
Abstract
Purpose of the Review:
Postpartum emotional issues, including postpartum blues, postpartum psychosis, and postpartum depression (PPD), affect many mothers worldwide. The prevalence of postpartum blues ranges from 300 to 750 per 1,000 mothers, while postpartum psychosis has a prevalence of 0.89–2.6 cases per 1,000 births. PPD affects 100–150 new mothers per 1,000 births, and its prevalence can go above 25% globally. Depression in mothers can have long-lasting impacts on children and the next generation, affecting their growth, development, and relationships. However, the condition of PPD is frequently misdiagnosed, and women who suffer from it do not receive treatment. There is a lack of solid systematic evidence that looks at the overall burden of PPD and the risk factors that are associated with it in India. The awareness of PPD is critical in managing the symptoms and seeking professional support, and studies are needed to evaluate and assess the situation in India.
Collection and Analysis of Data:
This study is a systematic literature review with a scoping review approach aimed at providing existing evidence on the awareness and prevalence of PPD in India. The search strategy for the electronic bibliographic search included a list of related terms and factors of awareness and prevalence of PPD. The search encompassed six prominent databases. The assessment tools used in studies from 2012 to 2023 study the factors using the Postpartum Depression Literacy Scale (PoDLiS) and the Edinburgh Postpartum Depression Scale, which measure the awareness and prevalence of PPD. The study found a significantly low volume of studies conducted in India to determine the prevalence of PPD. The materials or studies accessible are hospital-based research with a minimal number of samples. The reported prevalence rate of postpartum depression (PPD) in India varies across different studies, ranging from 4% to 48.5%. Among mothers who gave birth either naturally or by cesarean section in a hospital setting, one study reported the lowest prevalence rate (4%). The prevalence of PPD among women in India is estimated to be 18% based on the average score across all research. A study that evaluated the moms in the community found that PPD was prevalent in new mothers at a rate of 21.5%. There are three studies, in particular, that focus on how aware people are of PPD. Two studies found that 54% of the family members of postpartum moms and women undergoing tertiary pediatric care are aware of PPD.
Conclusions:
Many studies point to the lack of social support as a significant risk factor for mental health complications after delivery. History of depression, anxiety, adverse life events, partner abuse, low economic status, complications at childbirth, and a traumatic childbirth experience are some of the associated factors identified in the studies. Studies have also shown that women who undergo a cesarean section have a higher risk of developing PPD than those with a vaginal delivery.
Postpartum emotional issues include conditions such as postpartum blues, postpartum psychosis, and postpartum depression (PPD). The blues that come after giving birth typically last only a few days to a week, have relatively few adverse effects, and require little more than reassurance for the new mother. 1 The incidence of postpartum blues ranges from 300 to 750 per 1,000 mothers worldwide. 2 These conditions include, but are not limited to, anxiety, an easily upset disposition, being alone, fear of the unknown, and a guilty conscience. On the other hand, postpartum psychosis is a severe condition that manifests within the first four weeks after giving birth and requires the patient to be hospitalized. This condition can occur in any woman who has recently given birth. Postpartum psychosis has a prevalence that ranges from 0.89 to 2.6 cases per 1,000 births around the world. 2 PPD is a much more severe condition; however, it generally goes unnoticed and is not treated, harming the mother and the child. It can begin shortly after childbirth or as a continuation of antenatal depression. According to studies, out of 1,000 new mothers, 100–150 will suffer from PPD. 2 Some studies show that around the globe, the prevalence of PPD goes above 25%.3,4 According to Tareen and Tandon, 5 depression in mothers, unless addressed effectively, can have long-lasting impacts on children and the next generation.
PPD can be a risk factor for chronic or recurrent depression, affecting the relationship between the mother and the infant and the child’s growth and development. Children born to mothers who suffer from PPD are more likely to experience cognitive, behavioral, and interpersonal difficulties than children born to mothers who do not suffer from depression. These difficulties are primarily because PPD affects the mother’s ability to bond with her newborn child. 1 According to the findings of a meta-analysis carried out in upper-middle income countries, children born to mothers who suffered from PPD had a significantly increased risk of being underweight and having their growth rate lower than average. 2 Depressed mothers are also more likely to decide against breastfeeding their children and also more likely to avoid seeking the appropriate medical attention for themselves or their children.
The condition of PPD is frequently misdiagnosed; consequently, women who suffer from it do not receive treatment even though a sizeable percentage of women experience this condition after giving birth; moreover, physical activities during the antenatal stages have an effect on the level of PPD. 6 It is estimated that between 10% and 15% women in Western parts of the world suffer from PPD; however, higher rates have been reported in developing countries. 1
Even though India’s national mental health program is operational since 1982, mothers’ mental health is not yet a primary focus. Adding to that, the absence of specialized services for maternal mental health, trained professionals, and screening tools developed for use in clinical settings makes things more complex, and no data is routinely collected on the percentage of perinatal women who suffer from PPD.
There are an increasing number of empirical studies on PPD in India; however, there is a lack of solid systematic evidence that looks at the overall burden of PPD and the risk factors that are associated with it. Since very little data are collected on a national level, our current understanding of the epidemiology of PPD largely depends on a small number of studies conducted in specific geographic regions.1,2,7 To make a more precise evaluation and assessment of the situation in India, this scoping review focuses on the studies conducted over the past 10 years on the awareness and prevalence of PPD.
Methods
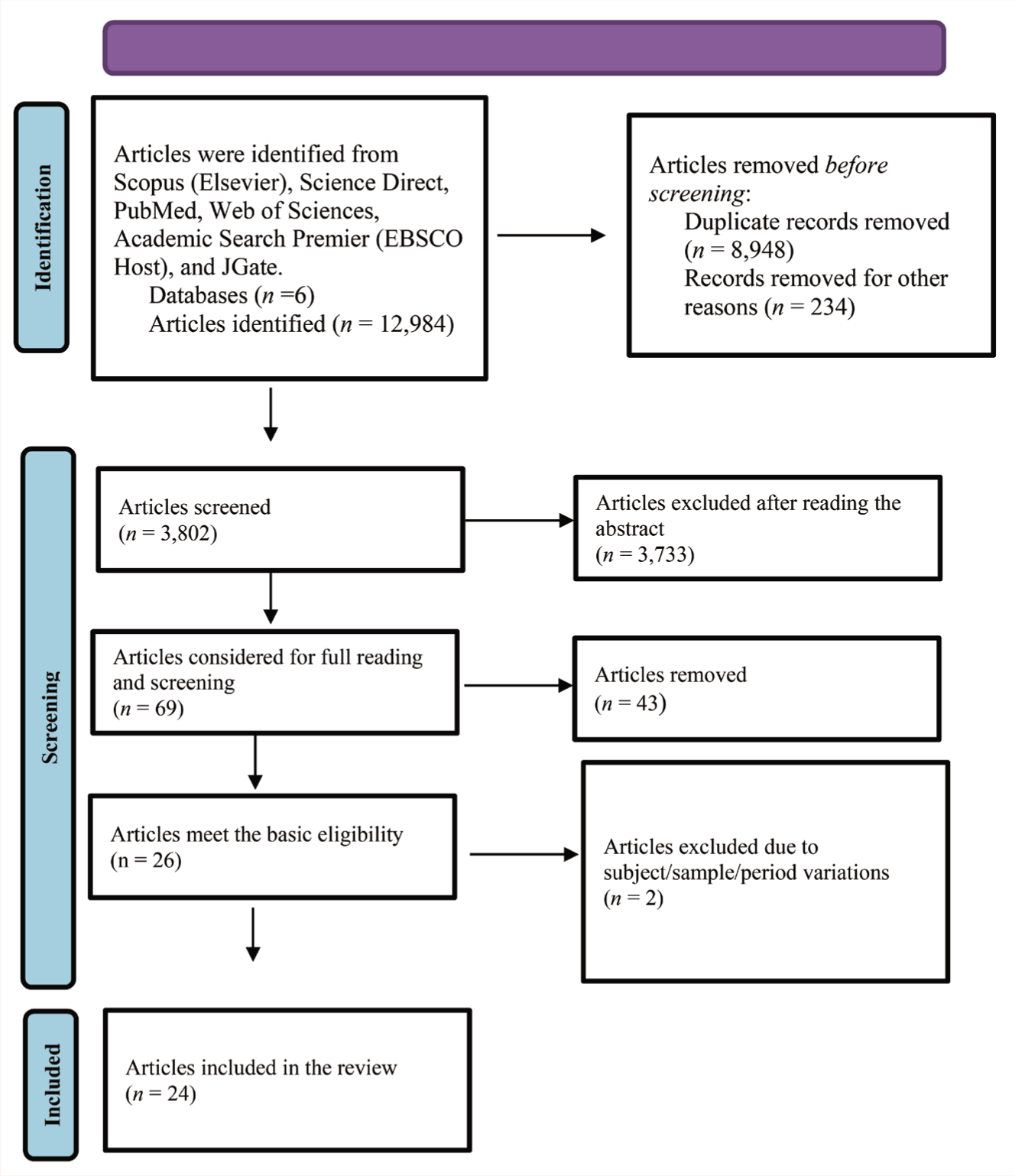
A systematic literature review was conducted on the awareness and prevalence of PPD in India. As indicated by Khalil et al., a scoping review assists in identifying critical research gaps, presenting the research outcome, and providing evidence. 8 In this study, the scoping review aimed at providing the existing evidence on the awareness and prevalence of PPD all over India. Scoping reviews give detailed evidence on the research question. For the electronic bibliographic search, the search strategy included a list of related terms and factors of awareness and prevalence of PPD. Knowledge and awareness of PPD are essential for generating strategies and devising plans to combat the associated threat. The databases included in this study include Scopus (Elsevier), Science Direct, PubMed, Web of Sciences, Academic Search Premier (EBSCO Host), and JGate (Figure 1). Only a few studies have been conducted in India to determine the prevalence of PPD, leaving a gap in postpartum research. The materials or studies accessible are hospital-based research with a minimal number of samples. This scoping review tries to synthesize the evidence generated in India during the past decade.
PRISMA-P Flow Chart of Evidence Screening.
Research Question and Objectives
The research topic was devised to address two critical characteristics of PPD in India: the prevalence and the level of awareness. The full scoping study aimed to build a search string that included as many alternative concepts as feasible, discover relevant published papers, filter the materials, extract the evidence from the shortlisted documents, and develop a synthesis of the evidence published over the past decade.
Identification of Relevant Studies
The search string included the following terms to discover the most significant number of search results within the regional specification (India as a whole) and the period: “postpartum depression” OR “perinatal depression” OR “antepartum depression” OR “postnatal depression” OR “post-delivery depression” OR “postpartum”) AND (“awareness” OR “understanding” OR “knowledge” OR “literacy” OR “aware” OR “consciousness” OR “realization”) AND (“prevalence” OR “presence” OR “existing” OR “extensive” OR “identified” OR “detected” OR “commonly seen”) AND (“youth” OR “young people” OR “youngsters” OR “young adults” OR “adults” OR “young population”) AND “India.”
The researchers systematically searched seven scientific databases—Scopus (Elsevier), Science Direct, PubMed, Web of Sciences, Academic Search Premier (EBSCO Host), Sage Journals, and Google Scholar—in June 2023 to collect original peer-reviewed journal articles published in English from 2012 to January 2023. All identified articles were imported into a reference management system (Mendeley), and all duplicates and titles in different languages (other than English) were deleted.
Screening Procedures and Selection of Reliable Studies
The databases were chosen based on their track record of containing the topic matter, resulting in 12,984 total search results being identified. The criteria for inclusion and exclusion were established. To be included in the scoping review, a peer-reviewed article must be directly related to the study of PPD awareness or prevalence. Included are papers written within the past decade. The evaluation excludes research that explores general depression or anxiety connected to the perinatal period or gestation period. Only studies discussing PPD in the Indian context are included; the remainder is removed. Finally, peer-reviewed articles published in the English language are included in this study. When consensus was required, a collective view from all the writers was gathered to include or exclude a study. The total number of records or articles identified was 12,984, and the number of papers excluded during various processes (duplication: 8,948; after reading the abstract: 3,733; after reading the full paper: 43; and excluded due to subject/sample/period variations: 2) was 12,960. The total number of records selected for review was 24 (see Figure 1).
Data Extraction and Analysis Procedures
After selecting the articles, a spreadsheet was shared among this study’s researchers, and they designated six articles each to do the primary extraction. The recording in the spreadsheet (data extraction sheet) included the author, year, objective of the study, geographical area, characteristics of samples, research design (qualitative, quantitative, and mixed method), sample size, tools used in the study, level of awareness, rate of prevalence, recommendations, and the limitation listed. After the first extraction by the corresponding researcher, a co-researcher performed the extraction, and the extraction’s validity was maintained.
Quality Appraisal of the Included Studies
Study design, study environment (setting), and sampling are the quality standards established for choosing an article. Thus, straightforward literary analyses, reviews of specific sources, and uncritical essays on electronic media have been disregarded.
Reporting the Findings
A narrative overview of the included research was compiled to demonstrate the prevalence and awareness of PPD. A numerical analysis was conducted to determine the sizes of the research studies (sample sizes), geographical distribution, and the rate of prevalence included in the review. Due to the breadth of the outcomes, the other findings were thematically analyzed and presented in themes (see Tables 1 and 2).
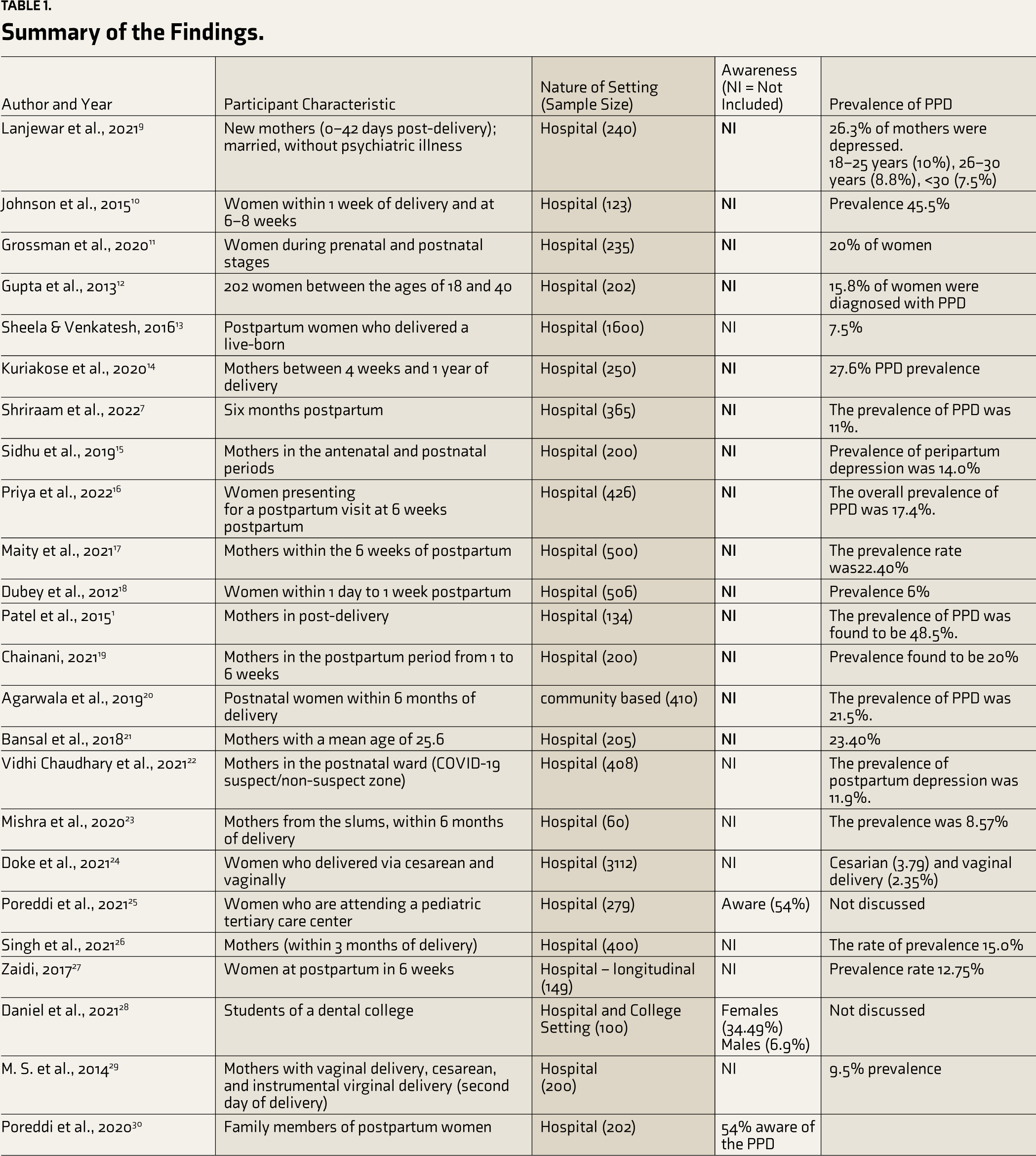
Summary of the Findings.
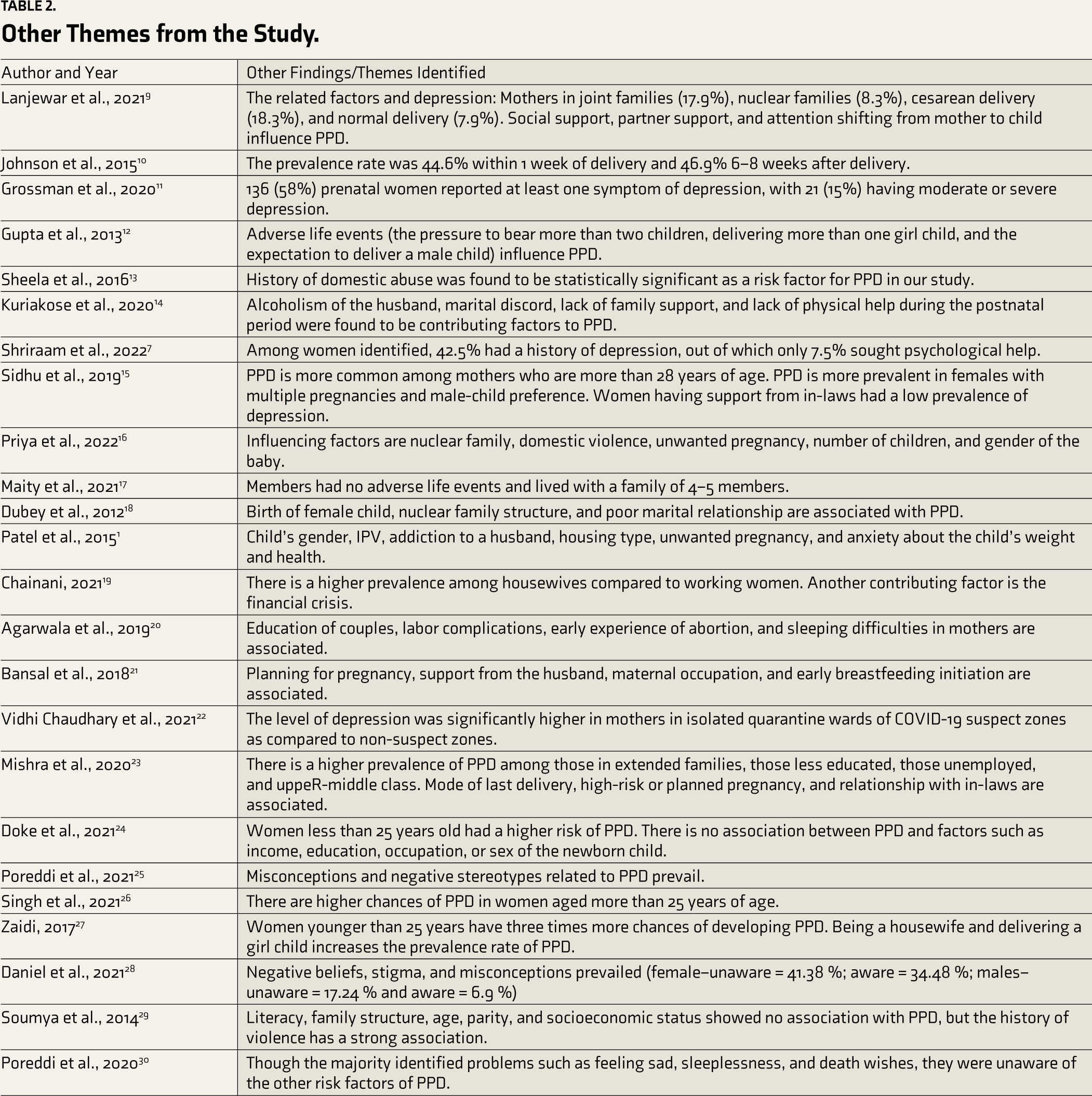
Other Themes from the Study.
Result
Figure 1 summarizes the entire process of this scoping review, especially the document screening and selection. The entire document has undergone four screening stages, including removing duplication, reading the abstract, reading the entire paper, and considering the sample size/subject/time frame.
Type of Methods and Design
Most PPD studies conducted in India from 2012 to 2023 used cross-sectional survey research, while some cohort studies and analytical investigations were also conducted. Nineteen of the 24 studies analyzed in this article were cross-sectional surveys.
Sample Size in the Existing Studies
Most PPD studies conducted in India during the past 10 years have used a sample size of under 300 (mothers). Only two studies have used a sample size of more than 1,000 (1,600 and 3,112). A few studies have also used a sample size of about 100 people.
Study Setting and Period for Inclusion as Samples
The research has been conducted in two settings: hospitals and communities. Most studies (23) have been done in hospital settings, and one study has been done in a community environment. The samples from the hospital settings included mothers who brought their newborns in for immunizations, extended hospital care, or right after birth and within one year after giving birth.
Assessment Tools Used in Studies
The researchers used the Postpartum Depression Literacy Scale (PoDLiS) and self-administered questionnaires to measure awareness of PPD. The Edinburgh Postpartum Depression Scale (19 articles) was the primary tool used to determine the prevalence of PPD.
Prevalence of PPD in India
According to studies, the prevalence of PPD in India ranges from 4% to 48.5%. The study, which included mothers who delivered naturally and by cesarean section in a hospital environment, reported the lowest (about 4%). The prevalence of PPD among women in India is estimated to be 18% based on the average score across all research. Agarwala et al., in a study that evaluated the mothers in the community, found that PPD was prevalent in new mothers at a rate of 21.5%. 20
Level of Awareness on PPD in India
Three research studies, in particular, focus on how aware people are of PPD. In two research studies conducted by Poreddi et al.,25,30 it was found that 54% of the family members of postpartum moms and women undergoing tertiary pediatric care are aware of PPD. However, according to a different study by Daniel et al., 6.9% of male students and 34.49% of female members of a dentistry college are aware of it. 28
Factors Associated with the Prevalence of PPD
Type of family and PPD has shown a correlation, where the studies show that more women in join families experience PPD than women in nuclear families. Also, many studies point to the fact that the method of delivery does have an impact on the level of PPD, as women who gave birth via cesarean show higher numbers than women who delivered vaginally.
Most studies (12 studies) point to adverse life events, including domestic violence, partner alcoholism, lack of familial support, pressure to deliver more than two children, economic issues, unwanted pregnancies, and the sex of the baby, as the significant trigger of PPD for women in India. Even among women diagnosed with PPD, studies found that only 7.5% had taken professional help.
This review found divergent opinions regarding age as a contributing factor to PPD, where two of the studies (Singh et al. 26 and Sidhu et al. 15 ) indicate that the prevalence of PPD is higher among women who are above the age of 25 than the ones below the age. However, studies by Zaidi 27 and Doke et al. 24 indicate a higher prevalence among women under 25.
Recommendations from the Reviewed Studies
Most studies emphasize the need to establish proper support systems and strengthen the existing healthcare system, including management and care for PPD. Early identification of PPD is imperative in providing better service and maintaining adherence to its treatment. Hospitals also need to develop referral systems to establish postpartum clinics.
At the micro-level, the study suggests the need for collaborative approaches in managing PPD with the partner and in-laws as critical players. This is substantiated by the argument that intimate partner violence triggers PPD, and the support from the in-laws to the new mother reduces the prevalence of PPD.
Discussion
The average prevalence rate among the select studies spans from around 4% to 48.5%, including two studies (Johnson et al. 10 and Patel et al. 1 ) that reported a prevalence rate of 45.5% and 48.5%, respectively, almost double the global average. 3 However, these two studies have a sample size below 150 (123 and 134, respectively). On the other hand, Doke et al. 24 reported a very low prevalence (approx. 4% [sample size = 3,112]), with continuous monitoring and follow-up even after the delivery and hospitalization.
Socioeconomic factors including domestic violence, partner alcoholism, lack of familial support, pressure to deliver more than two children, economic issues, unwanted pregnancies, and the sex of the baby were a trigger of high impact. A study by Maiti et al. 17 shows that even without a significant adverse life event, the prevalence rate seems at par with the global average of 22.4% conducted among a sizeable population of 500 postpartum women. This shows that PPD exists beyond socioeconomic conditions, but the impact of adverse life events cannot be ignored.
Familial support is one of the most effective methods to prevent and manage PPD. Sheela and Venkatesh 13 depict that domestic abuse triggers a high risk for PPD, whereas Mishra et al. 23 point out that good relationships with in-laws and spouses are vital factors that prevent PPD. This indicates a need to strengthen familial support for mothers in India.
In India, according to Priya et al., 16 Patel et al., 1 Gupta et al., 12 Zaidi, 27 Dubey et al., 18 and Doke et al., 24 the sex of the unborn (especially the obsession with a male child) and the newborn remains a significant cause of stress and anxiety among the mothers.
Additionally, studies by Patel et al., 1 Priya et al., 16 and Bansal et al. 21 reveal that unwanted pregnancies and pressure to deliver more children increase the chance of PPD among women in India. Delivering more than two children is significantly related to increased stress and anxiety among women, which is underlined in the increased level of PPD among Indian mothers.
Homemakers in urban areas who are less educated are more vulnerable to PPD than their counterparts, which is pointed out in the studies by Zaidi, 27 Singh et al., 26 Mishra et al., 23 and Sidhu et al. 15 These components are risk factors in seeking professional support to manage PPD. As Shriram et al. 7 point out, 42.5% women who were identified as having depression sought professional help.
Tareen et al. 31 suggest that awareness among women and their support systems could enhance the quality of mechanisms to cope effectively with PPD. Among the studies that pertain to the level of awareness in the Indian subcontinent, Poreddi et al.25,30 conducted their study among women attending a pediatric care center and family members of postpartum women. They identified the level of postpartum as 54%. In the meantime, these studies also point to many misconceptions and negative stereotypes about the condition.
Daniel et al. 28 identified that awareness among males (6.9%) is significantly lower than their counterparts (34.49%). The study confirms the existence of negative beliefs, stigma, and misconceptions about PPD.
Limitation of This Review
This review acknowledges the need for more representation across India. This study represents only 11 states, with a sample size comparatively smaller than the entire population. Some studies have included samples of less than 150.
Study Implication and Recommendations
One of the recommendations of this study is that there could be a full-fledged study across India that adequately represents samples from all states in India. Considering the emerging issues among new mothers, the research on PPD should be extended to make practical policy recommendations. Healthcare service providers and professionals need to be educated and trained to identify PPD early and make proper referrals so that the mothers get proper professional care.
The study recommends that an online or offline screening system be made available for professionals at hospitals so that when the mothers visit hospitals for themselves or for their child’s vaccination, this screening test can be administered, and proper professional care can be provided within the hospital using professionals. This study also recommends the establishment of a knowledge repository for public consumption in English and local languages, which will help with education, awareness, self-screening, and even finding professional help.
This study also recommends establishing specialized postpartum clinics in hospitals attached to pediatric departments. These clinics would provide necessary screening and care to mothers up to one year after the delivery.
Conclusion
This review found papers that claim the prevalence level of PPD is as low as 4% and as high as 48.5%. The prevalence of PPD in India can be considered to be between 18% and 20% on average. The level of awareness among people is low, especially among men. Many associated factors trigger PPD, such as adverse life events, misconceptions, and socioeconomic conditions. The recommendations of the studies highlight the importance of accessibility to services related to PPD screening and management. There is an urgent need to initiate a more geographically inclusive study in India on PPD.
Footnotes
Acknowledgements
We gratefully acknowledge the support of Rajagiri College of Social Sciences (autonomous) for providing the financial support to conduct this study under the Institutional Minor Research Policy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support to conduct this study was provided by Rajagiri College of Social Sciences (autonomous) under the Institutional Minor Research Policy.