
Abstract
The lower the dose, the ‘safer’ you are… but is that really the case in an emergency? The inferred (non-discernible) risks from radiation for low doses (below 100–200 mSv) are applied rigorously for emergency planning. However, the observable risks associated with protective actions, e.g. evacuation, have not yet been fully evaluated. Experience from the Fukushima Daiichi accident and hurricanes in the USA indicates there will be an observable increase in mortality associated with evacuating and dislocations particularly for residents of facilities for long stays and the elderly. In addition, mental health effects have been possibly the most severe health effects associated with past major nuclear power plant emergencies. A tool is needed to evaluate protective actions to ensure they are justified considering both the health risks of radiation exposure and protective actions. An analysis was performed of mortality and mental health effects associated with protective actions compared with the inferred radiation-induced deaths averted by protective actions. The results were presented in terms of absolute risk (cases per 1000) of health effects, which is an understandable way to compare and communicate risks. The analysis indicates that taking protective actions consistent with dose criteria typically used in many countries could result in observable deaths when trying to prevent the inferred (non-discernible) radiation-induced deaths. Residents of facilities for long stays and the elderly are particularly vulnerable.
INTRODUCTION
The lower the dose, the ‘safer’ you are… but is that really the case in a nuclear or radiological emergency? The health risks from radiation have been inferred (non-discernible) for low doses (below 100–200 mSv) and applied rigorously for emergency planning. Importantly, cancer deaths at doses below about 100 mSv effective dose are not consistently discernible, even after careful study of many thousands of exposed individuals over their lifetimes (ICRP, 2007). However, the observable health risks associated with protective actions, e.g. evacuation, and mental health effects have not been considered. So how can we be sure we’re doing more good than harm when recommending the public to evacuate? Experience from the Fukushima Daiichi nuclear power plant (NPP) accident and evacuations for hurricanes in the USA show a significant risk associated with evacuating and dislocations particularly for the elderly and patients in long-term care (Dosa et al., 2012; Tanigawa et al., 2012; Hasegawa et al., 2015, 2016). How can we quantify this risk and compare it with the radiation risk? A tool needs to be developed that allows evaluation of protective actions to ensure they are justified. Key stakeholders (e.g. local officials and the public) who may make or respond to decisions on protective actions need to use such a tool (ICRP, 2020), but this is only possible if the risks are presented understandably. This article provides such a tool.
2. BACKGROUND INFORMATION
There are two types of radiation-induced health effects—deterministic effects (also known as harmful tissue reactions) and late effects (also called stochastic (cancer and heritable effects)). The precautionary protective action strategy to avoid deterministic effects is typically based on conditions at the NPP, not on dose criteria. For stochastic effects, the risk of fatal radiation-induced cancer deaths is inferred using the linear non-threshold (LNT) model and the ICRP fatal radiation risk coefficient of 5% (50 deaths per 1000 exposed) per Sv effective dose (ICRP, 2007). This is typically used as a basis for the development of protective action strategies, particularly for lower dose situations after protective actions have been implemented. Predetermined projected effective dose (mSv) criteria to reduce stochastic effects are typically below levels at which deaths are discernible, and thus the risk is inferred. No consideration is given to the observable harmful effects associated with protective actions. Thus, protective action strategies using such criteria are biased in favour of protecting people from inferred radiation-induced health effects (not discernible)—the lower the dose, the better.
The experience from the Fukushima Daiichi NPP accident indicates that protective actions did more harm than good. There was no system for evaluating whether the protective actions were justified. For example, relocation was implemented based on a 20-mSv dose (the lowest value in the range of the ICRP reference level where consideration should be given to reducing doses for emergency exposure situations) (ICRP, 2007), even though no discernible radiation-induced health effects are expected at 20 mSv. However, after evacuation and dislocation due to protective actions (e.g. relocation,) there were observable deaths (Nomura et al., 2013; Yasumura, 2014; Morita et al., 2017; Reconstruction Agency Japan, 2019), increases in morbidity (e.g. diabetes, heart diseases, and mental health problems) (Satoh et al., 2015; Suzuki et al., 2015; Fukushima Medical University, 2018; Nomura et al., 2021), and other severe effects (e.g. economic) (Cabinet Office Japan, 2012) associated with the protective actions.
Furthermore, the biggest impact of the Fukushima Daiichi accident was mental health problems (e.g. depression, anxiety disorders, PTSD, and medically unexplained physical symptoms) (Maeda et al., 2014; Yabe et al., 2014). These effects were associated with perceptions of radiation health risks.
There are two ICRP publications (ICRP, 2007, 2020) that describe the principle of justification for an emergency exposure situation. The principle of justification is defined in ICRP Publication 103 as: ‘Any decision altering a radiation exposure situation should do more good than harm’ (ICRP, 2007). The Commission considers that a dose rising towards 100 mSv will almost always justify protective actions (ICRP, 2007). ICRP Publication 103 also states that in a major emergency, an assessment based on health effects would be insufficient and due considerations must be given to societal, economic, and other consequences (ICRP, 2007). Furthermore, ICRP Publication 146 describes that justification should take careful account of all non-radiological factors in order to preserve or restore the living and working conditions of all those affected (ICRP, 2020). But neither of these publications describes how this should be done.
ICRP Publication 146 states that key stakeholders (e.g. regulators, local officials, and the public) who may make or respond to such decisions on justifying protective actions need to be involved as they will be the ones who apply justification in their emergency preparedness arrangements (ICRP, 2020). However, it is only possible to take into account the risks of radiation exposure and protective actions if they are presented in an understandable way.
The aim of the authors is to provide a tool to allow key stakeholders to make justified decisions during planning and response considering the impact of both radiation and protective actions.
3. STUDY METHODS
An analysis was performed focusing on observed mortality and mental health problems associated with protective actions compared with inferred radiation-induced deaths averted by protective actions. Over 50 articles were selected as useful from more than 600 reviewed articles to characterise the health impact of protective actions taken during different emergencies (natural and man-made disasters). Mental health problems associated with protective actions and perception of radiation risk were also considered in the analysis, since these are possibly some of the most severe health consequences of past NPP emergencies.
A tool was developed to support the comparison of the absolute risk of radiation-induced deaths with deaths associated with protective actions, dislocations, and mental health problems. The tool can be used now but with caution owing to the variation and uncertainty in estimating such risks (e.g. risks can be age and sex dependent). The tool was developed for ease of use and to meet the need for a tool that can be available now to evaluate the risk of protective actions versus the radiation-induced death risks. It was developed based on the best available data and formulated such that it can be easily used as a basis for making informed decisions on NPP emergency preparedness arrangements.
4. RESULTS
The tool is presented in Table 1 (Callen-Kovtunova et al., 2022). The radiation-induced deaths possibly prevented by protective actions are inferred using the LNT model for the range of doses typically used for protective action criteria. The absolute risk of deaths associated with protective actions or dislocations is in the order of 3/1000 among the general population, 17/1000 among residents of facilities for long stays and the elderly when needed support (e.g. medical supplies) is provided, and 60/1000 when needed support was not provided. The absolute risk of mental health problems (probable PTSD) associated with dislocations and perceived risk of exposure to ionising radiation was 200/1000 among the general population and 120/1000 for psychological distress among children.
Dose criteria for triggering protective actions (mSv), absolute risk (per 1000) for inferred radiation-induced deaths prevented by triggered protective actions, observable deaths associated with protective actions or dislocations, and mental health problems associated with dislocations and perceived risk of exposure to ionising radiation (Callen-Kovtunova et al., 2022).
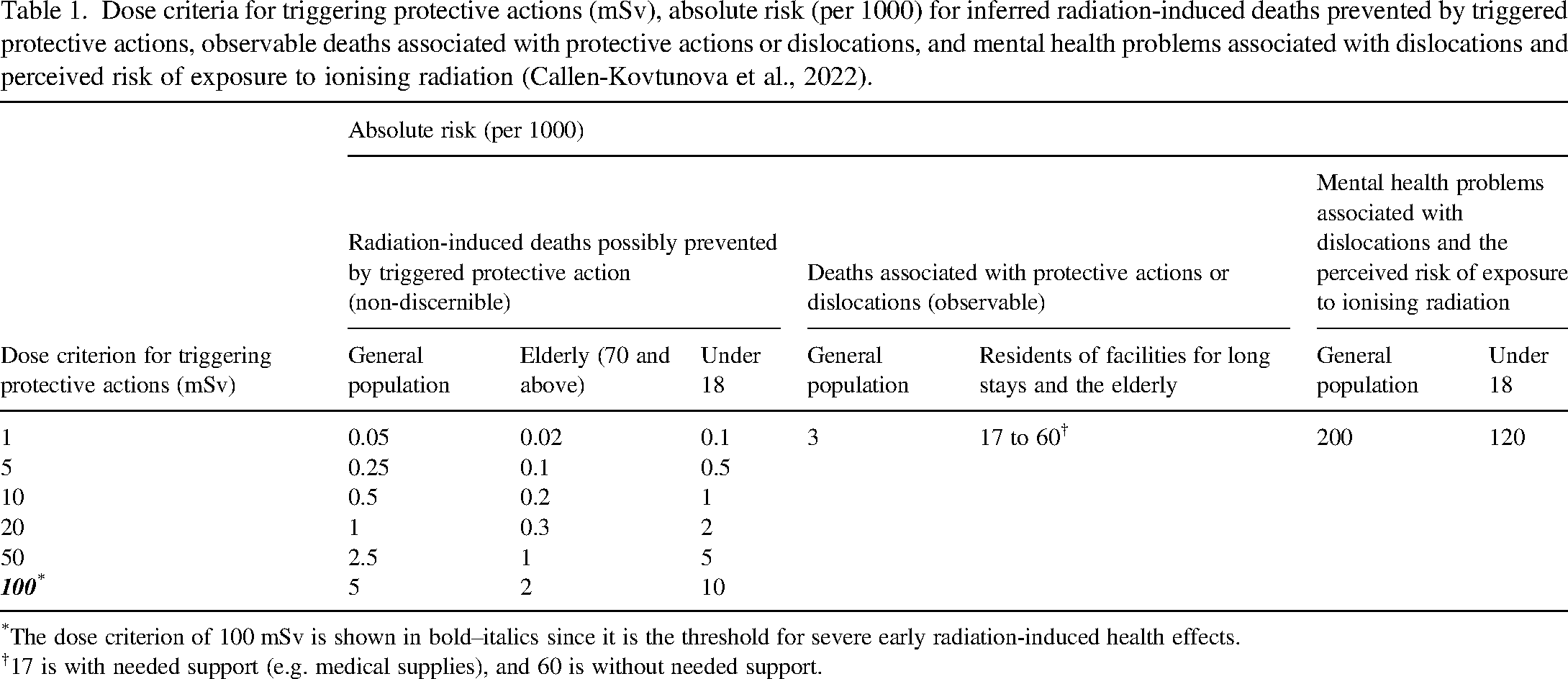
The dose criterion of 100 mSv is shown in bold–italics since it is the threshold for severe early radiation-induced health effects.
17 is with needed support (e.g. medical supplies), and 60 is without needed support.
An example of applying Table 1: taking protective actions at 20 mSv (e.g. relocation) may cause about 60 times (i.e. 17/0.3) more deaths among the elderly (aged 70 and above) who are residents of facilities for long stays, than the radiation-induced deaths possibly prevented by the relocation (and would also be non-discernible).
When estimating the 3/1000 risk of death for the general population, the authors found that ≈60% were due to causes that could possibly be alleviated by prior emergency preparedness provisions (Reconstruction Agency Japan, 2012). The estimate of three early deaths per 1000 of the general population was based on deaths recorded within 6 months after the accident. The 60/1000 deaths among residents of facilities for long stays and the elderly are associated with evacuation. They occurred during or shortly after transportation when needed support was not provided. Most of the excess deaths and mental health problems associated with protective actions would be clearly observable within months to a year.
This study only considered deaths and mental health problems for NPP emergencies. There are many other adverse effects observed after the Fukushima Daiichi and Chernobyl NPP accidents, including increases in morbidity—e.g. diabetes, hypertension, heart disease, disruption of social support networks, increases in domestic abuse, memory problems in children, and economic effects.
5. POSSIBLE FURTHER DEVELOPMENTS
A tool is also needed for radiological emergencies, including transport, orphan sources, sources used in industry, medicine and research, and malicious acts (e.g. radiation dispersal device and dirty bomb), as well as considering other scenarios, such as:
Food/product contamination (including ingestion of traditional food) Potentially contaminated people (failure to treat/transport) Perceived risks—misinformation Concurrent emergencies (with technical, natural, or other)—all hazards approach
The full range of adverse effects for important radiation pathways and an in-depth examination of the health effects from protective actions should be considered in future studies.
Furthermore, other human health impacts should be considered, including radiological and non-radiological (mortality, morbidity), as well as impacts on well-being. Both environmental and economic impacts should also be considered. When justifying protective action strategy decisions, early protective action strategies, such as evacuation, may consider only human health impacts. Whereas longer-term protective action strategies, such as relocation and return therefrom, should also consider environmental and economic impacts (e.g. involving decontamination and waste issues).
A comprehensive system for taking justified protective actions is needed, justified dose criteria, justified operational criteria, and justified information for decision makers and the public.
6. CONCLUSIONS
The analysis indicates that taking protective actions consistent with dose criteria typically used in many countries could result in more excess deaths than inferred radiation-induced deaths prevented, as well as resulting in mental health problems. Residents of facilities for long stays and the elderly are particularly vulnerable. This analysis provides a first step for developing tools for NPP and other emergencies to evaluate the risk of protective actions versus radiation-induced health risk. It is not comprehensive and does not cover other radiological emergencies or adverse consequences (e.g. increased morbidity rates and vast economic impact) which also affect people's lives. This tool could be expanded to consider other scenarios (e.g. malicious events and lost radioactive sources), morbidity risks, justifying protective actions during concurrent emergencies, and what expertise should be consulted with in developing such tools.