
Abstract
Background:
The prevalence of postpartum depression (PPD) and anxiety (PPA) is rising in India and efforts at generating local evidence for psychological intervention are scanty. We conducted a single-arm pilot study in an Indian rural community to test the impact of multicomponent psychoeducational intervention (MCPI) on women with PPD and PPA.
Methods:
Forty-three women with PPD/PPA/both received MCPI, which comprised three phases with in-person sessions held once weekly for a minimum of six and a maximum of ten weeks. Primary outcome variables were scores on depression and anxiety, assessed using the Edinburg postnatal depression scale and the state and trait anxiety inventory, along with evaluating the compliance rate to the intervention. The Mini-international neuropsychiatric interview (MINI) neuropsychiatric interview was used to confirm the diagnosis of depression and anxiety. Secondary outcome variables assessed were social support, functionality, parental stress, interpersonal violence, and marital satisfaction. We used Cohen’s d effect size method for assessing the mean differences.
Results:
MCPI resulted in the improvement of 72% women (95% CI = 56.3%–84.7%). The overall compliance rate to the intervention was 85.63%, which was higher for responders than nonresponders (92.9% vs. 69.8%; P < 0.001). MCPI resulted in statistically significant improvement in the mean score of depression (P = 0.001, d = 0.95) and anxiety (P = 0.001, d = 1.30). On secondary outcome variables, significant improvement was obtained in the overall present social support (P = 0.001; d = 4.65), present social support from partner (P = 0.027; d = 0.45) and parents (P = 0.001; d = 0.74), future social support from parents (P = 0.001; d = 0.81), the performance of household responsibility (P = 0.001; d = 0.97), lifestyle in the last two weeks (P = 0.001; d = 3.57), parental stress (P = 0.001; d = 1.04), and marital satisfaction (P = 0.014; d = 0.52).
Conclusion:
This pilot study shows that MCPI has a promising role in relieving depression and anxiety. It also improved the perception of social support from partner and parents, functionality, marital satisfaction, and reduced parental stress.
Keywords
1. MCPI is a brief yet comprehensive and culturally adapted interventional module derived from vital components of evidence-based psychotherapies. 2. MCPI has a promising role in relieving symptoms of depression and anxiety, with improvement in parental stress, functional status, marital satisfaction, and perception of social support from spouse and parents. 3. MCPI has a high compliance rate in community settings and can be included as part of the regular treatment services offered to women with PPD/PPA in the primary care settings.Key Messages:
Postpartum depression (PPD) and postpartum anxiety (PPA) are two of the most commonly reported psychiatric disorders in women. Worldwide, 13% of women who have just given birth experience a mental disorder, primarily depression, 1 while the overall prevalence of PPA at 1 to 24 weeks postbirth is 15%. 2 The situation is even alarming in developing countries, 4 especially India. One of the most recent systematic reviews and meta-analyses indicated that the overall pooled estimate of the prevalence of PPD in India is 22%. 3 Further, PPD/PPA has been found to be not only detrimental for women’s health but also linked directly to difficulties in young children. There is a reduced sensitivity and responsiveness in caregiving,8, 9 resulting in parental stress, which further impacts the quality of mother–child relationships. 10 Thus, studies have reported higher incidences of malnutrition, underweight, diarrheal diseases, incomplete immunization, and poor cognitive development in children having mother with PPD/PPA.4–7 These findings warrant the need for urgent clinical care.
In many high-income countries, the identification and treatment of PPD and PPA are prioritized. Psychotherapeutic approaches such as cognitive behavior therapy (CBT), interpersonal therapy (IPT), and acceptance commitment therapy (ACT) are effective for maternal mental illnesses. 11 Randomized control trials from low-income and middle-income countries resulted in similar findings.12, 13 However, the scarcity of trained mental health professionals to deliver the intervention to underprivileged communities remains one of the biggest challenges in implementation. 14 Further, maternal mental health does not get the priority it warrants, in the face of more pressing issues such as anemia and poor access to hospital deliveries.15, 16 The situation demanded developing an intervention that ordinary health workers could provide in the community. Promising results have been obtained for employing acceptable, feasible, and affordable educational interventions based on locally generated evidence. 17 Further, as psychoeducational interventions that promote problem-solving and a sense of personal agency and help to reframe unhelpful thinking patterns have consistently proven effective in managing PPD and PPA,18, 19 the need was felt to evaluate its implementation in the primary health care setting.
Thus, the study’s primary objective was to develop and pilot-test the impact of multicomponent psychoeducational intervention (MCPI) for women with PPD and PPA in reducing their depression and anxiety along with assessing their compliance rate to the intervention. The secondary objective was assessing the impact of MCPI on the women’s functional status, bonding with infants, parenting stress, social support, interpersonal violence (IPV), and marital satisfaction.
Methodology
The study was approved by the Institute Ethics Committee (IEC). It was also registered with the Clinical Trial Registry of India (Registration number CTRI 2018/01/011086).
This single-arm intervention study was conducted in 28 villages located in Ballabhgarh district in northern India and was designated under the Comprehensive Rural Health Services Project, All India Institute of Medical Sciences, New Delhi.
A community-based study from India found a prevalence of 11% 20 for PPD, whereas a 23% prevalence was reported in a hospital-based study. 21 For this study, presuming a prevalence of 15% and allowing 20% error (80% precision), the required sample size, with a 95% confidence level, was 567. Expecting a 20% attrition rate, the total sample was calculated to be 680. Thus, 680 women aged 18 to 40 years, who had given birth to a live baby and were in the postpartum period (between four weeks and six months postpartum), were screened for PPD and PPA after obtaining informed consent. Women who gave birth to a stillborn or a congenitally malformed baby and those who had a previous diagnosis of psychosis or any other major psychiatric disorder, including substance dependence, or had received psychiatric treatment for the same, were excluded. In addition, those with a history of significant medical/neurological illness, cognitive decline/intellectual disability, or sensory impairment interfering with assessment or intervention were also excluded.
Women were screened for PPD and PPA on Edinburgh postnatal depression scale (EPDS) and state and trait anxiety inventory (STAI). Fifty-nine patients were screened positive for PPD, PPA, or both. Mini-international neuropsychiatric interview (MINI) was then applied as a diagnostic tool that confirmed PPD/PPA or both in 43 women.
Measurement Scales
Sociodemographic and Clinical Data Sheet: Information was collected about the age, literacy, education, and occupation of the mother, along with detailed obstetric history. Socioeconomic status (SES) was assessed using a modified Udai Parikh scale. 22
Edinburgh postnatal depression scale (EPDS) 23 is a 10-item self-report measure of depressive symptoms. Screen positive was defined as a total score of >10. 24
State-trait anxiety inventory-form Y (STAI-Y-1) 25 consists of a 40 items self-evaluation questionnaire for state and trait anxiety. In the present study, STAI form Y-1 (STAI form Y-1) was used. Although the range of scores is from 20 to 80, a score of >40 was used as a cut-off for high anxiety. 26
Mini-international neuropsychiatric interview (MINI)-Sixth edition 27 was administered to women who were screened positive on EPDS, STAI, or both, to confirm the diagnosis of PPD, PPA, or both. It was also used to rule out any other psychiatric disorder.
Postpartum social support questionnaire (PSSQ) 28 was used to measure the present expected social support for women from partners, parents-in-law, and extended family and friends across 32 items. In the absence of clearly defined cut-off values, the Student t-test was used to compare the mean scores on the PSSQ across responder and nonresponder groups. The scale is positively worded such that a higher score indicates better social support and vice-versa.
Postpartum bonding questionnaire (PBQ) 29 was used to assess four different manifestations of bonding difficulties–impaired bonding (IB), rejection and pathological anger (RP), infant–focused anxiety (IFA), and incipient abuse (IA). A score >11 indicates IB, >16 indicates RP, ≥ 9 indicates IFA, and >2 indicates IA.
Inventory of functional status after childbirth (IFSAC) 30 contains five domains to measure a mother’s readiness to assume infant care and resume self-care, household responsibilities, social activities, community activities, and occupational activities following childbirth. As suggested by the authors, the overall functional status and the mean scores for each functional domain were calculated.
Parental stress index-short form (PSI-SF) 31 is a scale consisting of 36 items across three domains. Because two of the domains were applicable for older children, the present study employed only one domain, i.e., parental distress (PD), pertaining to infants. The cut-off value for PD was not available, hence scoring was done with reference to mean and standard deviation values of the 12 items. The scale is reverse coded such that a lower score indicates higher parental stress and vice versa.
HITS measure of intimate partner violence (HITS) 32 is a screening tool for intimate partner violence. There are four domains. Each domain is scored on a 1 to 5 Likert scale. A score >10 is considered positive for domestic abuse.
Kansas marital satisfaction scale (KMSS) 33 comprises three questions about the women’s rating of satisfaction with marriage, spouse, and relationship with the spouse on a 7-point Likert scale. A score <17 is considered to have poor marital satisfaction.
The World Health Organization guidelines for scale translation and adaptation were followed to translate all the scales except MINI, a clinician-administered tool, into Hindi.
Intervention
MCPI was developed after a comprehensive literature review of available evidence-based treatments (CBT, IPR, and ACT) to address postpartum mental health concerns. The intervention was adapted to include the sociocultural dynamics of the villages under study. Adaptation was made in three domains, i.e., language, content, and treatment delivery.
For language adaptation, translation of the intervention was done into the local language for the ease of understanding. Contextually appropriate examples were employed to facilitate learning. For instance, local idioms and symbols were used to convert an abstract concept such as mood/feelings into a more concrete, easy-to-understand idea—e.g., the use of a mood bucket to identify and rate the quantity of feelings.
The second form of adaptation pertained to the content of the intervention. For example, women were encouraged to engage in locally practiced Yoga rather than progressive muscle relaxation techniques. Activity scheduling included locally practiced skills (like stitching and candle making) or activities such as taking care of pet animals (cows and buffaloes). Coping skills training incorporated sharing her stress with the neighborhood women while performing daily chores (getting water) at familiar places (wells or handpumps). Similarly, contextual factors about women’s broader social, economic, and political context were addressed.
The third adaptation pertained to the treatment delivery. For example, a few but extended sessions were provided to avoid attrition instead of keeping many short and frequent sessions. Sufficient time was allocated to clarify misconceptions associated with treatment, causation, and recovery. Home visits were not considered cost-effective. Because of privacy and stigma concerns, local health workers (such as Anganwadi and Asha workers) arranged for therapy with a clinical psychologist in the health center located near their house such that it was convenient for women.
The broad structure of the intervention was divided into three phases. Details of each stage of intervention have been outlined in Table 1.
Outline of the MCPI Intervention Module
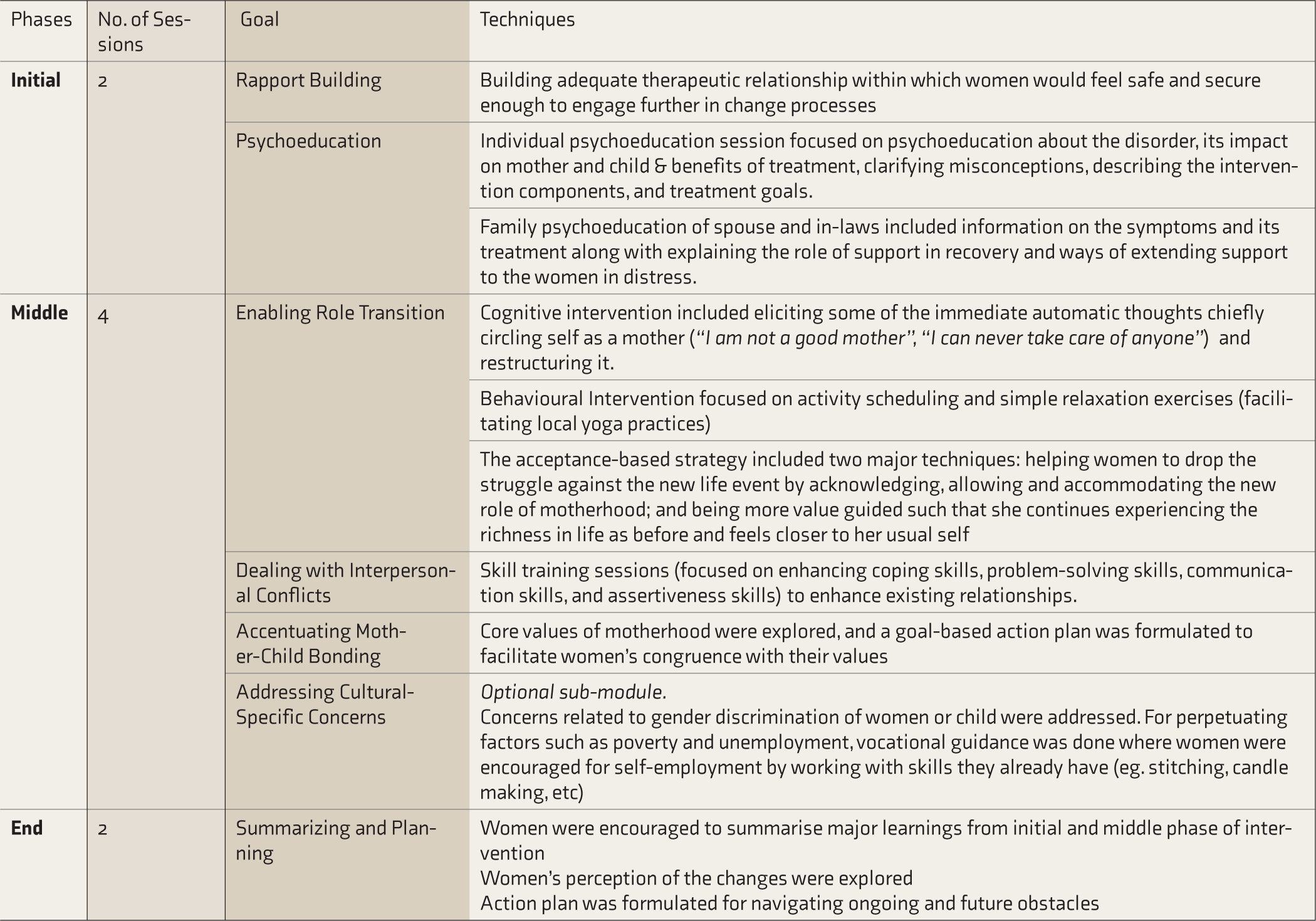
MCPI=Multicomponent Psychoeducational Intervention.
Procedure
After obtaining written informed consent, 43 women with PPD/PPA or both were invited to participate in the MCPI pilot study. The preintervention assessment was completed on the scales EPDS, STAI, PSSQ, PBQ, IFSAC, PSI- SF, HITS, and KMSS. Following the assessment, MCPI was delivered across three phases. Sessions were held once weekly for a minimum of six and a maximum of ten weeks. Each session lasted approximately 90 min. After completion of the intervention, postassessment was completed on all the tools as mentioned in preassessment. The entire assessment and intervention on the 43 women were conducted by two trained clinical psychologists who had adequate experience working in the community. A community psychiatrist monitored the treatment protocol under the supervision of the study’s principal investigators. The duration of the study was from October 2014 to November 2016.
Statistical Analysis
Statistical analysis was carried out using statistical software SPSS IBM version 25.0 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.).
Continuous variables were tested for normality of assumptions using the Kolmogorov–Smirnov test. Continuous variables were tested for normality of assumptions using the Kolmogorov–Smirnov test. Changes in scores from pre- to postintervention were compared using paired sample t-test. A comparison of mean values between the two groups (responders and nonresponders) was done using the independent sample t-test.
The effect size was calculated using the method of Cohen’s d for the mean differences. The interpretation of effect size (d) was based on the classification where ≤0.3 indicates a small effect, 0.5 to 0.7 a moderate effect, and ≥0.8 a larger effect. Women’s compliance to the therapy sessions were calculated using the following formulae:
Number of sessions attended/Number of planned session × 100.
To assess the consistency of the results, we conducted exploratory comparative analysis on a group of responders and nonresponders to MCPI on the total mean score obtained from the scales EPDS, STAI, KMSS, HITS, and PSI. For exploratory analysis, only scales with total scores were selected.
For all statistical tests, a two-sided probability of P < 0.05 was considered as statistical significance.
Results
The mean (±SD) age of women was 23.07 (±1.47) years. In the study subjects and their partners, 88.4% and 90.7%, respectively, had received formal education. About 47% belonged to lower middle SES, and 84% belonged to a joint family with <5 family members living together. The majority (79%) of male partners were involved in money-earning occupations and reported no history of substance use in the family.
Regarding pregnancy, about 86% had at least two pregnancies, and most of them reported vaginal mode of delivery with no major complications during pregnancy, after delivery, or in breastfeeding. The pregnancy was reported to be planned and desired by the majority of women. Further, about 98% have had at least one full-term pregnancy, and 63% had at least two living children.
MCPI improved symptoms in 72% (95% CI = 56.3%–84.7%) of women (31/43). Of the 31 women who showed improvement, 7 (22.6%) with PPD, 10 (32.2%) with PPA, and 14 (45.2%) with both PPD and PPA improved. The overall compliance rate to MCPI was 85.63%, which was higher in nonresponders (92.9% vs. 69.8%; P < 0.05). Improvement in the mean score of depression (P = 0.001, d = 0.95) and anxiety (P = 0.001, d = 1.30) from pre- to postintervention is shown in Table 2.
Pre- and Postintervention Score on Scales of Depression, Anxiety, Social Support, Functional Status, Parental Stress, Intimate Partner Violence, Marital Satisfaction, and Bonding
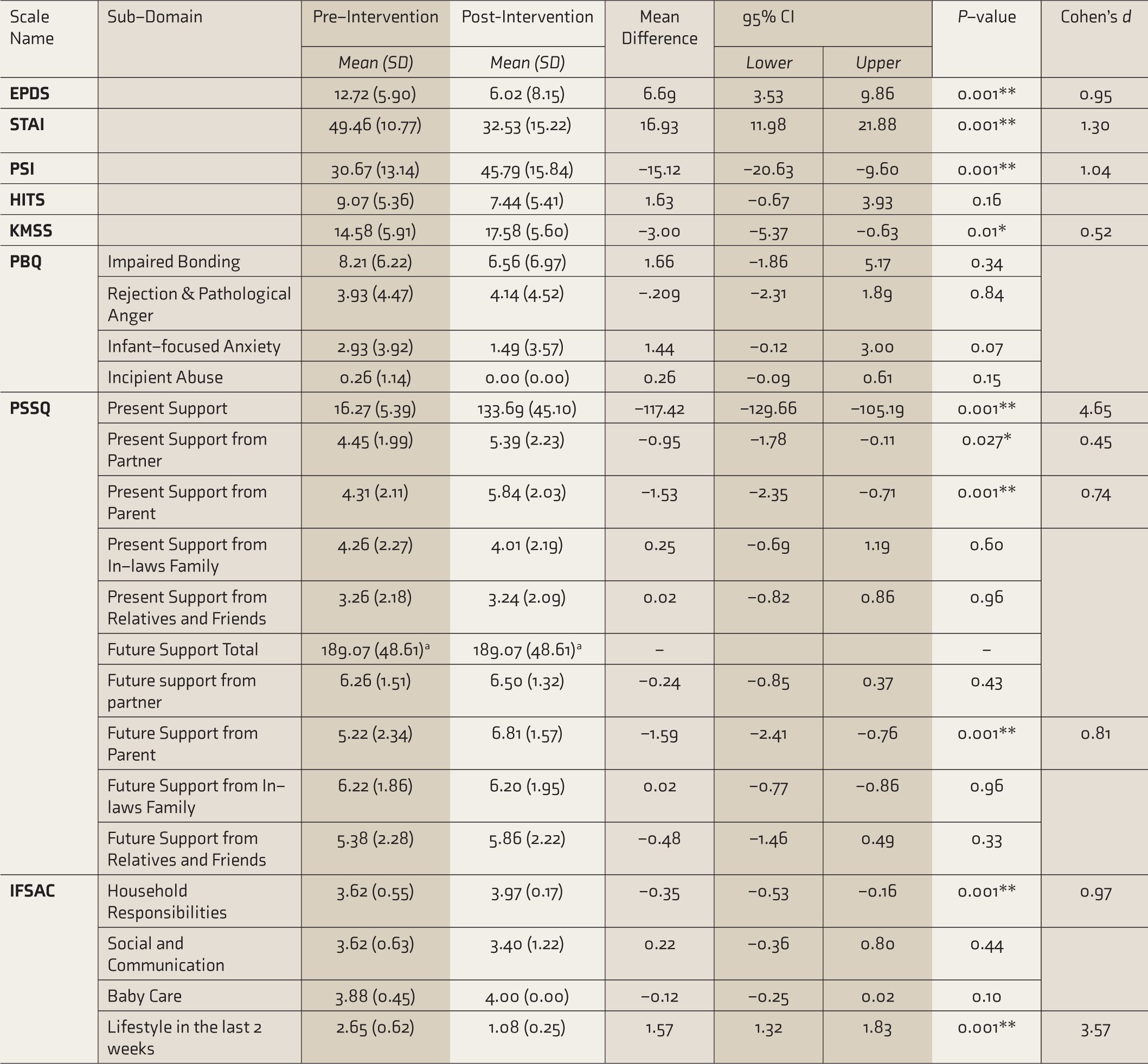
CI= Confidence Interval; PSSQ= Postpartum Social Support Questionnaire; IFSAC= Inventory for Functional Status After Childbirth; PSI= Parental Stress Index; KMSS= Kansas Marital Satisfaction Scale; PBQ= Post-Partum Bonding Questionnaire
The correlation and t cannot be computed because the standard error of the difference is 0.
* P Value is significant at 0.05 level
** P Value is significant at 0.001 level
Out of 43, however, one woman reported severe anxiety symptoms, and two reported suicidal ideations on MINI. Pharmacotherapy was provided to them in adjunct with MCPI.
There was a significant improvement in the perception of the overall present social support (P = 0.001, d = 4.65), present social support from partner (P = 0.027, d = 0.45) and parents (P = 0.001, d = 0.74), future social support from parents (P = 0.001, d = 0.81), the performance of household responsibility (P = 0.001, d = 0.97), lifestyle in the last two weeks (P = 0.001, d = 3.57), parental stress (P = 0.001, d = 1.04), and marital satisfaction (P = 0.014, d = 0.52).
Lastly, findings obtained on exploratory analysis of responders (n = 31) and nonresponders (n = 12) to MCPI were in corroboration with that of 43 women with PPD/PPA. Overall, the pre- to postintervention reduction in scores on EPDS (d = 2.23) and STAI (d = 2.42) was highly significant (P < 0.001) with a very large effect size. On account of the reduction observed in the depression- and anxiety-related scales, there was a significant (P < 0.001) increase in the marital satisfaction score (d = 1.07) and a significant reduction in IPV (d = 1.00) and parental stress index (d = 1.94), with a larger effect size.
Discussion
The present study found that symptoms of depression and anxiety improved significantly after MCPI, with a large effect size. Additionally, there was a significant reduction in parental stress and enhancement of functionality, marital satisfaction, and social support from spouse and parents. The findings support conclusions from studies assessing the comprehensive improvement of women than only symptoms of PPD or PPA. One such meta-analysis of ten studies, including 1324 depressed mothers, found that in addition to improvement in symptoms of depression, women receiving the psychological intervention reported lower levels of anxiety, significantly higher level of social support, improved marital relation, and better adjustment to parenthood.4, 34 Another systematic review and meta-analysis, including 13 studies from low- and middle-income countries, reported that psychological intervention had a significant positive effect on growth and development, decreased neonatal mortality, and decreased rate of infectious disease in infants. 4 The present study’s findings also align closely with a recent meta-analysis of the Indian literature that suggests an alarming increase in PPD/PPA. 3
Postpartum is also a phase where, despite undergoing major role transitions, the daily functionality of the women can get severely impacted. In the present study, various aspects of the functional status of the women were assessed using IFSAC. After the intervention, an increase in maternal functional ability was observed in the subdomain of “lifestyle in the last two weeks” and household responsibilities. Therefore, the present study results confirmed that PPD/PPA have a deleterious impact on the various domains of maternal functioning, 35 which may soon be resumed if the mothers are provided with adequate skill training and social support.
Parental stress is another factor defining role transition into motherhood, especially for mothers with PPD/PPA. Thus, we included in the module skill training to deal with parenting stress, which led to significant improvement in it after the intervention. Such findings are in line with studies highlighting a significant association between parental stress and PPD/PPA.36, 37 Thus, to prevent deterious impact on mother–child interaction and child’s care in the long run, there is an urgent need for early identification and treatment of PPD/PPA. 38
MCPI included a specific focus on enhancing effective interpersonal relationship with spouses and in-laws. As a result, significant improvement in the women’s felt sense of support from spouses and family members was noticed. Similarly, several studies have demonstrated that IPV and marital distress are also associated with postpartum mental health problems.39, 40 In fact, there is an increased risk of IPV for new mothers41, 42 during the postpartum period, with prevalence rates ranging 2% to 25%. 43 Interestingly, in our study, significant IPV was not noted in the women with PPD/PPA prior to the intervention, and hence, no significant change was observed in the postintervention assessment of 43 women. However, exploratory analysis across responders and nonresponders found a significant reduction in IPV scores among responders, with a large effect size. It must be noted that the conclusion obtained on exploratory analysis is not robust and would require further controlled trials for confirming the evidence for the same. Further, however, because MCPI addressed ways of dealing with interpersonal conflicts and enhancing relationships, the women reported significantly higher marital satisfaction after the intervention.
PPD/PPA can profoundly affect mother–child interaction and can cause a spectrum of difficulties like decreased maternal affective involvement, increased irritability, aggressive impulses, or, at worst, an outright rejection of the infant. 44 MCPI assisted women in developing a nurturing relationship with the infants. Interestingly, however, no significant difference in any parameter of postpartum bonding was obtained. Because the preintervention scores were within the range even before providing MCPI, it can be assumed that the impact of PPD/PPA on mother–infant bonding is less in the community setting than reported in the literature.45, 46 Thus, one of the key findings that emerged from the present study was no significant change in infant care because of the condition of PPD/PPA in the mother. These findings are consistent with other research where women with PPD continued to provide regular physical infant care despite depressive symptoms.47, 48 Further qualitative and longitudinal research may be needed to explore reasons for the same.
Further, the MCPI module is effective as it addresses practical and psychological barriers and provides a broader range of support. The intervention module had added the advantage of incorporating multiple components derived from cognitive behavior, interpersonal, acceptance, and supportive therapies. Moreover, its cultural sensitivity and easy availability to women could have contributed to the good treatment compliance (85.63%) noticed. It is well established in the literature that the cultural sensitivity of an intervention module based on a patient’s broader social context ensures optimal psychological treatment. 49 Supporting evidence comes from Ammermam et al. (2013), 50 who conducted a small randomized trial of in-home CBT for depressed mothers. Significantly greater improvement was reported postintervention and on follow-up. The authors commented that adapting treatment to home-based settings enhances engagement, compliance, and hence, effectiveness.
Thus, the present study provides promising evidence for MCPI as a culturally adapted, brief, and easily applicable intervention in the community setting, enhancing its applicability across multiple settings. Hence, the study implicates that MCPI can be incorporated as part of the regular treatment services offered to women in the primary care settings. In fact, one of the most promising systematic reviews here on content and delivery of psychological intervention for perinatal depression by nonspecialist health workers in middle- and low- income countries highlighted that task shifting is required in low-resource settings where specialist services are both scarce and expensive. 51 The evidence has been promising when such interventions are delivered under ongoing supervision and structured training of health care workers. 51 A similar format can be employed in future studies on MCPI so that it complies closely with the aim of the World Health Organization for task shifting and capacity building in low- resource settings.
Limitations and Future Directions
Despite its various significant findings, the study suffers from a few limitations. The foremost is the absence of a control group and follow-up assessment. Then, the use of self-rated tools only for assessing the pre- and post-intervention changes introduces the possibility of bias in the form of the “Hawthorne Effect.” A larger sample size, controlled trial, and a longitudinal follow-up may be needed to comment on the effect size of the intervention’s effectiveness. In addition, data on some of the extraneous variables (such as duration of illness, time since delivery, and the severity of disease) impacting results were not assessed. Further, while MCPI has been proven to be beneficial for the community women, it is difficult to discretely segregate the impact of a specific treatment technique on a specific symptom. To overcome this limitation, a component-specific trial can be planned on disorder-specific symptom presentation. Lastly, to disseminate the treatment awareness and effects, home-based interventions, including training community lady health workers to deliver the intervention, would be a necessary next step.
Conclusion
MCPI is a brief and culturally tailored interventional module derived from key components of evidence-based psychotherapies easily applicable for a low-resource community setting. The present pilot study shows that MCPI has a promising role in relieving symptoms of depression and anxiety, with improvement in parental stress, functional status, marital satisfaction, and perception of social support from spouse and parents. Large-scale randomized controlled trials can be planned in rural community settings to further establish the effectiveness of the intervention.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received financial support from the Indian Council of Medical Research (ICMR) to carry out the research.