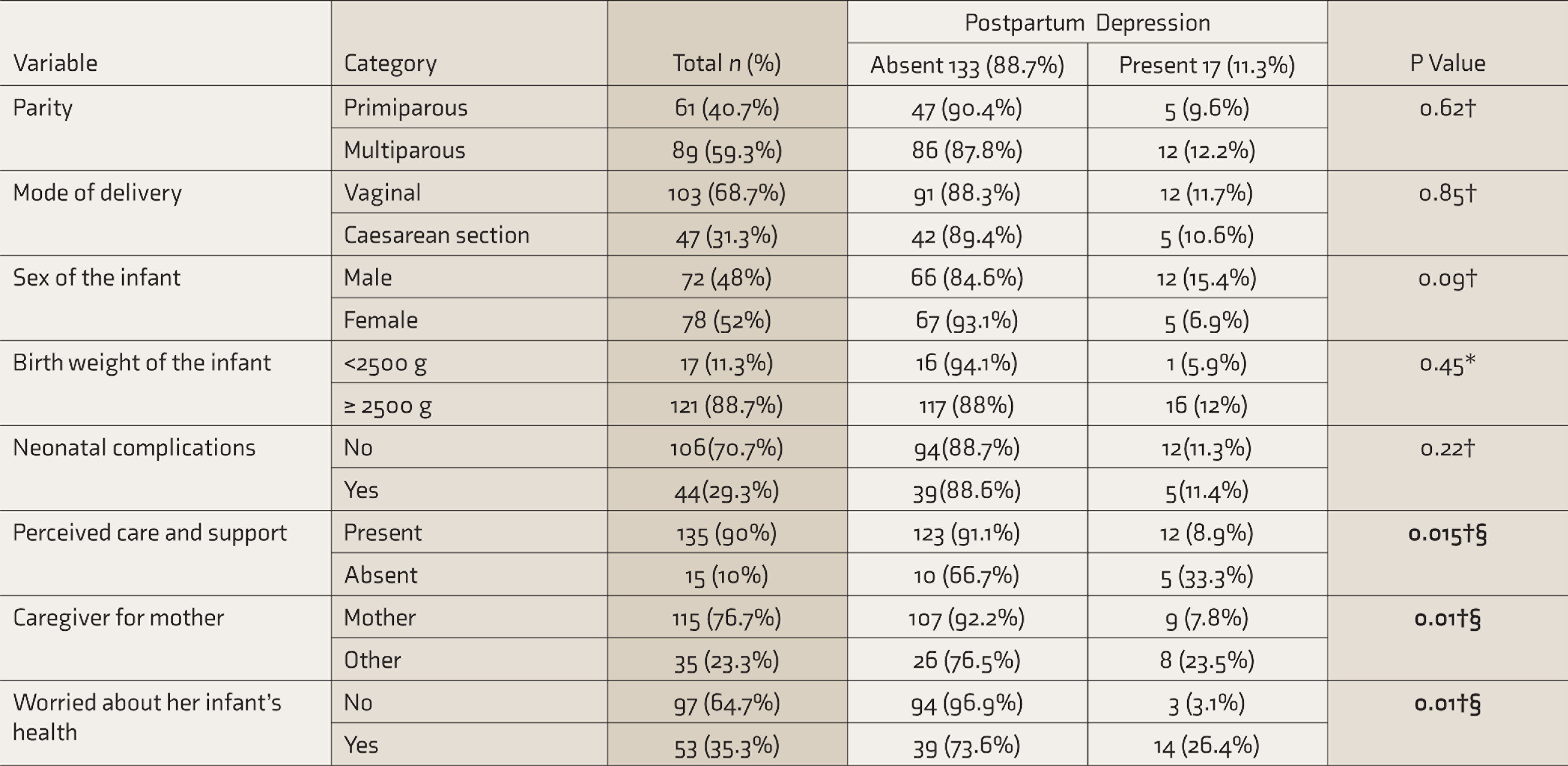
* Fischer’s exact test, † chi-square test, § statistically significant at <0.05. The significant p value < 0.05 is depicted in bold.
Association of Postpartum Depression With Antenatal Psychiatric Disorder and Psychiatric Symptoms (N = 150)
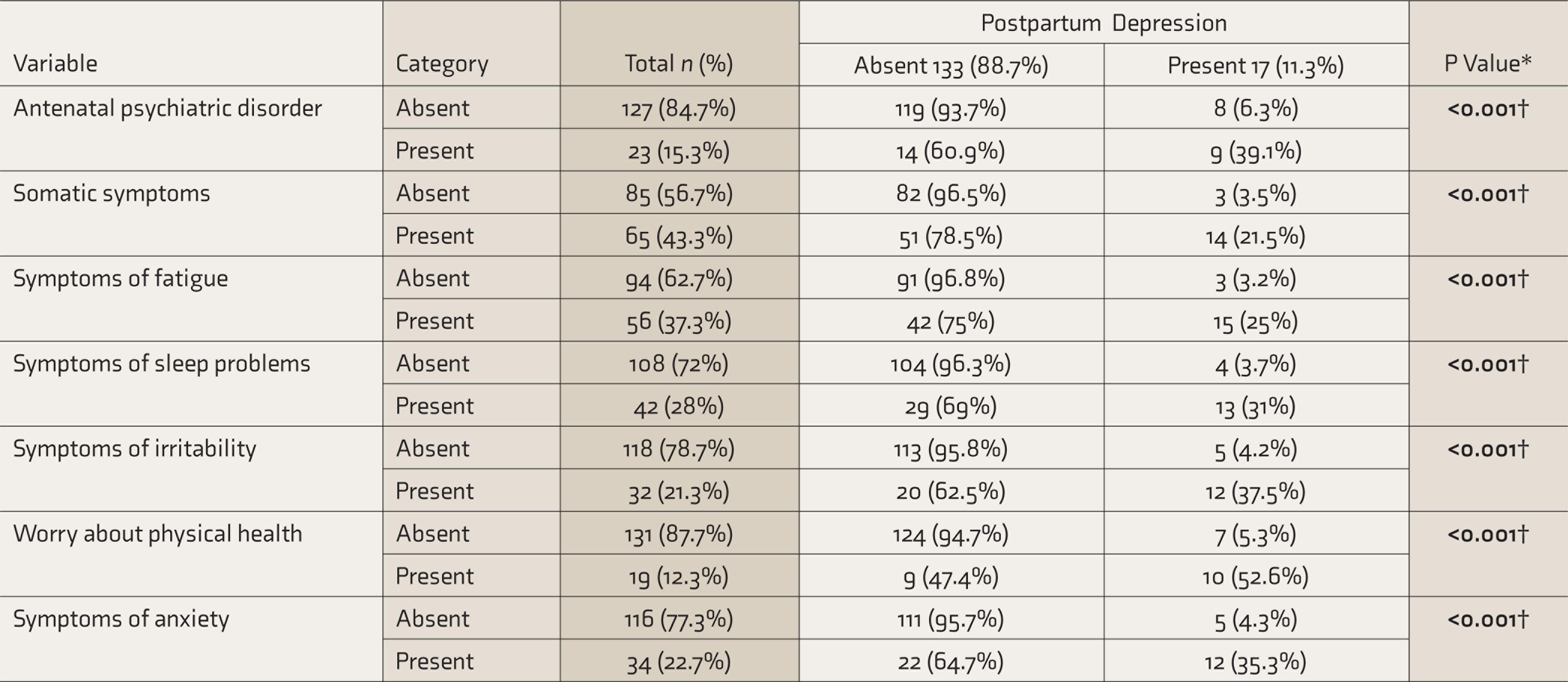
*Chi-square test, †statistically significant at <0.05. The significant p value < 0.05 is depicted in bold.
Logistic regression analysis of factors associated with PPD showed that mothers who were found to have antenatal psychiatric disorder were four times more likely to suffer from PPD (AOR = 4.3 [95% CI 1.22–5.11]; P = 0.028). Mothers who reported being worried about their infant’s health were nearly eight times more likely to have PPD (AOR = 7.7 [95% CI = 1.22–48.32]; P = 0.012]. The chances of PPD were four times greater among those women who were cared for by caregivers other than their own mother (AOR = 4.0 [95% CI = 1.13–8.09]; P = 0.030) (Table 5).
Binary Logistic Regression of Factors Associated With Postpartum Depression
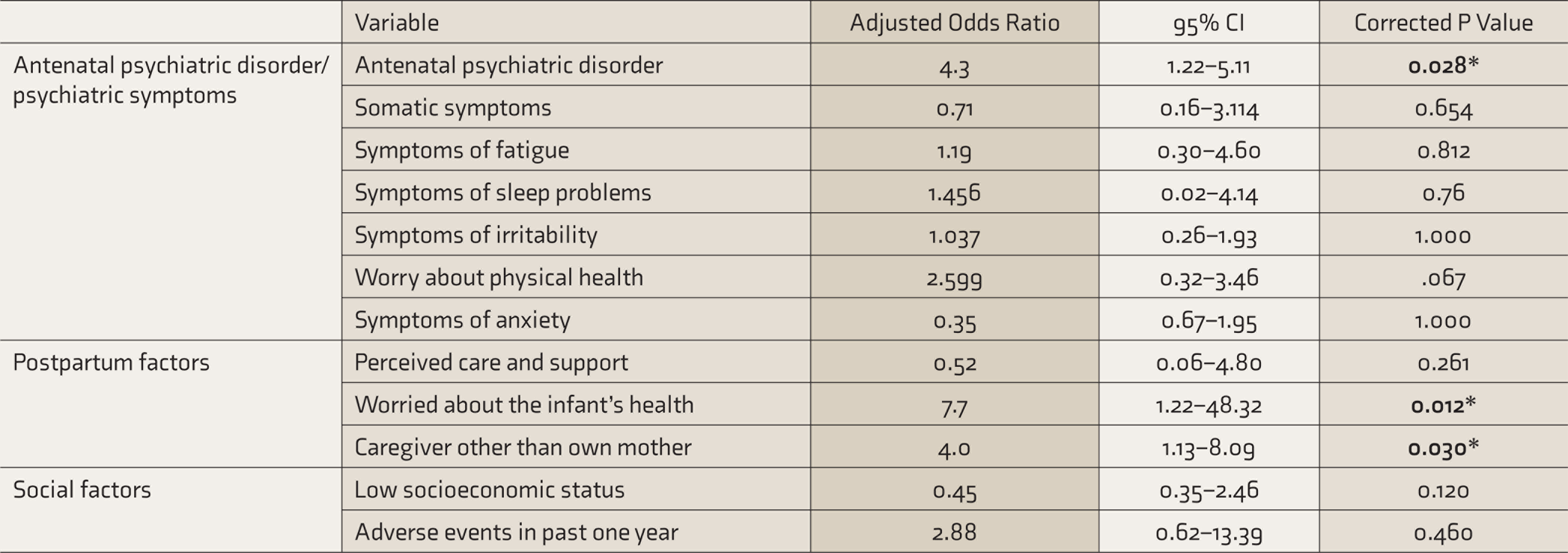
CI: Confidence Interval, *significant at <0.05, Cox and Snell R-square value: 23.9%, Hosmer–Lemeshow Goodness of Fit Test—Chi-square value: 7.223, df 7, P = 0.406. The significant p value < 0.05 is depicted in bold.
Discussion
To our knowledge, this is one of the first longitudinal, community-based studies that examined the link between PPD and various antenatal psychiatric disorders among rural women in India. Using EPDS, we estimated that the incidence of PPD among women residing in the villages of Bangalore Urban District is 11.3%. When compared to other studies, including ours that used EPDS to determine PPD, a much higher proportion of women with PPD was reported from hospital-based studies in rural Ramnagara district (45.5%), 14 rural Mandya district (31.4%) 25 of Karnataka, and Mapusa town of Goa (23%). 20 This may be because we excluded women with known depression, to calculate the incidence of depression arising after birth. Due to the absence of pre-existing depression in our study, our result has a lower proportion, but a relatively accurate reflection of the actual incidence of PPD. On the other hand, the prevalence of PPD reported in the other studies is reflective of both pre-existing depression in pregnancy as well as PPD.
This incidence of PPD indicates that one in every ten women in the rural area is likely to develop PPD. When extrapolated to the number of births among the rural population of our country, it could mean over one and a half million women with PPD. 26 The alarmingly high numbers indicate an urgent need to prevent PPD, especially in disadvantaged population who usually face challenges in accessing quality psychiatric care.
One of the best ways of preventing a disease is through primary prevention, where the chances of a disease occurring are reduced by interventions targeted at the risk factors of the disease. 27 Our study, therefore, looked at the risk factors of PPD and found that one in every seven women had an antenatal psychiatric disorder, and these mothers were four times more likely to develop PPD. Such a link has been demonstrated in a longitudinal hospital-based study in Mapusa town of Goa. The Goa study found that antenatal women with psychological morbidity (screened using General Health Questionnaire-12) were twice more likely to develop PPD at 6–8 weeks. 20
Flow Chart Depicting Study Methodology
The 15% prevalence of antenatal psychiatric disorders found in our study is higher than that found in a hospital-based study in Bangalore city (5.8%) by Johnson et al., which also used CIS-R. 28 Although the education status in both studies was similar, women in the urban study had easy access to referral-level maternity care at the government hospital and psychiatric consultation at a nearby medical college hospital. In contrast, in our study, the nearest referral hospital was around 20 km away, and the medical college hospital was 35 km away. Lack of availability and accessibility of obstetric and psychiatric services may have played a role in the higher prevalence of antenatal psychiatric disorders in our study.
The most common psychiatric symptoms reported in our study were somatic symptoms, fatigue, sleep problems, and anxiety. In contrast, in the study by Johnson et al., 28 the commonest symptoms documented were depression, depressive ideas, irritability, and lack of concentration. This difference may be attributed to the fact that women with depression were not included in our study. Also, in our study, the mean family size was much larger, and the majority of the women were multigravida, which could have resulted in an added burden of household chores in addition to looking after small children, which might account for somatic symptoms, fatigue, and sleep disturbances. It is interesting to note that, in our study, all the reported psychiatric symptoms were individually associated with PPD. This is important as many pregnant women complain of somatic symptoms, fatigue, and sleep disturbances, which are often brushed aside as part and parcel of pregnancy.
Besides antenatal psychiatric disorders, mothers who reported being worried about their infant’s health were nearly eight times more likely to have PPD. This may reflect the poor coping skills and difficulty to deal with challenges of motherhood faced by women with PPD. A mother who excessively worries about her infant’s health should raise a red flag of suspicion of PPD. We also found that the chances of PPD were four times greater among those cared for by caregivers other than their own mother in the postpartum period. This could be because women are better cared for in their parental home, with fewer family stressors and tensions. However, in a study in rural Ramanagara district, women who were away from their husband and living in the parental home during the postpartum period were more likely to have PPD due to separation anxiety, 14 indicating that the quality of the relationship between husband and wife and interpersonal relationships between family members also play a role in the development of PPD. The role of family dynamics and family stressors was further strengthened by our finding that the proportion of PPD was higher among women who perceived lack of care and support at home and reported adverse events in the last one year within the close family. Emotional and financial stressors and personal loss may reduce coping mechanisms and resilience, thereby leading to depression. We also found that the prevalence of PPD was significantly higher among the low socioeconomic class. This has also been found in other studies, both in India and other countries.29,30 Women of low socioeconomic groups are disadvantaged in terms of access to awareness and health care. Therefore, interventions should be more focused on this population.
Sex of the newborn was not associated with PPD in our study, and most mothers reported the lack of pressure to give birth to a male child, unlike the study in rural Mandya, 25 which found that PPD was associated with the birth of a female child. This could be due to the difference in the level of education, where illiteracy was 38% in the Mandya study 25 and 4.7% in our study, demonstrating the important role played by education in women accepting and welcoming female children, possibly as a result of the improved status of women in society through education.
We did not find any link between the age of the mother and PPD, which was similarly reported in other Indian studies.3,8,14,25 However, a Canadian study found that women aged 40–44 years had nearly four times greater risk of PPD than younger mothers. 31 This may explain the lack of association between maternal age and PPD in Indian studies, as maternal age in India tends to be much lower and childbirth after 40 years is not as common as in the West. In our study, we did not have any mothers in the above 40 age group.
Our study has revealed the need for screening for psychiatric disorders in pregnancy to prevent PPD. In the vast rural hinterland, where specialized psychiatric care is not available, we must rely on available mechanisms to deal with this issue. National Mental Health Program recommends imparting short-term training to general physicians and Primary Health Care Medical Officers to diagnose and treat common mental illnesses under the guidance of specialists, with capacity building of village-level workers in screening for mental disorders. 32 Community platforms, such as organized women’s Mahila Mandals, self-help groups, and Village Health and Nutrition Days may be utilized to spread awareness in recognition and destigmatization of common mental disorders in pregnancy and postpartum. The link between family environment and PPD also calls for strengthening the Home-Based Newborn Care Program, where weekly postpartum home visits are to be made by ASHA workers. These home visits can be an opportunity to screen for PPD, observe family dynamics, and counsel the mother and family members.
Strengths and Limitations
Our longitudinal study design and exclusion of pre-existing depression gave us an accurate picture of the incidence of PPD. Being a community-based study with random sampling, our study’s results may be generalized to rural areas in Karnataka state. However, these results may not be generalized to all rural areas in India, as levels of education, the status of women, and family dynamics differ across sociocultural settings in different parts of India. We used EPDS, which has high sensitivity and specificity for screening PPD in Indian settings. However, we have not further used any other diagnostic tool. We also did not study the link between PPD and the presence of medical comorbidities, such as anemia, gestational diabetes, or hypertension. Antenatal psychiatric morbidities not disorders were assessed. Due to logistic reasons, only one postnatal visit could be scheduled per subject, and we may have missed out on PPD that occurred after the visit. To capture various antenatal psychiatric morbidities, we used CIS-R, and for PPD, we used EPDS; the use of two different types of screening tools before and after delivery can be considered a limitation.
Conclusion
The incidence of PPD among the rural women in our study was 11%. The predictors with more than four times higher risk of PPD were antenatal psychiatric disorders, mothers reporting worry about their infant’s health, and mother receiving postpartum care by caregivers other than their own mother. We also found a higher proportion of PPD among women with an adverse event in the last one year (death or major illness in close family, financial loss), low socioeconomic status, and perceived lack of care and support at home. These factors did not retain significance after regression analysis. Based on these findings, we recommend imparting short-term training to general physicians for diagnosis and treatment of common mental illnesses under the guidance of a specialist and also for rural grass-root level workers in screening, referral and follow-up, and strengthening of Home-Based Newborn Care Program, where weekly postpartum home visits by ASHA are an opportunity for counselling mothers and their families and screening for PPD.
Footnotes
Acknowledgements
We would like to acknowledge the Anganwadi workers in the study area who helped in identifying the pregnant women.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.