
Abstract
Background:
The growing prevalence of schizophrenia in Indonesia requires the consideration of the families, caregivers, health care professionals, and the entire society, to serve as a support and coping resource for the patients. The process of recovery is rather difficult, especially in the absence of a decent place to live. Hence, there is the need to provide a supportive environment that facilitates recuperation from psychotic symptoms, enhances interaction with others, promotes self-expression of thoughts and feelings, and helps deal with daily stress and challenges. There are currently no studies on the framework of societal adaptation for people with schizophrenia (PWS). The aim of this research, therefore, was to explore the experiences of rural society inhabitants in adapting to PWS in Indonesia.
Methods:
The study uses a qualitative research design and implements an interpretive phenomenological approach. A total of ten society members were recruited from the community by purposive sampling, and the in-depth interviews conducted were audio-recorded and transcribed. In addition, thematic analysis was carried out using the interpretive phenomenological analysis method.
Results:
The majority of the participants assumed that PWS prompt the feeling of alertness over fear. In addition, the participants revealed a feeling of indecisiveness in related situations and emphasized the value of keeping up traditional beliefs and practices and the effectiveness of a demonstration of indifference. They explained the need to combine traditional and modern health practices as recommended by the spiritual leaders.
Conclusion:
Societal adaptation to PWS entails the understanding of how to deal with the disease’s uncertainty and complexity. It is important to create a supportive environment to promote mental health and wellbeing.
Learning about the societal adaptations to people with schizophrenia is an important step to overcome the social barriers during community treatment. Spiritual leaders play a powerful role as change agents in determining the way members of the community ultimately adapt.Key Messages:
Society support is a very powerful factor in the recovery of PWS. There are eight domains of recovery from mental illness, which include the abilities to work/seek learning programs, engage in social activities, establish daily routines, perform independent activities, understand and accomplish tasks and projects, improve wellbeing, decide goals, and manage the symptoms with psychosocial therapies. 9 The society could provide a collective and supportive environment for dealing with daily stress and social changes. A sense of belonging, trust, and self-confidence, which are the results of community engagement, embodies PWS’ social attachment, social engagement, and participation in communities.
The growing prevalence of schizophrenia in Indonesia needs to be possibly addressed through an adequate consideration of family, caregivers, health care professionals, and members of the whole society, to serve as supportive coping resources for the patients. The process of recovery is rather difficult, especially in the absence of a decent place to live, hence the need to provide a positive environment for managing daily stress and challenges. Currently, there is no study on the frameworks of societal adaptation to PWS. Using data assimilation from the participants’ verbatim responses help researchers create certain guidelines on societal adaptation. The aim of this study, therefore, was to explore the experiences of societies in adapting to PWS in a rural area, as well as the different forms of support provided in Indonesia.
Subjects and Methods
An interpretive phenomenological design was used to investigate the lived experiences of participants, in an attempt to recognize interpretative human stories as a form of sense-making mechanism. In addition, in-depth semi-structured interviews were used to investigate the societal experiences in adapting to PWS in Indonesian rural communities. Meanwhile, phenomenology was adopted to obtain an explanation, understand the meanings attributed to the experiences, and convert these observations into questions on the means to study and understand these relations.
Characteristics of Participants
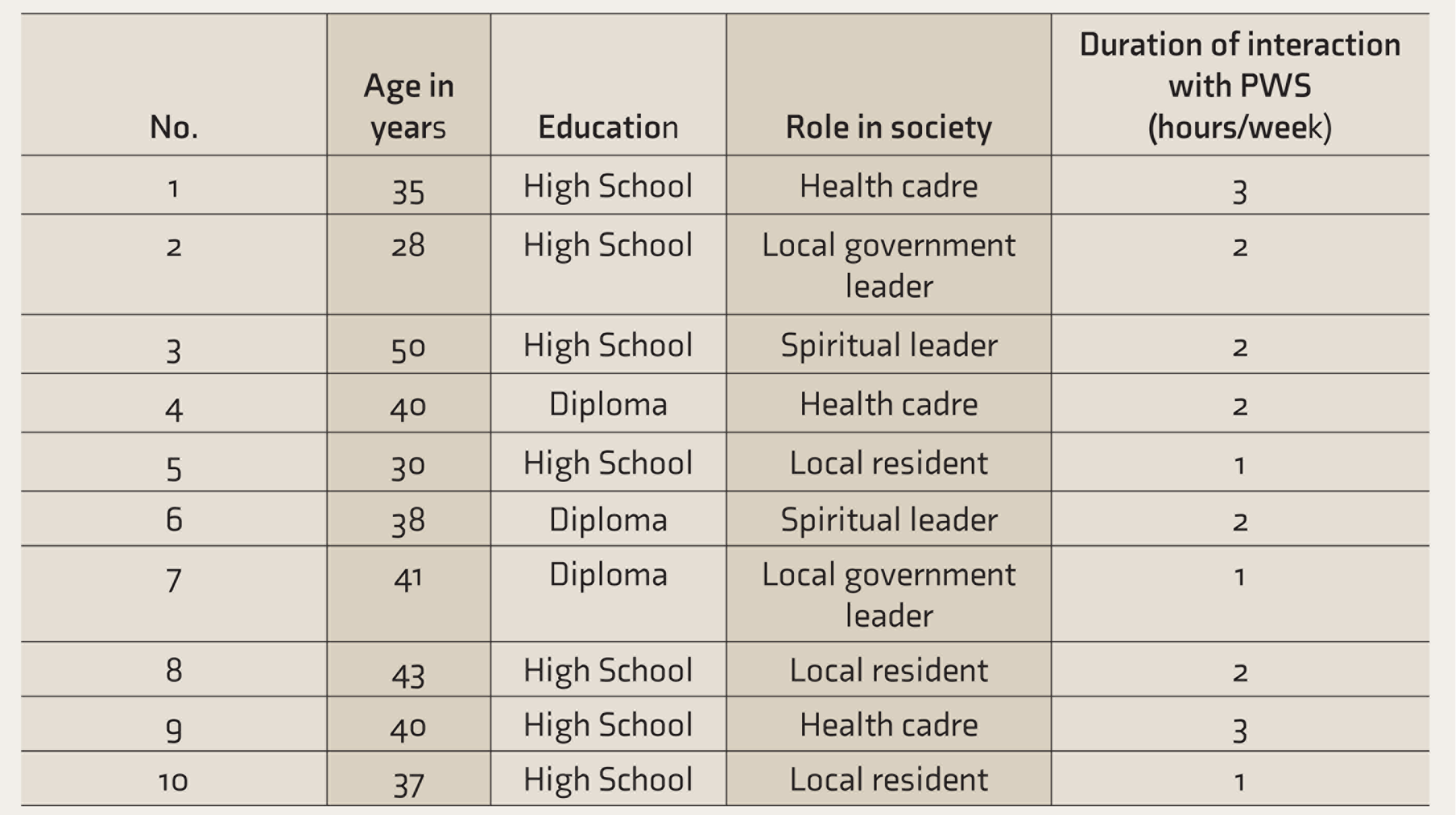
PWS: people with schizophrenia.
Data were collected after receiving permission and ethical clearance. The participants were informed about the study and asked for the willingness to share their experiences. The consent forms included the study aim, the use of the recording device, duration of the interviews, and the right to withdraw from the research at any given time without penalty. The principle of beneficence was attained by the implementation of pseudonyms to reduce the likelihood of revealing the participants’ identities.
There was a briefing on the benefits and risks and, then, opportunities were provided for questions, before conducting the interviews, which occurred at home, based on request. This process spanned approximately 30–45 minutes, and the data were digitally recorded and noted. The following questions were raised:
How do you feel about living near PWS? Why do you think it is difficult to mobilize societies to help PWS? Describe how societies can adapt to PWS.
Rigor was established in this qualitative study by creating four domain strategies, including credibility, dependability, confirmability, and transferability. The development of credibility required the possession of adequate knowledge and skills to perform the designated roles. All the team members engaged in regular meetings to establish confidence in the truth of the research’s findings. Dependability was achieved by creating a well-defined preparation system on details of the study protocol, therefore maintaining the accuracy of coding and the data track record. The triangulation technique is another way to obtain trustworthiness, which involves the confirmation of the study through several data sources, researchers, and theoretical frameworks. Data triangulation was achieved by gathering data using a variety of participants, including neighbors, health cadres, and public figures. 11 Investigator triangulation strengthened the researchers’ standpoint. Thus, the team that conducted this study comprised of researchers from different disciplinary backgrounds, with varying attitudes and motivations. Hence, a combination of diverse professionals helped establish a positive environment to facilitate and ensure successful group communication and effective individual contributions.10, 12, 13 Meanwhile, the provision of all the detailed operational and theoretical data was important in ensuring transferability. 12
The warranty of trustworthiness in an IPA is achieved by seeing things from the participants’ perspectives. Therefore, the transcripts were analyzed in order to ensure data accuracy, up to the point where all researchers met a consensus, as better interpretation is realized by attaining a thorough understanding of the participants’ experiences.
Results
Themes, Sub-themes, and Categories
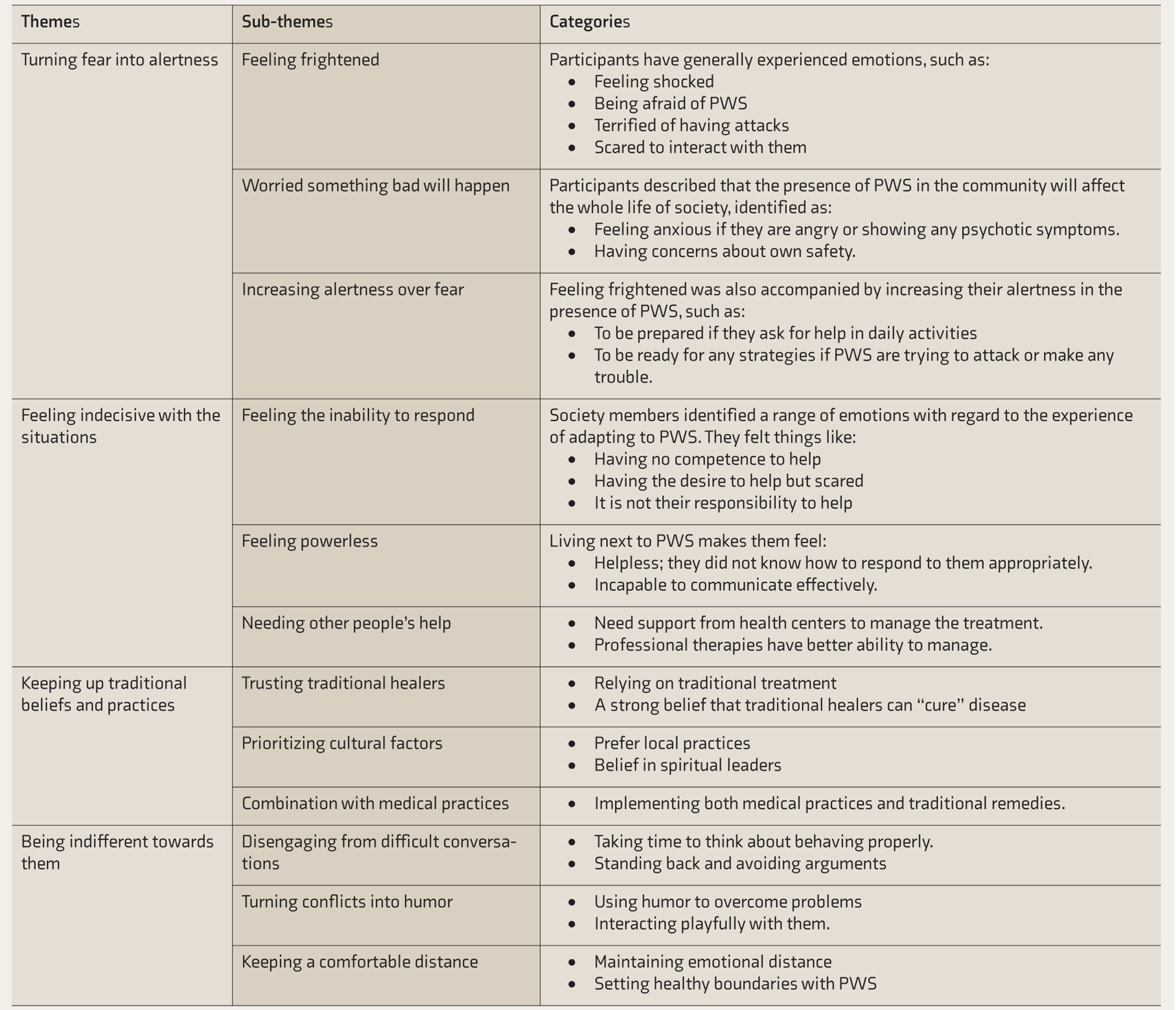
PWS: people with schizophrenia.
Theme 1: Turning Fear into Alertness
Feeling Frightened
The feeling of fright when participants are faced with PWS was described as the fear of being attacked at unpredictable and unexpected situations. Numerous other emotions were experienced while interacting with PWS, including the feeling of shock, conversing with anxiety, terrified of being attacked, and harboring an uneasy feeling. The participants stated the following:
“You know, suddenly he came … I was so shocked, unprepared to engage in a conversation, and did not know what to talk about, because I was alone at the time …. Then he asked for my help, as he needed a job, and I said I had none…. Then he just walked away….” (Participant 5)
“I didn’t know I could be so scared…. People told me to ignore him as he was a dangerous man, with the capacity to give a punch in the face and pull hair…. This took away from me the courage to engage in an interaction….” (Participant 7)
Worried Something Bad Will Happen
Participants described that PWS present in the community affect the entire societal life. This was identified as a feeling of anxiousness when near to patients who are angry or show any psychotic symptoms, hence the need to show concern for safety.
“They make me anxious, and that worsens my inability to interact, due to the expectation of a sudden anger for no apparent reason. Meanwhile, I have no idea of how to deal with the situation, and I do not want something bad to happen….” (Participant 8)
“I just had to think about my own safety. I need the help of someone during an interaction with them, as it is impossible for me to do it alone…I mean it…. Their presence affects our lives and the society, as we sometimes feel a bit worried….” (Participant 10)
Increasing Alertness over Fear
Feeling frightened was also accompanied by an increase in alertness in the presence of PWS. They have to be prepared when PWS ask for help in various activities, even though they feel anxious or afraid. Additionally, they need to develop self-esteem and self-confidence to overcome the fear. Therefore, it needs a proper strategy to overcome the fear and to communicate effectively with PWS.
“Sometimes he asked us to help fix something in his house, because he couldn’t do it alone. Yes…I helped him…. But I also try to overcome my fears…though I can communicate with him…in a better way than other people can….” (Participant 1)
“Our mental health professionals taught us how to interact with them, and to also not force a communication if they were not ready. Therefore, it is necessary to provide a safe space when they are interested in having a conversation. This is important as we need to understand the way they speak, the topic, and how to promote the feeling of comfort during a conversation….” (Participant 9)
Theme 2: Feeling Indecisive with the Situations
Feeling the Inability to Respond
Members of the society identified a range of emotions regarding the experience of adapting to PWS. There was a feeling of deficiency in the level of competence to help, despite the actual desire to render assistance. This occurs because of the fear associated with PWS and a perception that it is not their personal responsibility to help them.
“As neighbors, it is important to render assistance, but I do believe I lack the ability to do so….” (Participant 6)
“Despite the desire to help, I think it was not our duty but that of other members of the society and mental health professionals to provide psychological support, and that should be funded by the government….” (Participant 2)
Feeling Powerless
Living next to PWS caused the participants to feel helpless, as they lacked the ability to respond appropriately and also felt incapable of communicating effectively.
“Sometimes, I feel helpless, being unable to interact when they ask for food, but in a moment, they change the topic to education, and I do not know how to respond…. It is a really difficult experience….” (Participant 6)
“Yes, I know it is difficult to talk to them, and we lack the ability to communicate effectively….” (Participant 7)
Needing Other People’s Help
Participants expressed the need for support from societies to help PWS, as professional therapies deliver treatment with better effectiveness.
“We need to render support, as they need our help to survive, and also the appropriate treatment from mental health professionals….” (Participant 4)
Theme 3: Keeping Up Traditional Beliefs and Practices
Trusting Traditional Healers
Participants lived in rural areas and relied mainly on traditional treatment for the management of mental health issues, following local attitudes and beliefs.
“We live in a rural area…hence the belief in the ability of local traditional treatment to help these people….” (Participant 3)
Prioritizing Cultural Factors
Participants explained that local healing practices were the first attempt to “cure” PWS and the need to believe in the suggestions of spiritual leaders.
“Initially, my neighbor was taken to traditional healers, and the symptoms improved, not screaming at night, and we felt glad…hence…we believe the spiritual leaders’ advices….” (Participant 7)
Combining with Medical Treatments
Managing PWS living in a rural area is not very easy. The participants described the need to implement both medical and traditional remedies in order to manage the psychotic symptoms.
“In this rural society, it is acknowledged that traditional healers can help in most problems…. But we also visit the community integrated health center to get medications….” (Participant 3)
Theme 4: Being Indifferent Towards the Patients
Disengaging from Difficult Conversations
Participants stated that sometimes they need to take a break so that they can plan their responses to the patient appropriately and that, in other situations, it is necessary to stand back and avoid arguments.
“I remember a day when stepping back was the best response for me to his demonstration of anger…and…in another five minutes, we interacted again, and he was fine…yes…we need to create the time to communicate appropriately, in order to gain trust….” (Participant 10)
Turning Conflicts into Humor
Old philosophers report the use of humor as one of the most powerful medicines to support physical and mental health. PWS easily become upset or angry, and this causes muscle tension and emotional outburst. The participants agreed on the ability of humor to help overcome interaction problems.
“One day, I used jokes to release the tension, and he laughed…so we feel…maybe this is a good strategy to foster interactions….” (Participant 9)
Keeping a Comfortable Distance
Maintaining an emotional distance with PWS was described as an effective way to sustain relationships, as people need to set healthy boundaries with PWS.
“There is a need to enhance the feeling of being safe in our presence. Hence, we should learn and try to cope effectively and help them go through the illness…. It is really difficult. However, certain boundaries and safe distance ought to be maintained, and it is also important to enhance the feeling of comfort….” (Participant 1)
Discussion
The findings from this study showed the inability of society to avoid any form of consequences associated with living near PWS, as they have been living together for years, thereby significantly impacting the lives of the entire neighborhood. Furthermore, it is not possible to avoid the consequences as PWS need the help and support of others. The participants believed that it is better to prepare adaptation strategies and to consider effective means to control or react towards the challenges that would be faced in everyday life. Despite the initial negative responses to the presence of PWS, participants make efforts to adapt to the situations, which were supported by local leaders, health cadres, mental health professionals, as well as the local government. Specifically, the health cadres were observed to have better abilities to deal with PWS, compared to other members of the society.
Managing the PWS in the community is the key to living a balanced life, both mentally and physically. In this community, people feel safe, loved, and protected by local resources. People interact with each other to support PWS, assist them in maintaining and gaining independence in daily activities. However, the connection of all these aspects requires the support of society, local government, and policymakers.14, 15 The participants reported that it takes time to gain the confidence to adapt to the consequences of living next to PWS. Improving the understanding of the behavior of PWS was one of the ways to overcome the fear towards them. 16
PWS are affected by a lack of interest in activities, a feeling of disconnection from the reality, difficulty concentrating, avoiding people, hallucinations, delusions, and also disorganized thoughts and speech. This leads to a complete change in the nature of their relationships, and PWS are also challenged by the stigma and discrimination attributed to severe mental illness. In addition, the study participants viewed PWS as dangerous people to be feared. This perceived stigma is common amongst individuals in less dominant groups with low educational achievements and less income. 17
Studies have shown that strong social stigma and discrimination toward PWS cause internalized shame related to the possession of severe mental illness. In addition, a majority of the population tends to harness negative attitudes and beliefs towards PWS, including a perception that they are dangerous and should be avoided.18, 19 A previous study reported that 5.1% of society members avoid mentally ill individuals, while 2.1% treat them in an unfair manner. Establishing a positive attitude after the delivery of an anti-stigma program has been associated with lower odds of avoidance behavior (OR = 0.95, 95% CI = 0.91–0.99, P < .05). 20 Also, a lack of understanding is common in individuals with poor educational backgrounds, those who are unable to seek mental health information, and those with no family history of severe mental illness. 21
Despite the feeling of hopelessness and the absence of competence to help PWS, the community must deliver certain support programs, including activity-based therapies and other health services, for promoting recovery.22–24 A study suggested the need for mental health workers to acknowledge attitudes, values, and beliefs in order to enhance competence and render assistance. 25
Even though the participants felt indecisive, they were still trying to manage the problems, and it made them feel alert to the presence of PWS. Also, members of the rural society depend largely on spiritual leaders for advice and guidance, due to their ability to instill hope, encourage personal and societal development, and improve general wellbeing. Spiritual leaders have a strong ability to motivate oneself and others to enhance productivity and promote positive behavior.25, 26 These are key personalities with regular contact with everyone in the community. Therefore, the participants rely greatly on the spiritual leaders for ideas useful in decision-making.
Inhabitants of the rural area associated the treatment of mental illness with the nature of the illness itself as well as with other traumatic events. 6 In addition, a combination of traditional healing practices and modern medicines is considered effective in managing psychotic symptoms. These include the mixing of complementary and alternative therapies with medical treatment. Conversely, mindfulness, acupuncture, yoga, light therapy, and herbal medicines have also been adopted in the maintenance and improvement of mental health, while occupational therapy is used to facilitate better social interactions.27–29
Use of humor is one way to reduce tension during interactions with PWS. This valuable strategy is frequently adopted to promote coping with stressful life events, and also to enhance interpersonal relationships, grow communication skills, manage conflicts, and improve coping strategies. Furthermore, there is also a possibility of adopting humor in maintaining social relationships and building social bonds between PWS and other society members.30, 31
Participants agreed that a huge amount of time is required to build relationships with PWS. Avoiding arguments with PWS was quite common in the culture, and it made PWS feel comfortable during interactions. In addition, a disposition of indifference was recognized as a common way to deal with difficult situations, despite the fact that they still helping PWS with daily activities. 32
Studying the techniques the society uses to adapt with PWS would reveal possible ways to overcome social barriers in community treatment. Furthermore, it is possible to achieve better results from mental health programs by working together with the society to create a supportive environment and reduce the stigma. 33 Also, an adaptive society is characterized by five essential components, including community safety, social bonding, justice, identities and functions, as well as purpose in life. 34 There is a likelihood of improving these outcomes by collaborations with health care institutions, stakeholders, and policymakers.
Limitations of the Study
The results of the study were very positive. However, due to the limited scope of observation in a local area, there is a possibility that these findings are not translatable to other societies with a higher level of social capital to support PWS. However, the results can possibly be helpful for PWS worldwide. Additionally, the maximum length of interaction that the participants had with PWS in this study was only three hours/week, so this might be a very short period of interaction compared to living with PWS. Further study is recommended to interview families living with PWS to understand their experiences, views, thoughts, and feelings, to help us understand how to deal with PWS appropriately.
The members of the society possessing negative experiences and engaging in less frequent interactions with PWS perhaps experience a range of emotions, including anger, frustration, and security-related issues. Meanwhile, individuals with positive experiences tend to have had longer interactions and have also been more willing to communicate personal experiences.
Conclusions
Societal adaptation to PWS focuses on understanding the means to deal with the uncertainty and complexity, alongside creating environments that support mental health and wellbeing. Therefore, communities are recommended to improve the strategies adopted in addressing care for PWS, which ought to be supported by integrated mental health system, stakeholders, and the entire healthcare system. This study examined the adaptive experiences of societies within a limited geographical area, hence the suggestion that future research include samples from families living with PWS in this area to gain the most relevant insights. Accordingly, future studies can address the same topic in different settings, location, and/or culture of a wider region or be expanded to a multi-state analysis.
Footnotes
The authors declare that there are no conflicts of interests regarding this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.