
Abstract
We present a case of an encephalocele of the lateral recess of the sphenoid sinus and detail the utilization of a nerve-sparing, windowed, pterygopalatine fossa approach to the lateral sphenoid sinus recess in a 37 year-old patient. The patient presented with 15 years of headaches that worsened with stress and head position and 2 weeks onset of unilateral clear rhinorrhea that was similarly worsened by head position. Collected rhinorrhea was positive for β-2 transferrin, and computed tomography was notable for erosion of the roof of the sphenoid sinus at the lateral recess with soft tissue extending into the sphenoid sinus. Magnetic resonance imaging confirmed the presence of a sphenoid encephalocele. The patient underwent a nerve-sparing windowed transpterygoid approach to the skull-base defect. Intraoperatively, 2 discreet skull-base defects were encountered, each with exposed dural tissue that were then repaired with septal cartilage underlay grafts and overlay mucosal grafts. The patient started acetazolamide in the postoperative period and recovered without the recurrence of cerebrospinal fluid leak.
Introduction
Spontaneous cerebrospinal fluid (CSF) leaks are rare, with a reported incidence of 1 in 35,000 of all causes. 1 Increased intracranial pressure from idiopathic intracranial hypertension (IIH) remains a common cause of IIH with an estimated incidence of 0.9 per 100,000 person, increasing to 19 per 100,000 when considering only middle-aged obese women. 2 A United States database review has noted that the rates of spontaneous CSF leak have over-doubled between 2002 and 2012, rising in line with populational obesity and noting an association where higher obesity regions may present with higher rates of spontaneous CSF leaks. 3 CSF leaks secondary to IIH commonly occur due to encephaloceles within the ethmoid skull-base or lateral sphenoid sinus recesses (LSSR), but can be due to defects at other locations, 4 and 16% to 31% of patients with IIH may present with multiple skull-base defects.5,6
Successful management of IIH-related CSF leaks requires the management of skull-base defects and reduction in the underlying intracranial hypertension. The management of intracranial hypertension is often through acetazolamide or CSF shunting procedures, although the evidence regarding the use of acetazolamide remains mixed. 7 The lateral sphenoid sinus recess develops via pneumatization of the sphenoid bone lateral to a line extending lateral to the Vidian canal to the foramen rotundum (V-R) that is posterior to the pterygopalatine fossa and within the pterygoid process. In the setting of IIH, up to 42% of CSF leaks may present within the LSSR, 6 making recognition and appropriate treatment of these lesions critically important to the skull-base surgeon.
The LSSR is challenging to access surgically, and more traditional open approaches have since been replaced by endoscopic approaches to the LSSR. This can be accomplished through extended sphenoidotomy 8 or transpterygoid approaches. 9 However, complications with LSSR approaches are relatively common, with 12% to 19% of patients reporting facial numbness and 10% to 18% reporting dry eyes.10,11 In this report, we will examine a male patient that presented with acute onset of CSF leak with multiple LSSR skull-base defects and highlight a nerve-sparing, windowed endoscopic approach to the LSSR for CSF leak repair.
Case Presentation
The patient is a 37 year-old male with no significant medical comorbidities and body mass index (BMI) of 39.6 at the time of presentation. The patient reported that he had been experiencing headaches for approximately 15 years of uncertain etiology. These headaches tended to worsen with straining, stress, and head position, particularly bending over. He was in his usual state of health until 2 weeks prior to presentation when he began to have right-sided clear rhinorrhea and postnasal drip that was clear, watery, and salty in taste. The patient saw an outside otolaryngologist who obtained β-2 transferrin testing which was positive, consistent with a CSF leak. A computed tomography (CT) sinus was obtained, which demonstrated bilaterally-well-pneumatized LSSR with 2 right-sided areas of skull base with soft tissue extending into the sphenoid sinus lateral to the foramen rotundum with associated air-fluid level within the sinus (Figure 1). An MRI brain with contrast was obtained, which confirmed the presence of LSSR encephalocele, although the resolution was not adequate to identify both encephaloceles, in the setting of a partially-empty sella and enlarged ventricles for patient age (Figure 2).
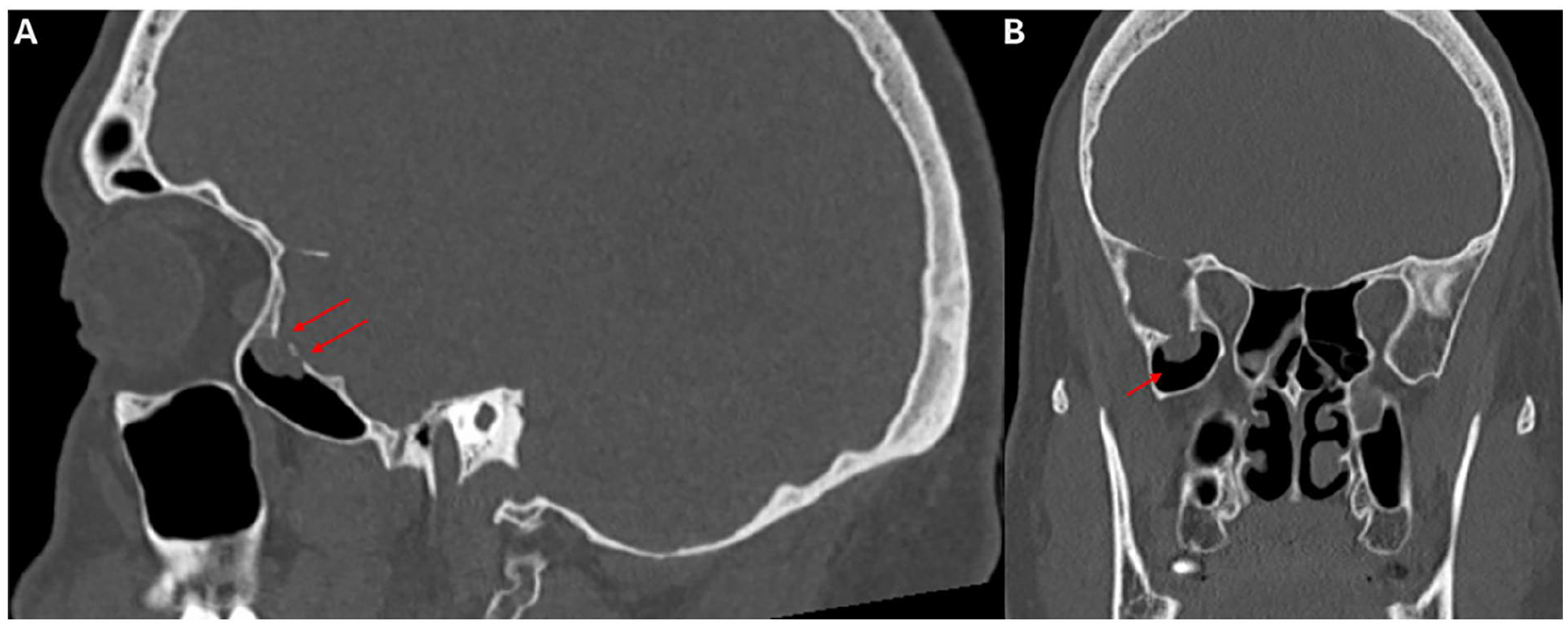
CT sinus in the sagittal (A) and coronal (B) planes. Note multiple areas of dehiscence as denoted by the red arrows in panel A within the lateral sphenoid sinus recess. CT, computed tomography.
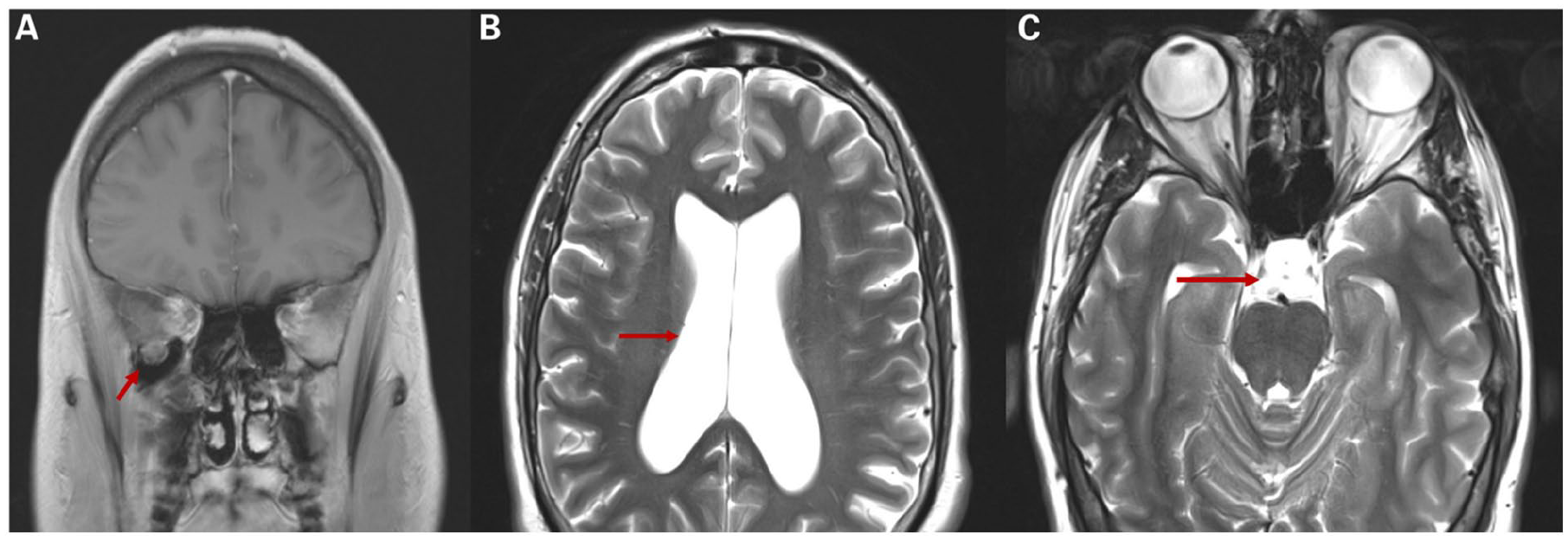
Magnetic resonance imaging obtained in the workup of lateral sphenoid sinus recess encephalocele. (A) depicts a coronal T1-weighted coronal image with the red arrow denoting apparent encephalocele. (B) and (C) are T2-weighted axial image with red arrow denoting ventricular dilation (B) and partially-empty sella tursica (C) that can be seen in idiopathic intracranial hypertension.
The patient elected to proceed with CSF leak repair via an endoscopic transpterygoid approach. The surgical approach was performed through an ipsilateral medial maxillectomy and sphenoethmoidectomy. A septoplasty was performed to improve endonasal access. To allow for improved lateral access, a Caldwell-Luc incision was performed and the face of the maxillary sinus entered. The pterygopalatine fossa was entered, and the sphenopalatine artery divided. The contents of the pterygopalatine fossa were retracted inferomedially, taking care to preserve the Vidian, infraorbital, and greater palatine nerves. The pterygoid muscle fibers were retracted, and the pterygoid plate exposed. The bone of the pterygoid plate was subsequently drilled, creating a window through which to visualize the LSSR. Within the LSSR, 2 separate encephaloceles were identified and ablated with bipolar cautery until they were flush with the skull base. Skull-base reconstruction was performed by placing an underlay septal cartilage graft in each defect followed by an overlay free mucosal graft, fibrin glue, and then densely packed absorbable packing (Figure 3).
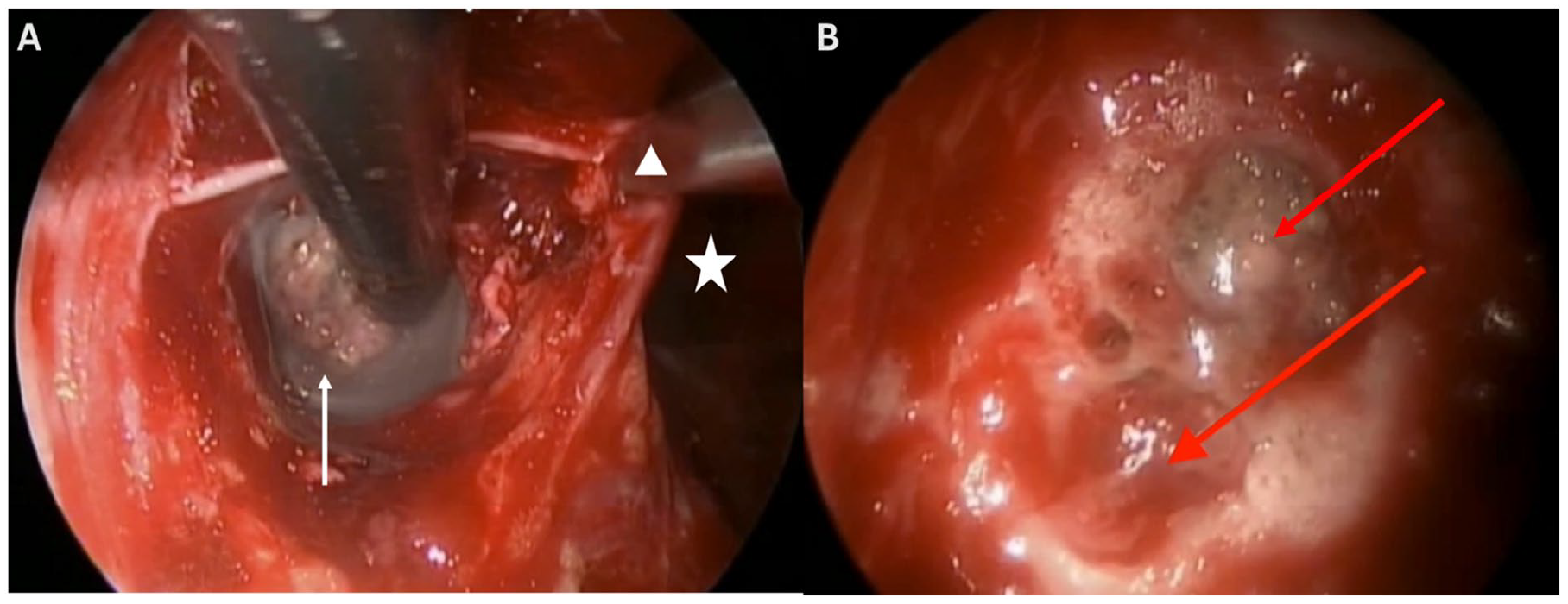
Endoscopic endonasal view of the windowed transpterygoid approach to the lateral sphenoid sinus recess. (A) demonstrates the presence of visible encephalocele (white arrow) through transpterygoid window. Note sphenoid sinusotomy (white star) and retraction of the sphenopalatine ganglion (white triangle) laterally to aid in access. (B) is an angled view through the transpterygoid window that looks upward and noted 2 separate skull-base defects (red arrows) with bridging bone.
The patient was admitted overnight and started on acetazolamide prior to subsequent discharge. At the follow-up, he denied facial numbness or dry eyes. The patient was unable to tolerate his acetazolamide and self-discontinued medication after a few months. Postoperatively, he was followed by ophthalmology and neurology to monitor his IIH. In his 6 years of follow-up, the patient lost over 60 lbs, reducing his BMI to 32.1 and has not had any recurrence of his CSF leak or any complications from his IIH.
Discussion
This patient was a male with likely long-standing IIH who eventually developed multiple spontaneous CSF leaks within the right LSSR. He was successfully managed with a combination of a nerve-sparing windowed transpterygoid approach to the lateral sphenoid sinus recess, initial medical therapy with acetazolamide, and sustained weight loss. This patient’s case highlights multiple important aspects of caring for patients with a spontaneous CSF leak in the setting of IIH, namely, to ensure careful evaluation for multiple skull-base defects and the ability to perform a nerve-sparing skull-base repair of the LSSR.
The presence of multiple skull-base defects in the setting of IIH has been documented in previous reviews and is a critically-important consideration in the evaluation and management of patients with IIH. Schlosser et al. published an early report of 5 patients presenting with multiple skull-base defects in the setting of IIH in 2002. They reported 4 patients with 2 encephaloceles and 1 patient with 3 encephaloceles, the most common presentation being bilateral LSSR encephaloceles (3 patients) with the remaining 2 patients presenting with combinations of frontal, ethmoid, and central sphenoid defects. 5 Woodworth et al. 6 examined a larger cohort of 48 patients and noted that 9 patients had multiple CSF leaks at the time of their initial surgery, although the exact location of these specific leaks were not specified. Patients in this cohort were followed for an average of 34 months, and during that time, there were 6 recurrent leaks noted, 3 of which were at sites distant from the initial CSF leak. Most (5/6) patients recurred within 3 months, but 1 patient had recurrence after 14 months with half having ventriculoperitoneal shunt failure and direct evidence of failure to reduce ICP. 6 These cases highlight the importance of careful endoscopic and imaging review in IIH patients to ensure secondary skull-base defects are not missed. Additionally, these studies emphasize the importance of postoperative care as there is a high risk of treatment failure, either at the primary repair site or at secondary skull-base defects with inadequate reductions in intracranial pressure. The principal management of IIH involves reducing intracranial pressure, weight loss, and monitoring for complications of intracranial hypertension to include visual changes and neurological sequelae. 12 Fortunately for our patient, he presented with 2 skull-base defects that were isolated to the same LSSR, and he was able to undergo successful repair with a single approach without recurrence of disease. Additionally, while our patient was unable to tolerate medical management of his IIH, he did have a substantial and sustained weight loss of over 60 lbs
Equally important to the management of patients with IIH is the selection of the appropriate surgical technique. In this patient, we utilized a nerve-sparing windowed technique through the pterygoid plate to visualize and reduce the encephalocele. A Caldwell-Luc was used for this specific case given difficulties in lateral visualization, but this is not routinely performed in our practice and the medial maxillectomy is typically adequate for complete exposure. The nerve-sparing windowed approach allows for direct visualization of the encephalocele without the need to ligate the Vidian nerve or retract significantly on V2 or the greater palatine nerve, preserving lacrimation and facial sensation, respectively. In 2024, Tosi et al. 11 proposed a classification system for categorizing encephaloceles of the LSS based on a review of 49 patients. The classification system had 4 types of LSSR encephalocele; type I encephaloceles extended superomedial to the facial recess and medial to the Vidian canal (within Sternberg canal), type II were those superomedial to the foramen rotundum and intruding into the sphenoid sinus more medially, type III were inferolateral to the foramen rotundum and extending more laterally, and type IV eroded the foramen rotundum and surrounded V2 with extension in both the medial and lateral directions. The type III LSSR encephalocele was the most common (71.4%) followed by type IV (16.3%).
The patient in our case presented with multiple encephaloceles, but given their proximity and location would be most consistent with a type III encephalocele, isolated lateral to the foramen rotundum and Vidian canal. For type III encephaloceles, we recommend the nerve-sparing window technique described above. This technique was first illustrated by Dr. Bolger in 2005 in a series of 9 patients, 6 of which had LSSR encephaloceles. In this cohort, only 1 patient had postoperative V2 and palatal numbness due to the need to divide the sphenopalatine ganglion for access to a large encephalocele. 13 Alexander et al. 14 expanded on this approach, devising an algorithm for how to best approach LSSR encephaloceles. The primary branch point in their algorithm was whether the skull-base defect was lateral to the foramen rotundum and inaccessible via angled endoscopes, in which case a windowed endoscopic transpterygoid approach was utilized or if it was medial to the foramen rotundum or had minimal LSSR pneumatization, in which case a transnasal sphenoidotomy would be appropriate. Not accounted for in this algorithm are those patients with large or type IV encephaloceles where a combination approach with potential sphenopalatine ganglion sacrifice may be required for adequate exposure.
Conclusion
IIH is an uncommon cause of CSF leak, but its incidence has been increasing in line with increased rates of obesity. It is vitally important that surgeons engaging in skull-base repair understand the medical and surgical treatment of CSF leaks, particularly at the lateral sphenoid sinus recess. We present a case of a patient with multiple skull-base dehiscences in close proximity that were successfully managed by medical management with acetazolamide and a nerve-sparing windowed transpterygoid approach without facial numbness, dry eyes, or recurrence of leak.
Footnotes
Consent to Participate
Written informed consent was obtained from the patient for the publication of this case report.
Consent to Publication
This article is original and has not been submitted elsewhere in part or in whole.
Author Contributions
All authors reviewed the case, contributed to writing and editing the manuscript, and approved the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
N/A.