
Abstract
Background:
The Affiliate Stigma Scale (ASS) is a widely used tool to measure affiliate stigma in the caregivers of individuals with various types of mental illnesses. However, the Hindi adaptation of this scale with evident psychometric properties is not available. This study aimed to adapt the ASS in the Hindi language and, further, to validate it in the Indian setting.
Methods:
Translation and back-translation methods were used to translate the original items of the ASS to the Hindi language. After completion of translations and linguistic adaptation process, the Hindi translated version of the ASS, WHO Quality of Life-BREF (WHOQOL-BREF), General Health Questionnaire-12 (GHQ-12), and Hospital Anxiety and Depression Scale (HADS) were administered to 140 caregivers of persons with mental illness. Purposive sampling method was adopted. The age range of the participants was 17–60 years. Psychometric properties, as well as the factor structures of the scale, were evaluated.
Results:
The Hindi version of the ASS has adequate internal consistencies (r = 0.87–0.93) and test–retest reliability (r = 0.78, P < 0.001). The concurrent validity of this scale was also high, as the correlation coefficients among the Hindi version of the ASS, WHOQOL-BREF, GHQ-12, and HADS were ranging from 0.23 to 0.35. The exploratory factor analysis revealed three underlying factors, namely, cognition, affect, and behavior.
Conclusions:
The Hindi version of the ASS is a reliable and valid psychometric tool to measure affiliate stigma in caregivers of patients with mental illness.
The Hindi version of the ASS is a comprehensive and efficient tool to measure affiliate stigma among caregivers of individuals with various mental illnesses. Given that the internalized form of stigma negatively impacts the psychological health and well-being, this scale might be useful to understand the role of stigma on health outcomes in clinical as well as research settings.Key Messages:
As a result, many times, family members internalize this public stigma and consequently experience stress, guilt, embarrassment, shame, helplessness, inferiority, etc.2, 3 This kind of internalized form of stigma is conceptualized as “affiliate stigma (AS)” by Mak and Cheung. 4 AS negatively affects the health status of caregivers and gradually diminishes their quality of life (QOL). There are very few Indian researchers, such as Banga et al. and Patra et al., who conducted empirical research in the area of AS among caregivers of PMI.5, 6 Unavailability of valid and reliable tools in the Hindi language to measure AS could be one of the major reasons behind the scarcity of research on this topic.
Mak and Cheung developed the Affiliate Stigma Scale (ASS) to measure AS. 4 The scale is widely used and comprises cognitive, affective, and behavioral components of stigma. The applicability and proficiency of this scale can be gauged by the fact that the scale’s translation and adaptation have been done in different languages, for example, Persian, Hebrew, Amharic, Chinese, and Malay.7–11 The ASS has also been validated and utilized to measure internalized stigma in the caregivers of individuals with different mental illnesses such as dementia, Alzheimer’s disease, and autism spectrum disorders.10, 12–14 However, the Hindi adaptation of this scale is yet to be done. Additionally, there is a lack of a Hindi psychometric tool with evident and valid psychometric properties to measure AS in the caregivers of PMI. Therefore, this study aimed to translate and validate the ASS in the Hindi language and further analyze its factor structure.
Materials and Methods
Sample
The study was approved by Institutional Ethics Committee. It was conducted at the Central India Institute of Mental Health and Neurosciences, Rajnandgaon, Chhattisgarh, using a cross-sectional design. The sample consisted of 140 first degree relatives of patients with schizophrenia, of the age range of 17–60 years. Purposive sampling technique was used. Only those participants who gave written informed consent were included. The following inclusion criteria were followed: (a) Educated up to 8th grade, (b) Could read and comprehend the Hindi language properly, (c) Living with the patient for at least six months, and (d) Actively involved in fulfilling the patient’s needs. Those with a history of mental retardation, epilepsy, major psychotic disorder, or any significant neurological disorder were excluded. The sociodemographic as well as clinical details of the participants were recorded in a sociodemographic and clinical datasheet specially drafted for this study. Based on the said inclusion and exclusion criteria, 95 males and 45 females were selected.
Tools
Procedure
First, permission for the Hindi adaptation and psychometric evaluation of the ASS was taken from the original authors. After that, six bilingual professors proficient in Hindi and English languages were selected for the linguistic adaptation of the scale. All the experts were having previous experience of translation and back-translation of questionnaires or inventories. Forward translation work was carried out by three professors of psychology who were aware of the concept and purpose of the questionnaire. Afterward, forward-translated items were presented to another three professors for back-translation. To avoid biases, the back-translation work was given to translators who were not aware of the original English version of the scale. Lastly, the original ASS and translated versions were reviewed together for incongruities, if any. The backward-translated version did not show any notable difference regarding meaning from its original version. There were no culture-sensitive items in the scale; therefore, no culture-specific modification was done. After completion of the translation work, the psychometric evaluation of the Hindi translated version was started (see supplementary file). For this purpose, the Hindi version was administered on the participants along with WHOQOL-BREF, HADS, and GHQ-12. Lastly, to check the temporal stability, the Hindi version of ASS was re-administered to 48 participants after a gap of two months.
Statistical Analyses
The IBM Statistical Package for the Social Sciences, version-19, was used to analyze the obtained data. Cronbach’s alpha coefficient and test–retest coefficient were calculated to assess the reliability of the scale. Pearson’s correlation coefficients were computed to estimate the concurrent validity. Lastly, exploratory factor analysis was conducted to determine the factor structure of the scale using the principal component analysis method. Initially, sample adequacy for factor analysis was tested using Kaiser–Meyer–Olkin measures and Bartlett’s test for sphericity. The Bartlett’s test of sphericity was calculated to test the overall significance of all the correlations within the correlation matrix. The Kaiser–Meyer–Olkin measure of sampling adequacy was tested to estimate the strength of the association among the variables. After that, the scree plot was used to know the possible number of factors suitable to retain. The factors that had eigenvalues >1 were retained in the analysis. 18 The unrotated factor component matrix was rotated using varimax rotation with the criteria of factor loading >0.40, recommended by Hair et al. 19 Finally, the cut-off point for the low, moderate, and high level of AS was derived from the percentile distribution of the scores.
Results
Sample Characteristics
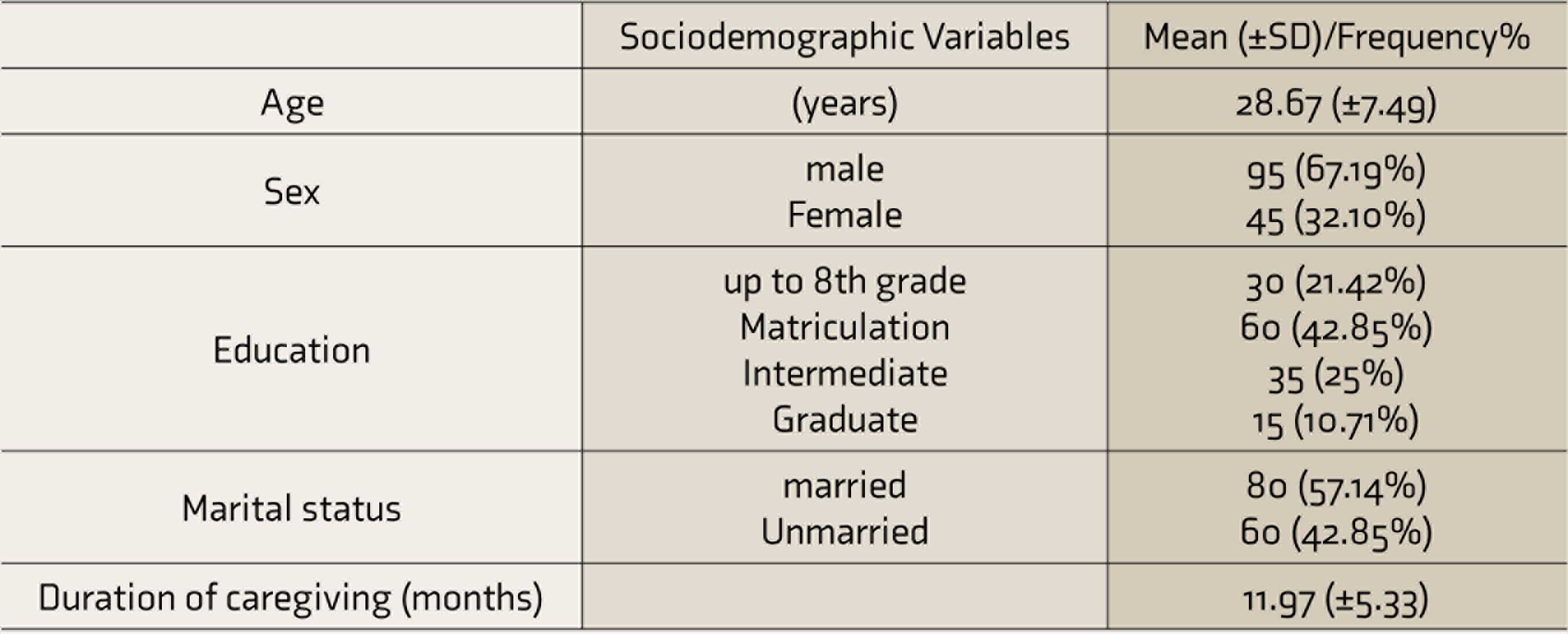
The mean (±SD) age of the participants was 28.67 (±7.49) years. Most of the participants were married (57.14%) and educated up to matriculation level (42.85%). The mean duration of caregiving was approximately 11.97 (± 5.33) months (
Sociodemographic Profile of the Participants
Reliability
Internal consistencies of the scale, as well as its subscales, were assessed by using Cronbach’s alpha coefficient.
The obtained high Cronbach’s alpha coefficient values for affect (α = 0.87), behavior (α = 0.90), and cognition (α = 0.89) subscales, as well as the full scale (α = 0.93), indicate the ASS has adequate internal consistency.
Validity
Correlation of the Hindi Version of the ASS with Measures of QOL, General Mental Health, Anxiety, and Depression

ASS: Affiliate Stigma Scale; QOL: Quality of Life, WHOQOL-BREF: WHO Quality of Life-BREF Scale, GHQ-12: General Health Questionnaire-12, HADS: Hospital Anxiety and Depression Scale.
The obtained correlation coefficient values indicate a substantial amount of concurrent validity of the scale. Scores of the ASS were found to be significantly positively correlated with the score of GHQ-12 (r = 0.23, P = 0.005) and HADS (r = 0.35, P < 0.001). Results imply that higher level AS is associated with greater anxiety and depression, as high scores on the ASS indicate more AS, whereas high scores on HADS reflect more anxiety and depression. Similarly, a higher score on GHQ-12 indicates poor mental health, which means a higher level of AS is related to poor mental health. Moreover, scores of the ASS were negatively correlated WHOQOL-BREF (r = -0.30, P < 0.001); high scores on QOL indicate better overall well-being. The findings further indicate that caregivers who have a low level of AS experience fewer symptoms of anxiety and depression and have better overall health and QOL.
Initially, principal component analysis extracted 22 unrotated factors. The factors that had eigenvalues >1 were retained in the analysis.
18
It is evident from the scree plot (
Scree Plot, Depicting Factors with Their Eigen Value
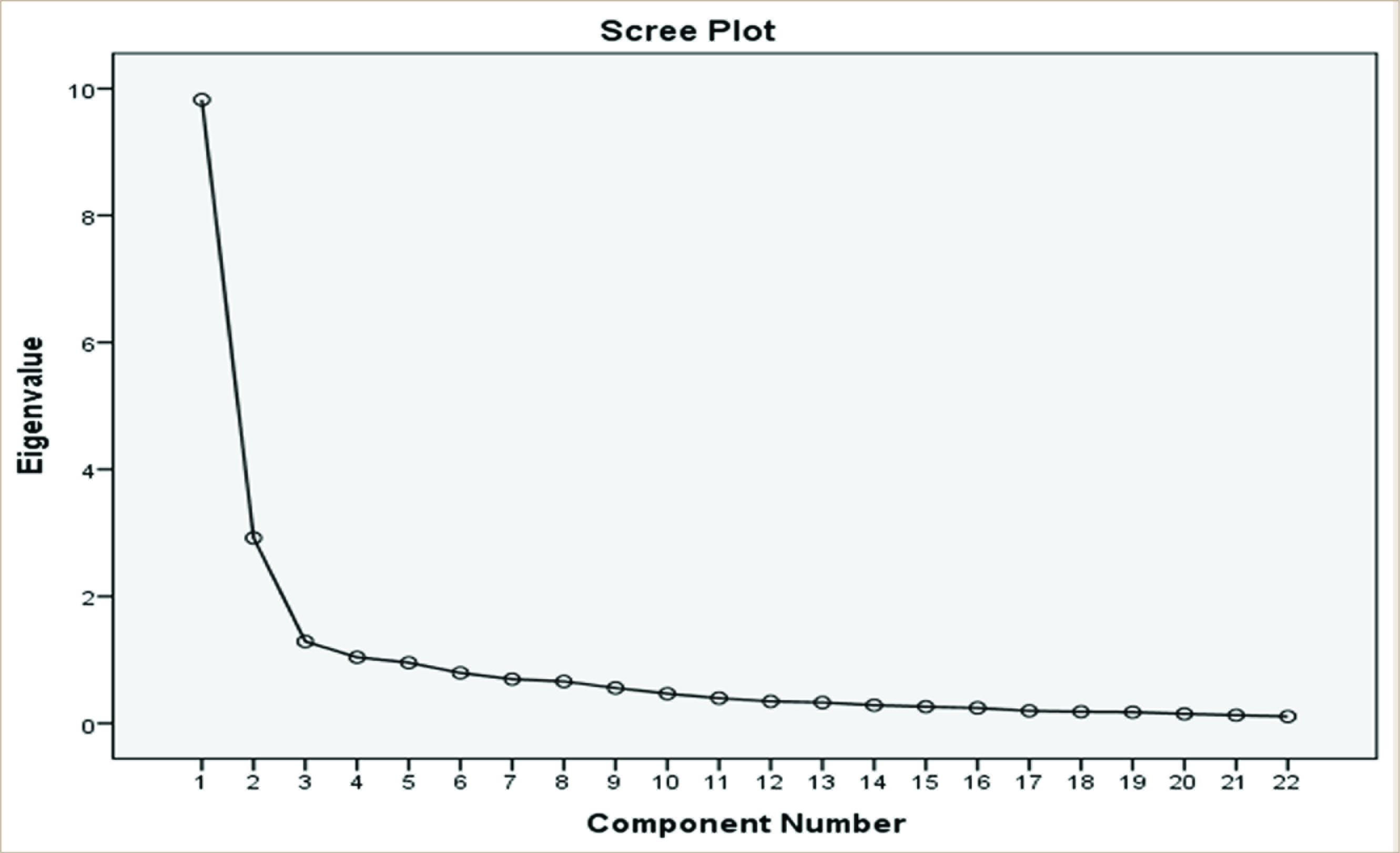
Varimax rotation, with the criteria of factor loading >0.40 recommended by Hair et al. and Field,19, 20 indicated three distinct factors underlying the items of the Hindi version. All the 22 items, with their respective factor loadings, have been presented in
Item Factor loadings for Exploratory Factor Analysis Using Varimax Rotation Method (n = 140)
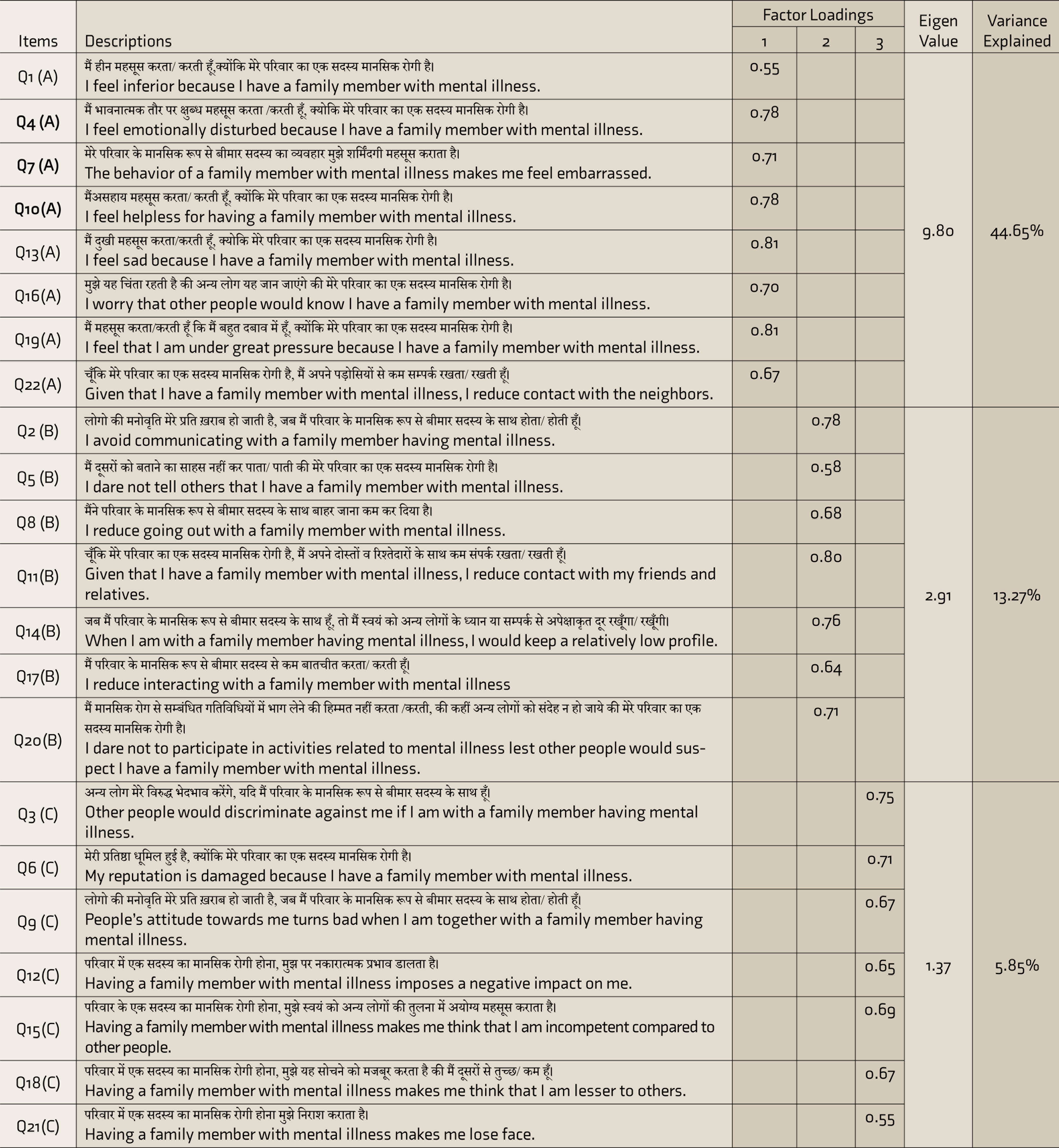
A: affect, B: behavior, C: cognition.
The first factor was labelled as “affect,” due to the higher loading by the items related to “affective” aspects of AS, for example, “I feel sad because I have a family member with mental illness.” This first factor accounted for 44.65% of the total variance. The second derived factor was labelled as “behavior” because of the higher loadings by the items related to behavioral aspects of AS like, “I avoid communicating with a family member with mental illness.” This factor emerged to explain 13.27% of the total variance. The third factor was named as “cognition,” as all the highly loaded items on this factor were about cognitive aspects of AS such as “Other people would discriminate against me if I am with the family member with mental illness.” This factor shared a total of 5.85% variance. Altogether, these three factors explain 63.78% of the total variance (
Finally, the cut-off points of the scale were derived from the percentile distribution of the scores. Based on the total scores of the obtained data, the 33rd and 66th percentiles were considered as the cut-off points to identify low, moderate, and high scores for AS. The 33rd percentile was used as the low AS score cut-off, and the 66th percentile was used as the high AS score cut-off. The range of values between the low and the high score cut-offs denotes moderate AS level. The 33rd and 66th percentile are taken as the cut-off point because these two tertile points divide the population into three equal subgroups and help in categorizing them as high, moderate, and low scorers. 21 Also, this classification method is commonly practiced in psychological research to determine the cut-off points of a scale.22, 23
Based on these three percentiles, a score of ≤55 reflects a low level of AS, a score of 56–62 reflects a moderate level of AS, while a score of ≥63 suggests a higher level of AS.
Discussion
This study was conducted with twofold objectives; first, to adapt and validate the ASS in the Hindi language, and second, to explore its factor structure. For the linguistic adaptation of the present scale, forward and backward translation methods were used.24, 25 The translation was done with a focus on conceptual and cross-cultural equivalence rather than mere literal similarity, as per the recommendations of Phongphanngam et al. 26
The Hindi version of the ASS was found to be a reliable and valid scale. The analysis of the data offered an acceptable range of Cronbach’s alpha values for the full scale as well as its subscales. It shows that the items of the Hindi version of the scale are homogeneous and significantly correlated with each other. These findings are consistent with the results of Mak and Cheung, Chang et al., and Yun et al.4, 10, 11 Further, high consistency between the scores of the test and retest phases suggests the temporal stability of the Hindi version of the ASS. The present finding is consistent with the findings of the Persian validation study of the ASS conducted by Saffari et al. 12 Overall, it can be inferred that the items of the scale are reliable to assess the various underlying components of AS.
The concurrent validity of the Hindi version was assessed by correlating its score with different valid measures of general mental health, QOL, anxiety, and depression. Earlier research findings highlight that the family members of psychiatric patients come across various types of negative emotions and experiences during the whole process of caregiving to the PMI, which often results in internalizing stigma. 10 A person with a higher level of AS experiences negative effects such as shame, guilt, sadness, and inferiority. These negative emotions gradually cause depression and anxiety and lead to reduced QOL.10, 27, 28 Hence, measures of general mental health, QOL, anxiety, and depression were considered for measuring concurrent validity of this scale.
As expected, a significant negative correlation was obtained between the scores of the ASS and WHOQOL-BREF. On the other hand, the scores of the ASS were found to have a significant positive correlation with the scores of HADS and GHQ-12. It illustrates that an individual with a higher level of AS experienced a reduced QOL and poor well-being. The present findings are similar to the findings of Chang et al. and Saffari et al.10, 12
These results provide evidence for the concurrent validity of the Hindi version of ASS. However, it is important to note that the correlation coefficient values among the scores of these tests are significant but moderate in strength. These moderate correlation coefficients can be the result of the fact that an individual’s QOL, general health, and overall well- being are affected by several other factors as well.
Further, an exploratory factor analysis provided three-factor solutions for the Hindi adaptation of the ASS. The three factors obtained were similar to the factors reported by Mak and Cheung, namely, cognitive, affective, and behavior factors. 4 This three-factor solution of the scale was also claimed by several other researchers.8, 10, 12
Lastly, it was found that a considerable portion of family members of PMI experienced moderate to high level of AS. These findings are consistent with the findings of Thara and Srinivasan, as they have also reported a large number of primary caregivers of schizophrenia patients to experience stigma and discrimination. 29
Further, various studies have found that a higher level of AS consequently leads to various positive symptoms of psychosis, depression, and poor mental health. Hence, this scale could be useful for the identification of individuals with a higher level of AS who are likely to develop mental health issues, so that proper intervention could be provided to them in time.
Although this study will be useful for clinicians and mental health workers in measuring caregivers’ AS, it has certain limitations. Firstly, the sample size was relatively small. Also, the cross-language equivalence of the scale was not evaluated. The Hindi version was validated only for the family members of PMI. Therefore, this tool can be validated for caregivers of terminally ill patients such as those with HIV/AIDS, leprosy, tuberculosis, etc., in future studies.
Conclusion
The Hindi version of ASS is a reliable and valid psychometric tool to measure AS among Hindi-speaking caregivers of PMI. It is a comprehensive Hindi scale to assess the cognitive, behavioral, and affective components of internalized stigma. This scale would be very useful and effective for clinicians as well as researchers working in the area of caregivers’ well-being, especially in the Hindi-speaking zones.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Hindi Adaptation and Psychometric Validation of the Affiliate Stigma Scale by Rajbala Kumari, Jay Kumar Ranjan, Saroj Verma, Hari Shanker Asthana in Indian Journal of Psychological Medicine
Footnotes
Data Sharing Statement
Deidentified individual participant data (including data dictionaries) that underlie the results reported in this article (text, tables, figures, the informed consent form, and the statistical analysis plan) will be made available for wider use. The data will be made available upon publication and for lifetime, to the researchers who provide a methodologically sound proposal for use in achieving goals of the approved proposal. All available data can be obtained by contacting the corresponding author. Proposals should be submitted to jaykumarranjan@gmail.com.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.