
Abstract
Objective:
A scoping review was conducted to detect the factors that affect family retention (FR) or involvement (FI) in the treatment of persons with severe mental illness (PwSMI) and to understand the gaps in this research area.
Design:
We included studies that described factors associated with FR/FI in the treatment of persons with PwSMI. English language articles available in full text, published until June 2022, were included. The literature search was carried out in four major electronic databases, such as PubMed, Scopus, ProQuest, and EBSCOhost, for 6 months from January 2022 to June 2022, which yielded 5442 articles, of which six (four primary studies and two secondary studies) were considered for the final scoping review as per the inclusion criteria.
Results:
Five major categories of factors were identified: (a) family level, (b) professional level, (c) mental health system level, (d) related to characteristics of the patient and illness, and (e) related to the external environment. Most studies described barriers to FI, while only a few elaborated on facilitators for FI/FR. Systemic and family-level factors were the major contributors to the barrier to FI and FR in the treatment of people with PwSMI.
Conclusion:
There is a dearth of literature in the field of FR/FI in the treatment of people with schizophrenia. More research is required so that holistic interventions can be designed and provided.
Retention in treatment is defined as completing or continuing the course of treatment advised by the clinician. 1 Family retention (FR) refers to family members ensuring service delivery and remaining in the mental health services offered. 2 Similarly, family involvement (FI) in mental health services has been broadly defined as the availability of family members and the accomplishment of various tasks by them at different levels of intervention, from basic assessment and educational intervention to higher levels such as family therapy. 3
FR/FI in mental health services represents a critical practice issue, especially in the case of persons with severe mental illness (PwSMI), where treatment is long-term and costly. 4 Families maintain considerable control over many aspects of the treatment process, PwSMI (PwS): recognizing the disorder/assisting consultants for diagnosing the disorder, outpatient consultation, record keeping, admissions, inpatient care, discharge, and continuing care. In the case of schizophrenia, nonadherence to the treatment is 41.2%, 5 which eventually puts the patients at risk of re-hospitalization and increases the burden of treatment costs. 6 Although the importance and benefits of FI in mental health are recognized globally, many factors still hinder its optimal utilization.7–11 Even if families are initially motivated to seek mental health services, a myriad of experiences can interfere with the treatment process, leading them to disengage or drop out prematurely. However, very little information is available on the factors associated with the retention or involvement of family members in the treatment of PwSMI.
Understanding the factors associated with family retention or involvement in the treatment of PwSMI will contribute to how a clinician can support such families and patients and eventually enable them to remain in treatment. Past research in the area of FR/FI has heavily focused particularly on child psychiatry, adolescent mental health, and substance abuse disorders.12–18 It is unclear what kind of information is available in the literature about the underlying factors that impact the family’s decision to remain involved in the PwSMI. Hence, this study aimed to provide broad overview of evidence on the factors associated with FR/FI in treatment of PwSMI. To achieve this, a scoping review was conducted.
Methods
We followed the Preferred Reporting for Systematic Review and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR). 19 Our primary research question was What factors impact family retention or involvement in the treatment of PwSMI?
The inclusion criteria and the main question were converted into a Population-Concept-Context (PCC) framework to guide the scoping review. 20
Population
We included studies with participants who were caregivers, relatives, or family members of PwSMI, from any gender, culture, and ethnicity, availing of mental health services. Studies describing factors affecting family retention or involvement from patients, families, or mental health professionals’ perspectives were also included.
Concept
All factors describing FR or FI in the treatment of PwSMI were considered key concepts. This included primary and secondary studies, including intervention-focused ones, that described factors in this direction. To widen the scope of this review, we also included studies with severe mental illness, which includes mood disorders, psychosis, and schizophrenia. We also included studies that did not mention the details of the participants’ diagnoses in detail but mentioned severe mental illness. However, studies that focused on drug adherence, patient participation, or retention were excluded.
Context
We included studies and reviews done in mental healthcare settings (e.g., inpatient care, outpatient services, long-term care, and community care), the methods applied are qualitative and quantitative, and the studies were published until June 2022 and available in the English language with full text.
We excluded protocols, recommendation letters, and concept papers.
Search Strategy
The literature search was conducted between January 2022 and June 2022 on PubMed, Scopus, ProQuest, and EBSCOhost. Detailed search strategies are described in the online-only supplementary file Appendix A.
Study Selection
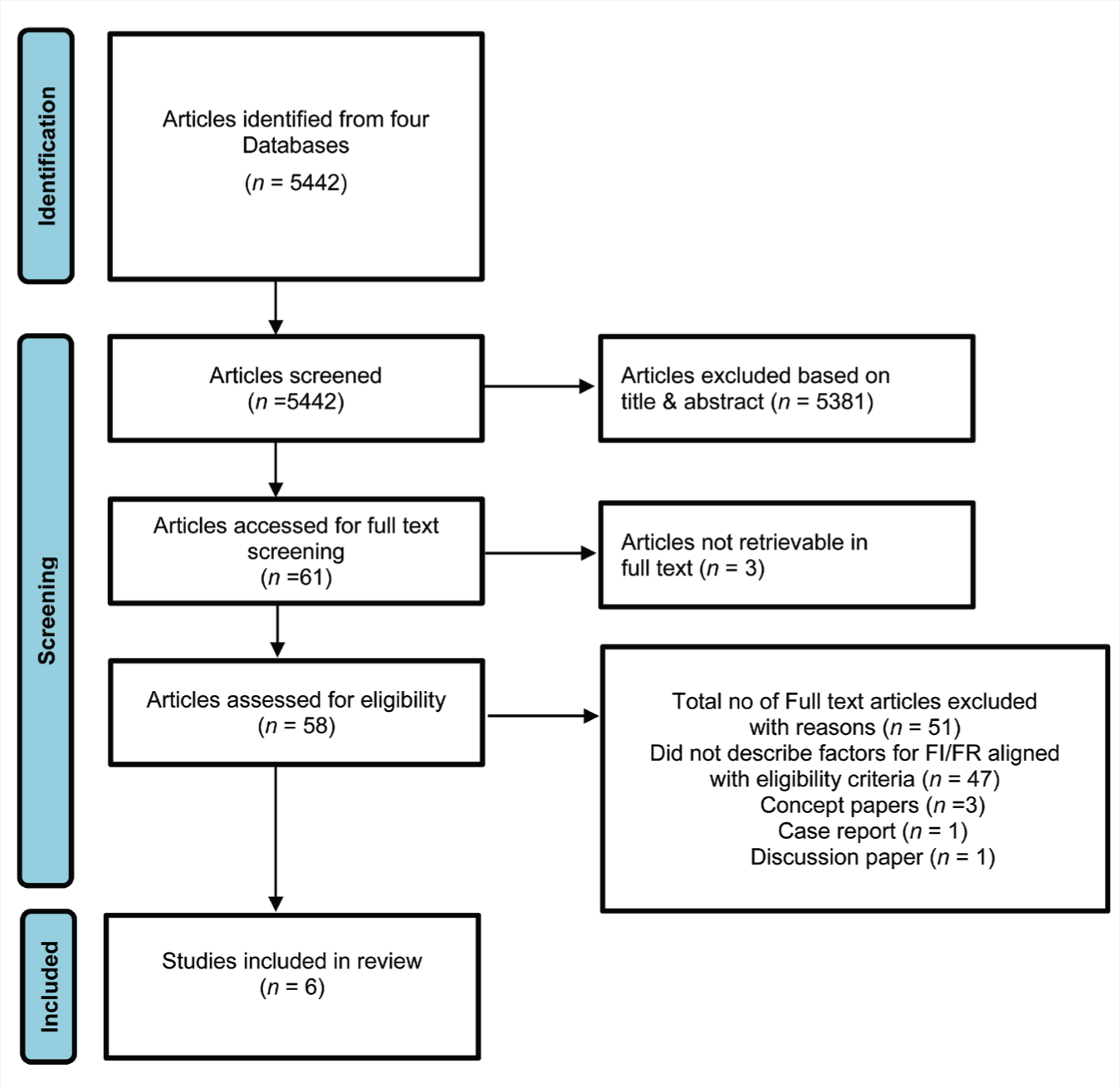
The first author did the literature search and manually screened the titles and abstracts of articles to check against the inclusion criteria. After excluding articles that did not meet the inclusion criteria, 61 remained. The first, second, and third authors assessed their full texts to consider them for final inclusion in the review. Disagreements among the authors were resolved through discussions. The screening process is documented in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement, 19 along with reasons for exclusion, in Figure 1.
Data Extraction
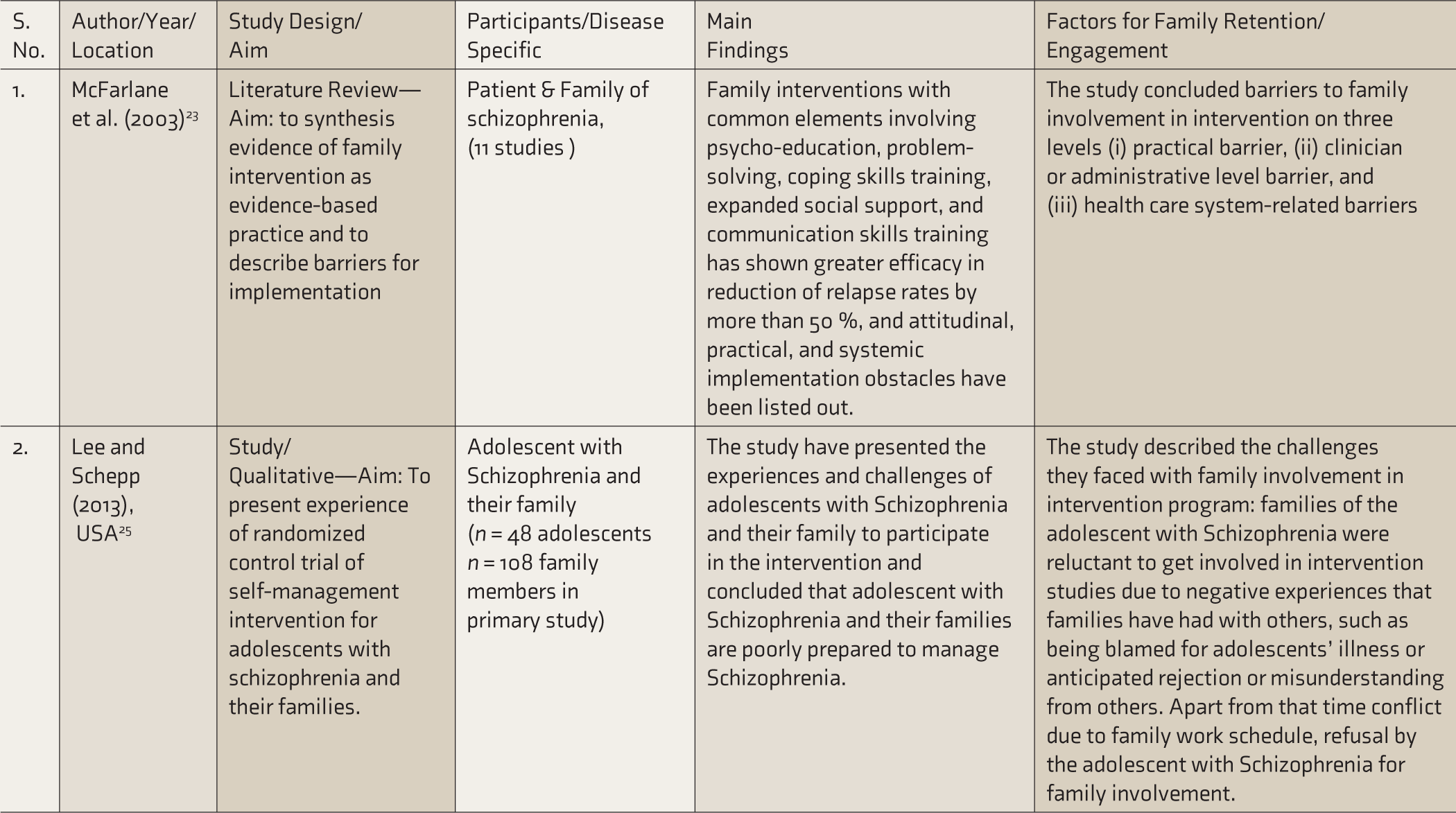
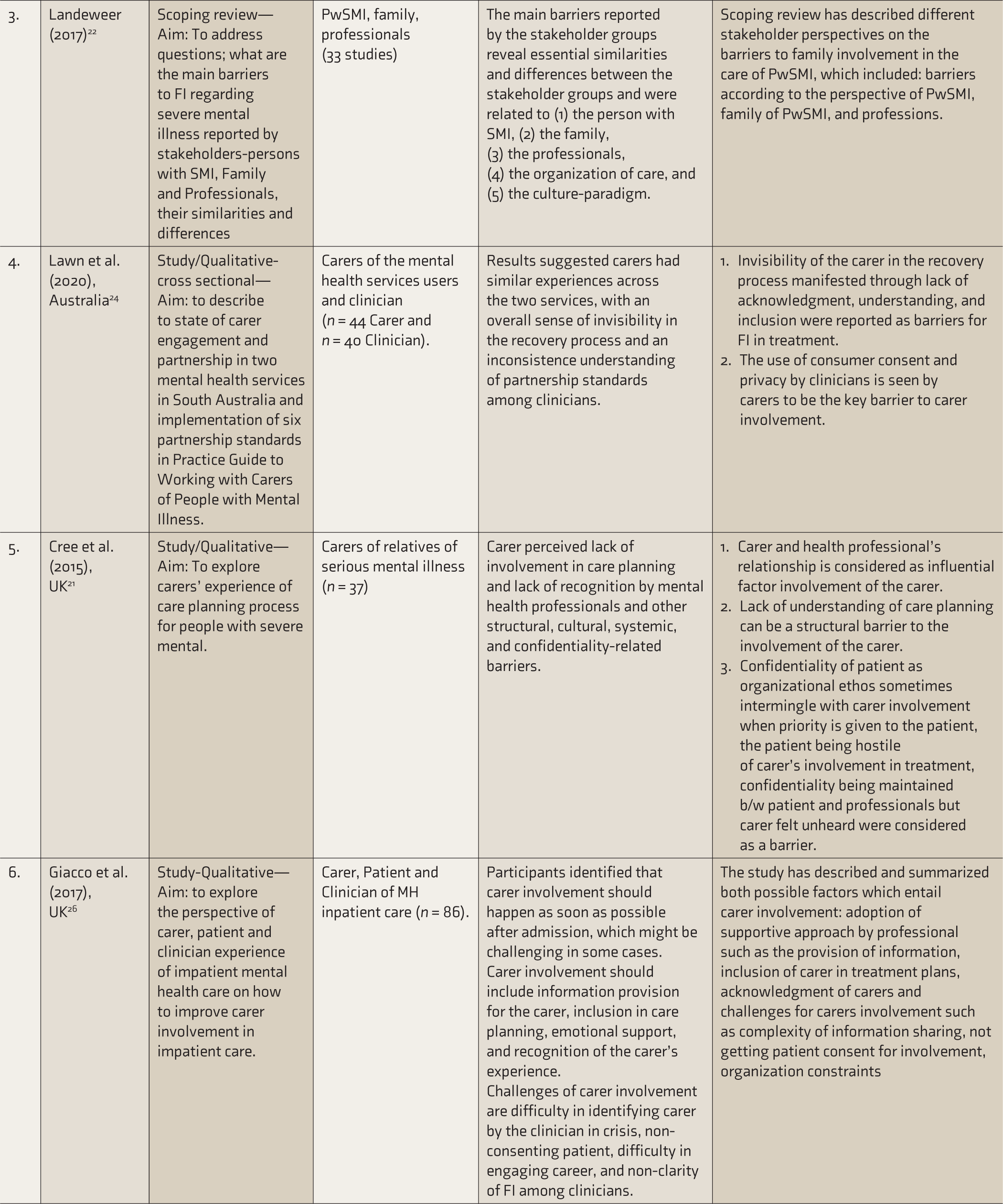
The charting table was developed after discussion and consensus among all the authors. The most relevant data extracted and included were author/s, year of publication, the country where the study was conducted or published, design/method of the study, the aim of the study, study participants and sample size (if applicable), main finding, and findings related to this scoping review; the details are provided in Table 1.
Study Inclusion Process.

Results
Study Inclusion
The search terms “Factors AND Family Retention OR engagement AND Schizophrenia AND treatment” were used in the multiple databases depicted in Appendix A, along with Boolean operators. The details of search results among each database are depicted in Table 2. The entire process of study inclusion is depicted in Figure 1.
# PRISMA, Preferred Reporting for Systematic Review and Mata Analysis Extension for Scoping Reviews.
Overall, six studies were eligible for final inclusion in this scoping review. The description and summary of these studies are presented in Table 2.
Studies on Factors Associated with Family Retention or Involvement in Treatment of Persons with Severe Mental Illness.
PwSMI, persons with severe mental illness; FI, family involvement; MH, mental health.
We have summarized the factors that influence FR or FI in the treatment of PwSMI in five categories: (A) family level, (B) professional level, (C) mental health system level, (D) related to characteristics of patient and illness, and (E) related to the external environment.
Family Level
This category is further divided into two aspects: (i) knowledge and understanding of family and (ii) expectations and experiences with the service provider.
(i) Knowledge and Understanding of Family: Family members play a crucial role in the process of treatment and family retention. Many studies revealed that their lack of knowledge and understanding would adversely impact the treatment of patients. Additionally, the lack of information on the benefits of FI and how it works and impacts the treatment of patients has been reported as a barriers to FI. Studies revealed that the family members’ misunderstanding of the illness could hinder the FI.21, 22 Another factor in this category is family members’ low self-competence; whether they are capable of getting involved in the patient’s treatment and whether it will be harmful to the patient’s treatment if they get involved such doubts about self-ability would have hindered FI. 22
(ii) Expectations and Experiences with Service Provider: Families’ expectations, both low and high, regarding the outcome of FI in treatment hindered FI in treatment.22, 23 Additional barriers included the family’s unwillingness or poor motivation to be part of treatment and they are not getting involved in treatment so as to keep family secrets. 22 Families reported that their experience in dealing with PwSMI has not been acknowledged or respected, leading them to be uninvolved in treatment.22, 24 One review suggested that the family members were not offered or provided with the proper information or rendered services by the professionals, which hindered FI. 22 Many intervention studies reported that family members had negative, unpleasant experiences and dissatisfaction with service providers. Furthermore, family members reported that while involved in treatment, they felt that the service providers considered them to be responsible for the patient’s illness. Family members’ such experiences with service providers hinder FI.23, 25
Professional Level
The professionals’ supportive approach, such as validation of caregivers’ emotions, reassurance, empathy, and maintaining a positive relationship while dealing with family, would facilitate FI.21, 26 Professionals’ competence was a significant factor in the family involvement; skills in dealing with family’s emotions, poor retention of skills to work with family learned in the training period, self-doubt, and communication skills required to build successful relationships in the complex family issues, lack of such competence among professionals were considered a major barrier for FI/FR.22, 26 The lack of experience of professionals in family intervention was considered the major barrier to FI. 22 Professionals’ low expectations and unawareness of benefits from family involvement and they perceiving it as a time-consuming and costly service were the other barriers.22, 23 Professionals’ stand on theories about psychodynamic and family pathogenesis and their persistent use during clinical practice would have been perceived by the family members as blame for the patient’s illness, resulting in family disengagement from the FI. 23
Mental Health System Level
This category is further divided into two aspects: (i) organizational practice- related factors and (ii) service delivery- related factors.
(i) Organizational Practice-Related Factors: The usual practice of MH organizations and practitioners is to maintain confidentiality between patients and professionals while including family members in the treatment of PwSMI. It is a dilemma for professionals whether to share some of the information with the family members or not; the patients want privacy, and the professionals do not want to compromise on that to maintain the therapeutic relationship with the patient. Consequently, maintaining confidentiality became a barrier, according to most studies.21–23,26 Many families reported that MH services are more patient-centric. Families have not given much attention to the treatment and management of PwSMI, which keeps them from getting involved in their treatment.22, 23, 26 While practicing family involvement, professionals and caregivers both have reported power struggles as being a barrier. The caregivers perceived that the professionals’ attitude is superior and that their own opinion and experience in looking after the patient would not be considered, thus hindering them from FI. On the contrary, while working with families, professionals felt over-involvement and interference by the caregiver in the direction of treatment, which also hindered FI.21, 22 Inter-professional struggles have been reported among the treating team about who should take the lead role in FI. Several studies report that the psychiatric nurse, psychiatric social worker, and psychiatrist have difficulty in determining what kind of role they should have with the families. Such role confusion might hinder FI.22, 26 The reviews have documented the traditional organizational practice as non-accommodative for FI/FR as it differs from the organization’s primary goal or is unable to prioritize FI/FR in practice.22, 23
(ii) Service Delivery-Related Factors: Families in the majority of studies have reported that the lack of clarity on the accessibility of information regarding the treatment of the patient, as well as FI, has discouraged them from being involved in the treatment.23, 24, 26 Many studies have reported that professionals face dilemmas in sharing information while practicing family involvement with caregivers. Moreover, professionals feel indecisive on how much information should be shared, what information should be shared, and what not to be shared with the family members in a manner that does not interfere with the confidentiality or autonomy of the patient. Many times, non-consent by the patient for family involvement hindered FI. In short, the complexity of information sharing and non-consent by the patient have been reported as significant barriers to FI. Professionals keep the attitude that during FI, most responsibility should be taken up by the caregivers, and the caregivers perceiving the intervention as an additional responsibility are other barriers.22, 23 In a study, patients and families reported that choosing the timeframe of offering FI is crucial; according to the clinical situation of the patient, some preferred the time of admission, while others preferred a later time when the caregivers are involved in long-term treatment. 26 Studies have also demonstrated that mental health professionals, in their routine practice, fail to recognize the primary caregiver and assign the role of caregiver to that identified member of the family with mental illness for uninterrupted care; this could be a barrier to FI. 26 Similarly, many studies have reported the lack of resources available to the organization as a barrier, such as the lack of well-trained human resources to deal with the family, a lack of time due to an overload of cases, a lack of incentives for FI sessions, and a lack of cohesiveness among different settings such as inpatient and outpatient settings.22, 23, 26
Related to Characteristics of the Patient and Illness
Many studies have indicated that the symptoms of the illness, such as being hostile and aggressive towards family members, make it challenging for FI to receive treatment.21, 22, 25 Another study stated that patients are concerned about additionally burdening the family or not getting along with the family as a barrier for FI and about losing their social status within the family as a consequence of FI. 22 Additionally, professionals have reported that it often becomes difficult to convince or motivate the patient and family to FI. 22
Related to the External Environment
This category has two subdivisions: (i) practical/economic factors and (ii) sociocultural factors.
(i) Practical/Economic Factors: Many studies have reported that families could not engage in the treatment of patients due to the multiple roles they hold in the family, such as the work-commitment schedule and fulfiling social roles. It becomes difficult for the family when services that need their involvement are offered only during working hours. Likewise, family members become unable to spare time for their involvement due to other roles and responsibilities they hold within the family.22, 25, 26 Many studies reported that patient refusal or non-consent for family involvement was a major barrier, and their poor relationship with the family member also added to the barrier.21, 22, 24, 25 The non-availability of family members to receive services is another practical barrier to FI. Many families reported being involved in a patient’s treatment apart from the caregiving as an additional responsibility for them, hindering them from FI. 22 Moreover, logistical factors such as the location of service centers, transportation, the family’s lack of resources (e.g., money), and continuity of personnel affected FI. 22
(ii) Sociocultural Factors: Families’ cultural beliefs about illness and cultural background have been considered barriers to family involvement in treatment.22, 26 Likewise, many studies have indicated various forms of stigma held by patients, family members, or the community regarding the illness or family involvement, fear of being identified by others as using psychiatric facilities or having a family member with mental illness, and anticipated rejection by others, all of which hinder the process of FI/FR.22, 23, 25, 26 One review reported the language background of caregivers not matching that of the service provider and the technical language used by professionals as a barrier for FI/FR. 22
Discussion
Our scoping review identified six studies addressing the factors associated with family involvement or retention in the treatment of PwSMI. Even though we did not have any time specificity for inclusion, we got studies published from 2003 to 2020. Our review indicates the dearth of research in this area. To our knowledge, this is the first scoping review to reflect on what is known about the factors of FR/FI in the treatment of PwSMI. Overall, only two studies in the present review were exclusively focused on schizophrenia. The rest of the studies included schizophrenia along with other severe mental illnesses. Two out of six studies were secondary studies, and the remaining four were primary studies, all of which adapted qualitative methods. All the primary studies included were from European countries, and most are from the United States and the United Kingdom. Caregivers were the major participants in the studies.
Review findings suggest that most studies have described barriers for FI, while only a few have elaborated on facilitators for FR/FI. Our review indicated the mental health system and family- level factors as the main contributors to the barrier to family involvement or retention in the treatment of PwSMI. The most common factors described as barriers in the majority of the studies were non-acknowledgment and recognition of the caregiver in mental health settings, the complexity involved in maintaining confidentiality and autonomy of the client, a lack of competence among clinicians for FI, a lack of resources for FI with both caregivers and organizations, non-recognition of the benefits of FI, and the practical barriers for FI/FR.
The definition of family involvement or family retention in treatment remained complex, as in our review. Two intervention-focused studies described it as a minimum of 12 months of a family’s continued participation in the intervention;23, 25 however, they did not specifically define family involvement. In the rest of the non-intervention-focused studies, the definition of FI/FR varied, where some defined it as an activity that required collaboration between multiple stakeholders in mental healthcare, 26 some considered it the basic level of functional intervention such as information provision and assessment, some also included more complex specialized intervention such as family therapy 22 and some did not give a clear definition at all.21, 24
Family involvement is essential and crucial in mental healthcare and treat- ment. It can reduce treatment costs and readmissions and improve the prognosis. Mental Health Care Act (MHCA) 2017 also emphasizes the empowerment of the patient and caregiver so they can manage symptoms by themselves. 27 MHCA 2017 mandates the rights of persons with mental illness, according to which the patients can choose their course of treatment. While the patient is severely ill and not in a state to understand, the family members’ role as nominative representatives becomes very important. As a nominative representative, the family member’s presence and support throughout the admission to the mental healthcare service are paramount.
In general, the nature of FI/FR in mental healthcare calls for a multidiscipli- nary team (psychiatrist, clinical psychologist, psychiatric social worker, psychiatric nurse, etc.)28, 29 approach. At the same time, our review revealed the inter-professional struggle and the power struggle between family members and professionals,21, 22, 26 which indicates that better collaboration among these stakeholders is a must for realizing the benefits of FI/FR as prescribed in guidelines. 30 This review also revealed that the most frequent barriers for FI/FR are the acknowledgment of family members and the competence of professionals, for which we recommend instilling a supportive approach that keeps family members as prominent stakeholders in routine mental healthcare practice through training that includes the most recent research evidence related to this field.
Limitation
One of the limitations of this scoping review is that we did not formulate the definition of family retention or family involvement strictly, the reason being to widen the scope of this specialized area. Even though we targeted the population with schizophrenia, given the paucity of research in this area, we included studies on other severe mental illnesses as well. The studies included in the review were from 2003 to 2020, covering almost two decades; hence, there might be some variability among the factors synthesized in this review. The literature search was restricted to English-language articles whose full text was accessible. A single author screened the title and abstract. Finally, due to resource restrictions, we could not accommodate unpublished articles.
Conclusion
Without an in-depth understanding of the factors pertaining to this specialized field of FI/FR, it will be futile to develop and implement any intervention for PwSMI and their families in FI/FR. This scoping review, with its scientific rigor, brought out specific factors associated with FR/FI in the treatment of PwSMI, such as (i) family-level factors, (ii) professional-level factors, (iii) mental health system-level factors, (iv) related to characteristics of the patient and illness, and (v) external environmental-related factors. However, further research is clearly needed to bridge the gap in the available literature in this field. The current knowledge is insufficient to design holistic interventions encompassing the multidimensional field of FI/FR in treating PwSMI.
Supplemental Material
The Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.