
Abstract
Advanced imaging technology has opened new horizons for medical diagnostics and improved patient care. However, many procedures are unjustified and do not provide a net benefit. An area of particular concern is the unnecessary use of radiation when clinical evaluation or other imaging modalities could provide an accurate diagnosis. Referral criteria for medical imaging are consensus statements based on the best-available evidence to assist the decision-making process when choosing the best imaging procedure for a given patient. Although they are advisory rather than compulsory, physicians should have good reasons for deviation from these criteria. Voluntary use of referral criteria has shown limited success compared with integration into clinical decision support systems. These systems support good medical practice, can improve health service delivery, and foster safer, more efficient, fair, cost-effective care, thus contributing to the strengthening of health systems. Justification of procedures and optimisation of protection, the two pillars of radiological protection in health care, are implicit in the notion of good medical practice. However, some health professionals are not familiar with these principles, and have low awareness of radiological protection aspects of justification. A stronger collaboration between radiation protection and healthcare communities could contribute to improve the radiation protection culture in medical practice.
1. INTRODUCTION
The system of radiological protection aims to control radiation risks to provide an adequate level of protection without unduly limiting the potential benefits for individuals and society. Achieving this balance in medical exposures is particularly challenging. The use of ionising radiation for diagnosis and treatment of human diseases has increased worldwide (UNSCEAR, 2010). Benefits have gained recognition, and advanced imaging technology has opened new horizons to medical diagnostics and improved patient care. While modern technology improves the safety of new applications, inappropriate or incorrect use can lead to unnecessary or unintentional radiation exposures with associated radiation risks for patients and staff. As such, there is a need for public health policies that recognise the multiple health benefits that can be obtained, while addressing and minimising health risks.
It has been reported that a substantial proportion of medical imaging procedures (>20% in some areas) may be inappropriate (Malone et al., 2012). An area of particular concern is the unnecessary use of ionising radiation when clinical evaluation or other imaging modalities could provide an accurate diagnosis (justification of procedures). In addition to the scientific evidence, justification of an examination must rely on professional evaluation of comprehensive patient information, such as relevant clinical history, prior imaging, laboratory tests and treatment. Once the procedure has been justified, methods for dose reduction should be applied to manage the radiation dose commensurate with the medical purpose (optimisation of protection). Radiation protection in medicine is built on these two principles: justification and optimisation. However, some health professionals are not familiar with these principles and have a low level of awareness of radiation doses and potential risks (Shiralkar et al., 2003; Lee et al., 2004; Carpeggiani et al., 2012). There is a need to establish a radiation protection culture in medical practice in order to ensure that patients benefit from the medical use of radiation, and allowing more cost-effective allocation of health resources. This paper addresses the radiological protection aspects of justification of medical imaging, and discusses the concept of referral criteria and decision support systems, and their potential role to improve justification of medical imaging procedures.
2. JUSTIFICATION OF MEDICAL EXPOSURES IN THE CURRENT SYSTEM OF RADIOLOGICAL PROTECTION
In Publication 103, the International Commission on Radiological Protection (ICRP) proposed a system of radiological protection based on the characteristics of the radiation exposure situations (planned, existing, or emergency exposure situations) and the categories of exposure (occupational, medical, or public exposure) (ICRP, 2007a). The principles of justification and optimisation apply universally to all three exposure situations and categories of exposure. In this context, the principle of justification implies that any decision that alters the radiation exposure situation should do more good than harm; in other words, the benefits to individuals and society of introducing or continuing the activity should outweigh the harm (including radiation detriment) resulting from the activity. ICRP recognises that radiological protection in medicine requires an approach different from that applied in other exposure situations. One major difference is that radiation exposure in medicine is intentional and for the direct benefit of the patient.
1
Neither dose limits nor dose constraints are therefore recommended for patients, because they might reduce the effectiveness of the procedure, thus doing more harm than good. The emphasis is on justification of the procedure and optimisation of the protection, noting that medical exposure of patients calls for a different and more detailed approach to the process of justification than any other category of exposure. In this case, justification often lies with health professionals rather than the government or the competent regulatory authority. The responsibility for justification of a particular procedure falls on the relevant medical practitioners, who need to have special training in radiological protection (ICRP, 2007a). The ICRP recommendations for radiological protection and safety in medicine are given in Publication 105 (ICRP, 2007b), which explains that the principle of justification applies at three levels in medicine as described below.
Level 1: the proper use of radiation in medicine is accepted as doing more good than harm to society. Level 2: a specified procedure is justified for a group of patients showing relevant symptoms, or for a group of individuals at risk for a clinical condition that can be detected and treated. Level 3: the application of a specified procedure to an individual patient is justified if that particular application is judged to do more good than harm to the individual patient.
3. JUSTIFICATION OF MEDICAL EXPOSURES IN THE INTERNATIONAL RADIATION SAFETY STANDARDS
Co-sponsored by eight international organisations, 2 the International Basic Safety Standards (BSS) for Protection against Ionising Radiation and for the Safety of Radiation Sources (IAEA, 2014) provide the leading international benchmark for safety standard setting, policy making and decision making. The International BSS establish specific responsibilities for health professionals related to radiation protection and safety in medical exposures. The introductory chapter notes that application of the principle of justification to medical exposures requires a special approach. In addition to general justification of the use of ionising radiation in medicine (Level 1), there is a need for generic justification of a given radiological procedure that applies to the justification of new technologies and techniques as they evolve (Level 2). Finally, justification of a radiological procedure for a given individual (Level 3) includes consideration of the purpose of the exposure, the clinical circumstances, and the characteristics of the individual involved. Referral criteria developed by professional bodies and health authorities have to be taken into account. These introductory concepts are further developed in Chapter 3 of the International BSS, which is devoted to planned exposure situations. The government or the regulatory body, as appropriate, should ensure that provision is made for the justification of any type of practice and for review of the justification, as necessary, and should ensure that only justified practices are authorised. It is emphasised that medical exposures should be justified by weighing the expected diagnostic or therapeutic benefits against the potential radiation detriment, with the benefits and the risks of available alternative techniques that do not involve exposure to radiation taken into account. While the responsibility for generic justification is assigned to the health authority in conjunction with appropriate professional bodies, the individual justification should be performed through consultation between the radiological medical practitioner and the referring medical practitioner, as appropriate, with consideration of appropriateness, urgency, type of exposure, patient conditions, and relevant previous information, with relevant referral guidelines taken into account. Justification of radiological procedures in asymptomatic populations as part of a health screening programme should be undertaken by the health authority in conjunction with appropriate professional bodies. However, specific individual justification by the radiological medical practitioner and the referring medical practitioner is required if the procedure is to be performed on an asymptomatic individual for the early detection of disease, but not as part of an approved health screening programme. The individual should be informed of the expected benefits, risks, and limitations of the procedure. Special considerations regarding pregnancy and breast feeding are provided in the International BSS. Procedures should be in place for ascertaining the pregnancy status of a female patient of reproductive capacity before the performance of any radiological procedure that could result in a significant dose to the embryo or fetus, so that this information can be considered in the justification and optimisation processes. Justification of nuclear medicine procedures that could result in a significant dose to a breastfed infant is addressed explicitly. Specific requirements for justification of exposure of volunteers as part of a programme of biomedical research are included in the International BSS. Critical review of implementation of the principle of justification should be part of radiological audits performed in medical radiation facilities.
Safety requirements concerning the justification of medical exposures represent a major component of the new European Commission Council Directive 2013/59/Euratom of December 2013 (EC, 2013), laying down the BSS for protection against the dangers arising from exposure to ionising radiation. Availability of clinical imaging guidelines is mandatory in the Euratom BSS, which are legally binding. In contrast, the International BSS are not legally binding; however, the implementation of their safety requirements, including those related to justification, can be subject to inspection by national regulatory bodies.
4. DOES THE INCREASE IN THE FREQUENCY OF RADIOLOGICAL IMAGING PROCEDURES IMPLY ‘OVERUSE’?
The increasing trend in the use of radiation in medical imaging cannot be taken per se as evidence of ‘overuse’. Considerable disparities exist between and within countries with respect to the use of radiation technologies (e.g. high-, medium-, and low-income countries; rural vs urban areas). While most developing countries still lack adequate capacity and resources to provide access to radiology services on a widespread basis, developed countries are increasingly facing the risk of overuse of computed tomography and other sophisticated technologies.
Health service delivery is one of the building blocks of health systems. Good health services deliver safe and effective health interventions to those that need them, when and where needed, with minimum waste of resources (WHO, 2007). In this context, the appropriate use of radiation in health care contributes to the strengthening of health systems.
The ultimate purpose of healthcare systems is to deliver the best care to every person, any time, and everywhere. Poor-quality care may come in the form of overuse (i.e. giving people care that they do not need), underuse (i.e. failing to give people the care that they need), and misuse (i.e. making errors that can damage people). All three problems should be addressed to improve the quality and safety of health care.
In medicine, the term ‘overuse’ refers to the application of a procedure where/when it is unlikely to improve patient outcome (i.e. unnecessary or unjustified). In this context, the ‘overuse’ of radiological medical procedures represents an issue that goes beyond the boundaries of radiation protection, and falls within the notion of good medical practice.
When choosing a procedure using ionising radiation, the benefit/risk balance must be considered carefully. Even if benefits outweigh risks, there is unnecessary use of radiation when clinical evaluation or other imaging modalities could provide an accurate diagnosis. Cost, local expertise, available resources, accessibility, and patient values have to be considered, as well as efficacy.
The benefit outweighs the risk when the procedure is prescribed appropriately and performed properly. This is not the case if there is no clinical indication or the radiation dose is higher than necessary for the clinical purpose (e.g. adult protocols used to image children). A medical imaging examination is useful if its outcome, either positive or negative, influences the management of the patient or strengthens confidence in the diagnosis. When indicated and available, imaging modalities that do not use ionising radiation (e.g. ultrasound or magnetic resonance imaging) are preferred, especially for children. The possibility of deferring imaging to a later time if/when the patient’s condition may change must also be considered. The final decision may also be influenced by cost, expertise, availability of resources, and/or patient values.
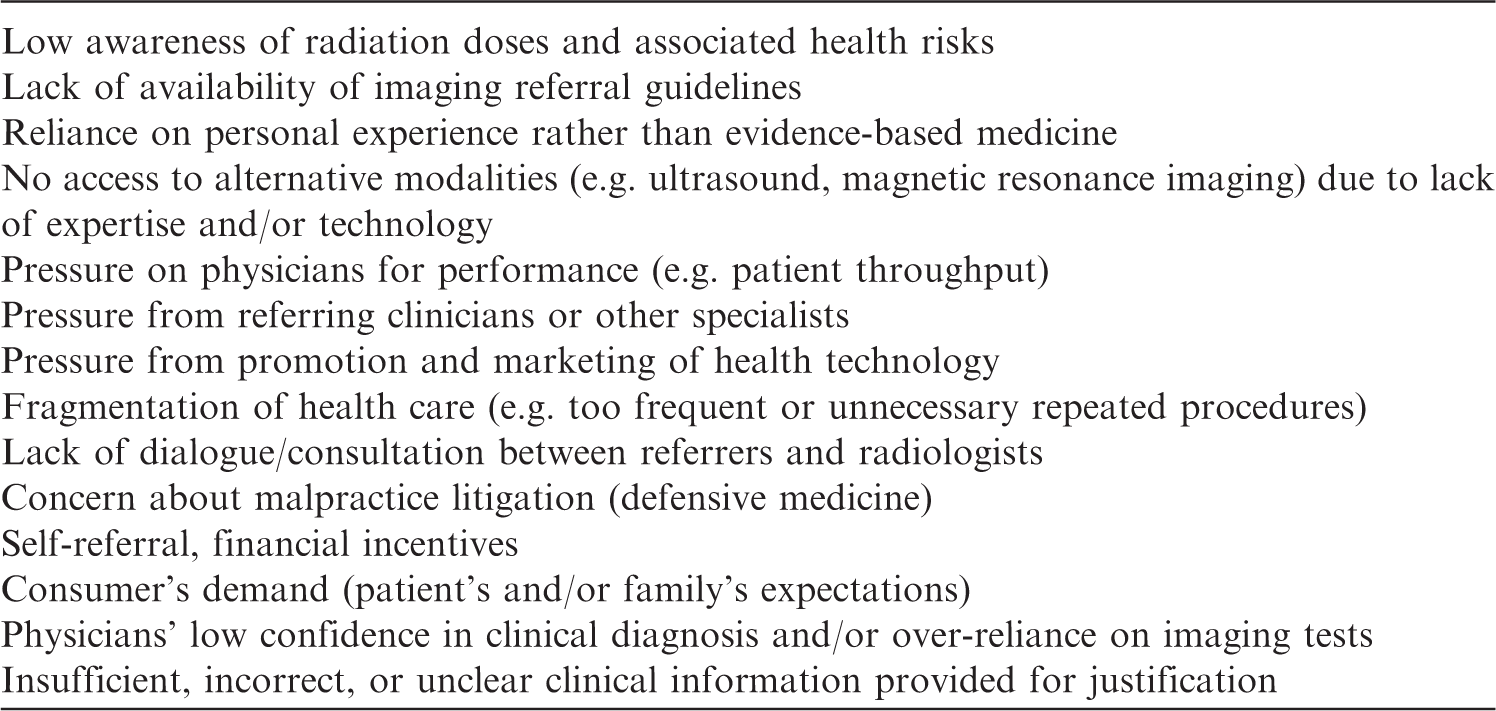
Possible referral incentives for radiological imaging procedures.
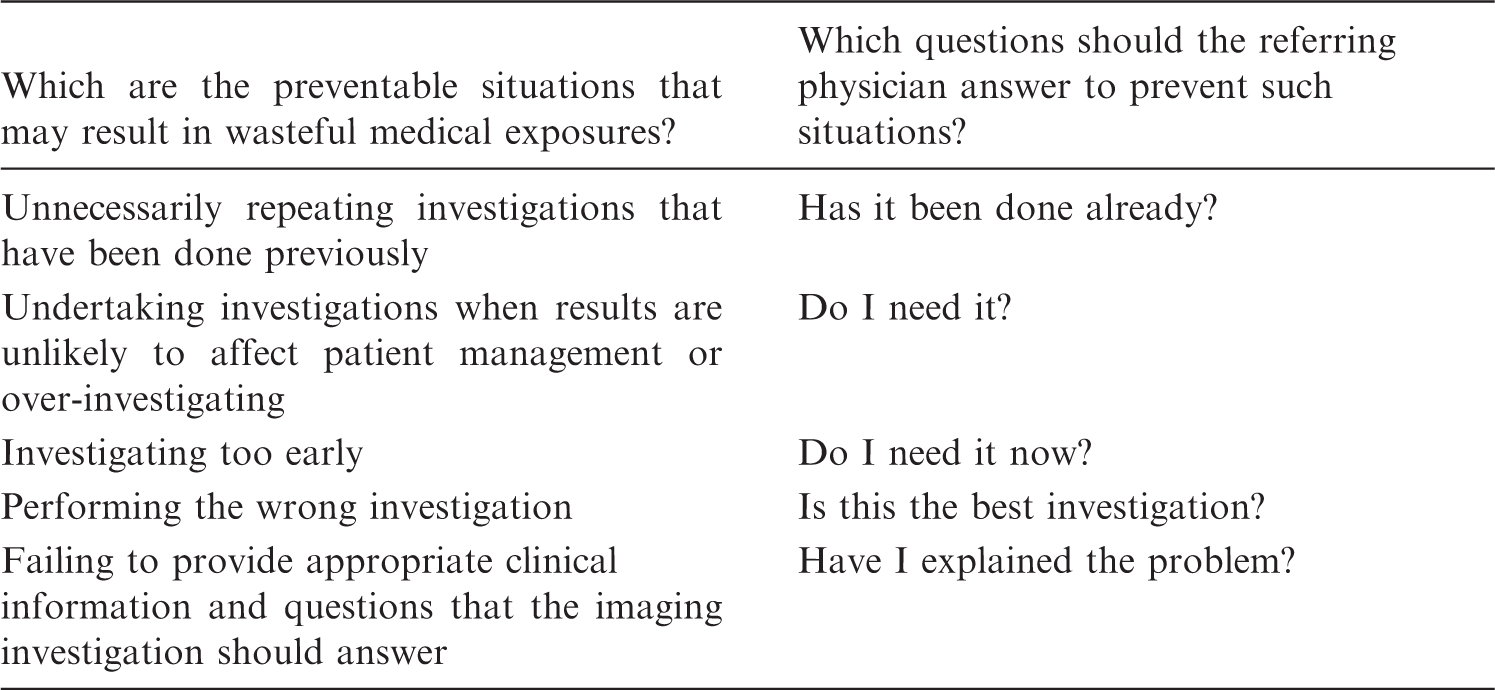
Examples of questions proposed for referring clinicians (adapted from RCR, 2013).
Depending on the national healthcare system, commercial interests may influence medical imaging referral as radiological examinations may be a source of income to radiology departments. Such a situation may create referrals that exceed the needs of good medical practice, confer unjustifiable risk on patients, and are inconsistent with principles of radiological protection and medical ethics (ICRP, 2007b).
In some countries, health professionals have concerns about possible malpractice litigation. Physicians may respond to this threat of litigation by ordering more referrals and more tests, some of which may be wasteful and even harmful. This so-called ‘defensive medicine’ often results in overuse of radiation for medical imaging, and this is particularly relevant in trauma centres and emergency departments (Hadley et al., 2006; Sierzenski et al., 2014). It has been demonstrated that such defensive behaviour can be modified towards evidence-based behaviour by training physicians in the use of referral guidelines (Rohacek et al., 2012).
5. REFERRAL CRITERIA FOR MEDICAL IMAGING
Faced with a clinical presentation, the referring physician makes a decision for an individual patient based on overall best practice (Level 3). However, complexities and rapid advances in medical imaging render it difficult for referrers to follow changes in evidence-based standards of care. Therefore, generic guidance for justification of imaging (Level 2) is usually provided by professional societies in conjunction with health authorities as referral criteria for medical imaging. These criteria are consensus statements based on the best-available evidence to assist the decision-making process when choosing the best imaging procedure for a given patient. Although these criteria are advisory rather than mandatory, physicians should have good reasons for deviation from these criteria.
Imaging referral guidelines provide physicians with information regarding which procedure is most likely to yield the most informative results, and whether another modality is equally or more effective, and therefore more appropriate. As decision-aiding tools for good medical practice, these guidelines can improve health service delivery. These guidelines support the practice of evidence-based medicine and form a foundation to guide appropriateness in prescribing diagnostic imaging services.
Examples of referral guidelines include the Appropriateness Criteria of the American College of Radiology (ACR, 2014), ‘iRefer: Making the Best Use of Clinical Radiology’ (RCR, 2013), ‘Diagnostic Imaging Pathways’ (Government of Western Australia, Department of Health, 2014), and ‘Guide de bon usage d’imagerie médicale’ (SFR/SFMN, 2013).
The use of imaging referral guidelines could reduce the number of unjustified examinations (RCR, 1993; Oakeshott et al., 1994; Hadley et al., 2006). It was recently demonstrated by clinical audit that, even when awareness of the availability of referral guidelines is relatively low, scrutinizing based on imaging referral guidelines and amending or returning those found inappropriate enables a high level of appropriate imaging (95%), thus making the best use of clinical radiology (Remedios et al., 2014).
Evidence-based imaging referral guidelines have gained widespread global acceptance, and many countries are now considering the adoption or adaptation of one of the existing evidence-based referral guidelines. Given the frequency of similar pathologies, it is not surprising to find comparable guidelines in different regions of the world. Despite various formats (e.g. tabulated vs flow charts) and media (e.g. hard copy, electronic copy, interactive web-based, smart phone-based, etc.), the common philosophy behind the use of these guidelines is to promote a questioning attitude among physicians before making decisions about medical imaging. An example of this approach is the Socratic questions 3 proposed in iRefer, summarised in Table 2.
6. DECISION SUPPORT SYSTEMS
Voluntary use of referral criteria has shown limited success compared with integration into clinical decision support (CDS) systems. These systems support good medical practice, can improve health service delivery, and foster safer, more efficient, fair, cost-effective care, thus contributing to the strengthening of health systems. The importance of having such systems in place to assist referring physicians in making the best decisions has been acknowledged over the past few years (Health Council of Canada, 2010).
Formerly called ‘computerised physician order 4 entry’ systems, these CDS systems facilitate the integration of imaging referral guidelines into the daily workflow, with provision of interactive reminders. Such CDS systems should be available at the point of care, implemented through clinical workflow, and preferably executed in real time. At the time of entry into the CDS system, the referring doctors receive feedback on the degree of appropriateness of their choices relative to the referral guidelines (e.g. warnings and coloured codes) (Kawamoto et al., 2005).
The integration of CDS into radiology requesting systems embedded in patient care pathways has proven to slow down the increasing use of computed tomography, to be acceptable to clinicians and to improve appropriateness of imaging referral, particularly in the emergency department (Sistrom et al., 2009; Ip et al., 2012).
Potential caveats related to the use of CDS systems include technical challenges of connectivity and interfacing with existing clinical information systems, inability to cover all possible clinical presentations, limited applicability of their guidance to individual patients, and possibility of bypassing ‘soft stops’ in the system. Nevertheless, it can be concluded that CDS systems are useful tools to facilitate implementation of evidence-based imaging referral guidelines at the time of referral.
7. DISCUSSION
The principle of appropriateness in imaging can be encapsulated into three words: ‘best test first’. A number of international, regional, and national initiatives are being conducted to increase appropriateness, reduce unnecessary radiation exposures, and thus prevent unnecessary radiation risks.
ICRP currently has a Working Party on Justification of Medical Imaging composed of members of ICRP Committee 3 on Protection in Medicine as well as external experts. In the framework of its Global Initiative on Radiation Safety in Health Care Settings, the World Health Organization (WHO) promotes availability and use of imaging referral guidelines at a global level, and is currently conducting a project on justification of medical imaging of asymptomatic people for individual health assessment (Lau et al., 2011a,b). In the framework of its International Action Plan for Radiological Protection of Patients, the International Atomic Energy Agency (IAEA) launched a ‘3-A’s campaign’ promoting the concept of awareness, appropriateness, and audit to improve justification (Malone et al., 2012). The European Commission, its Working Party on Medical Exposures of Article 31 of the Euratom Treaty, 5 and the association of Heads of European Radiological Protection Competent Authorities 6 complement each other’s efforts to foster appropriateness and enhance justification in Europe. Large-scale campaigns are being pursued intensively by professional societies (e.g. Image Gently, Image Wisely, Eurosafe 7 ). National initiatives on this topic are numerous.
An international conference on radiation protection in medicine was organised by IAEA in cooperation with WHO in December 2012, hosted in Bonn by the Government of Germany. More than 500 participants from approximately 80 countries and 16 organisations reviewed advances, challenges, and opportunities. The main outcome of this conference was a list of 10 priority actions to improve radiation safety in health care in the next decade.
8
The first priority action of the so-called ‘Bonn Call for Action’ refers to enhancing implementation of justification by:
introducing and applying awareness, appropriateness, and audit to facilitate and enhance justification in practice; developing harmonised evidence-based criteria to strengthen the appropriateness of clinical imaging, including diagnostic nuclear medicine and non-ionising radiation procedures, and involving all stakeholders in this development; implementing clinical imaging referral guidelines globally, keeping local and regional variations in mind, and ensuring regular updating, sustainability, and availability of these guidelines; strengthening the application of clinical audit in relation to justification, and ensuring that justification becomes an effective, transparent, and accountable part of normal radiological practice; introducing information technology solutions, such as decision support tools, in clinical imaging, and ensuring that these are available and freely accessible at the point-of-care; and further developing criteria for justification of health screening programmes for asymptomatic populations (e.g. mammography screening), and for medical imaging of asymptomatic individuals who are not participating in approved health screening programmes.
Justification of procedures and optimisation of protection, the two pillars of radiological protection in health care, are implicit in the notion of good medical practice. However, some health professionals are not familiar with these principles, and have low awareness of radiological protection aspects of justification.
Global partnerships should be expanded, and stronger collaboration between radiation protection and healthcare communities should be fostered to improve radiation protection culture in the medical sector. The most effective means to decrease radiation dose associated with medical imaging without compromising the benefits is to eliminate unnecessary or inappropriate referrals. Application of the principle of justification is therefore a key measure to control unnecessary radiation exposures in health care.
Footnotes
1
Although risks and benefits associated with a medical procedure usually accrue to the same person, there may be other considerations such as occupational exposure of health workers, and screening programmes that may benefit the population rather than every screened individual.
2
European Commission, Food and Agriculture Organization, International Atomic Energy Agency, International Labour Organization, Organization for Economic Co-operation and Development/Nuclear Energy Agency, Pan American Health Organization, United Nations Environment Programme, and World Health Organization.
4
The term ‘order’ is not appropriate because it gives the false impression that referring physicians are entering ‘orders’ while, in fact, they are entering ‘requests’ for advice from the imaging specialists. As such, the abbreviation ‘CPOE’ is not recommended.