
Abstract
Sinonasal angioleiomyomas (SNALMs) are rare, typically indolent tumors that present as painless, slow-growing nasal masses arising from the nasal septum, inferior turbinate, or nasal vestibule with minimal local invasion. We present a case of a 39 year-old man with no relevant past medical history with a uniquely aggressive case of a SNALM originating in the pterygopalatine fossa (PPF) with expansile erosion of adjacent skull base structures—an unusual radiographic feature for a tumor classically considered nondestructive. Clinically, the patient’s presentation with severe ipsilateral posterolateral headaches and rapid-onset nasal obstruction further deviates from the expected course, highlighting an atypical symptom profile not previously associated with SNALMs. Surgical excision of the mass was curative with resolution of headaches and no tumor recurrence at 7 months of follow-up. This case expands the current understanding of the clinical and radiographic spectrum of SNALMs and reinforces the importance of considering them in the differential diagnosis of vascular skull base lesions.
Introduction
Angioleiomyomas (ALMs) are benign, pericytic tumors arising from vascular smooth muscle. Sinonasal ALMs (SNALMs) most commonly present in patients in their sixth decade of life with no gender predilection. Endoscopic resection with negative margins is the treatment of choice with favorable prognosis and low recurrence rates. 1 Most commonly, these masses present as painless, slow-growing, solitary masses with symptoms of nasal obstruction and epistaxis. They are pedicled along the nasal septum, inferior turbinate, or nasal vestibule. 2 Only once previously has a SNALM been documented to occur within the pterygopalatine fossa (PPF), presenting as an isolated mass extending into the nasal cavity with minimal symptoms other than chronic congestion. 3 We present a novel case of a SNALM that presented as a PPF mass with expansile skull base erosion that was successfully managed by endoscopic resection. This case represents an exceedingly uncommon but potentially confounding presentation of a rare sinonasal mass.
Case
A 39 year-old male presented to the emergency department with 1 week of rapidly progressive left-sided nasal obstruction and severe ipsilateral posterolateral headaches. He denied visual changes, epistaxis, nasal drainage, or facial/dental numbness. Computed tomography demonstrated a lesion within the left posterior nasal cavity with apparent extension into the PPF with resultant erosion of the pterygoid plates, sphenoid body, greater sphenoid wing, and sphenoid sinus floor. There was additional expansion of the Vidian canal, likely from direct tumor extension, with resultant tumor extension into the sphenoid sinus. Magnetic resonance imaging (MRI) demonstrated a heterogeneously enhancing mass without apparent intracranial extension (Figure 1). Nasal endoscopy demonstrated a submucosal mass arising from the lateral nasal wall, causing nasal cavity obstruction, with apparent submucosal involvement of the inferior turbinate.
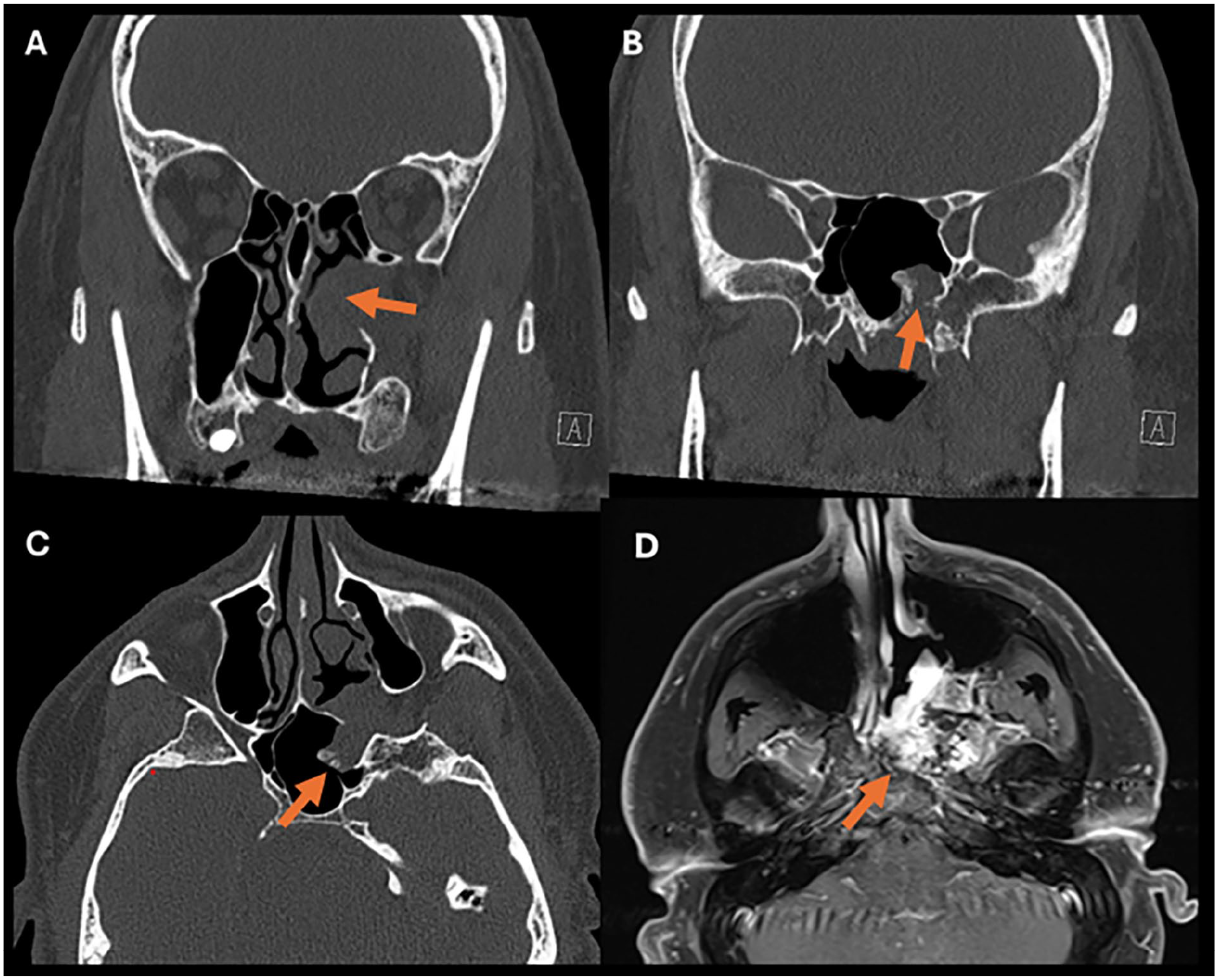
CT Imaging depicting left sided sinonasal mass. (A) Coronal view with expansile mass of left PPF with extension into nasal cavity. (B) Posterior view demonstrating erosion of the sphenoid bone with tumor eruption into the left sphenoid sinus (orange arrow). (C) Axial view demonstrating widening of PPF with additional expansion of tumor posteriorly along the Vidian canal and into the sphenoid sinus (orange arrow). (D) Axial T1 postcontrast image demonstrating heterogeneously enhancing lesion. CT, computed tomography; PPF, pterygopalatine fossa.
The patient subsequently underwent an endoscopic excisional biopsy. Intra-operatively, the tumor was noted to be highly vascular with apparent feeding vessels noted to arise from the internal maxillary artery at the pterygomaxillary fissure. The tumor was well encapsulated but with apparent erosion into the pterygoid plates and sphenoid bone with approximation to the inferior orbital fissure and pterygomaxillary fissure. The Vidian canal was widened with direct tumor extension posteriorly and into the sphenoid sinus and anteriorly into the maxillary sinus, although the adjacent neurovascular structures remained intact. Gross total resection was achieved, and the patient was subsequently discharged without complication. The patient noted resolution of headaches promptly after surgical resection and remains recurrence-free at 7 months follow-up. Final histopathology demonstrated a SNALM with predominately adipocytic differentiation in a background of mixed venous and cavernous histologic subtype (Figure 2).
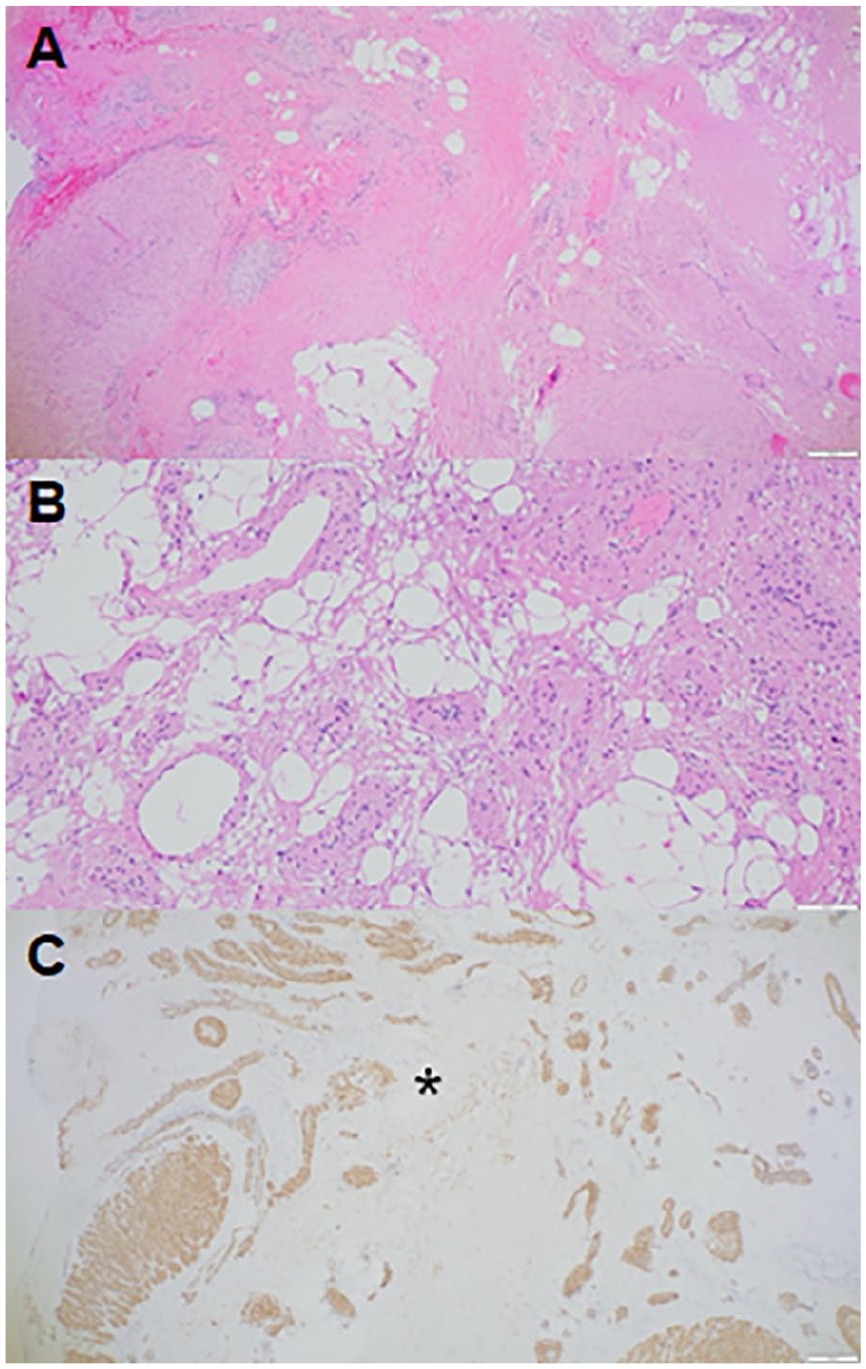
Histologic sections of sinonasal angioleiomyoma with adipocytic differentiation. (A) H&E, 40× and (B) H&E, 100× show numerous bland-appearing vessels of various size and caliber, admixed with mature adipose tissue in a haphazard fashion. (C) SMA, 40× highlights smooth muscle within vessel walls, as well as focal stroma (*). SMA, smooth muscle actin.
Discussion
ALMs are benign smooth muscle tumors that most commonly arise in the extremities, with 76% occurring in the lower limbs and 21% in the upper limbs. 4 These lesions typically present as solitary, firm, and slow-growing nodules. 1 Prognosis following surgical excision is excellent, with recurrence reported in only 2.8% of cases involving the lower extremities. 5 Head and neck ALMs are rare, accounting for only 3% of all ALMs. 4 Within this subgroup, common tumor sites include the buccal mucosa, parotid gland, and palate. Like ALMs found in the extremities, head and neck ALMs are benign and exhibit a <1% recurrence rate. 6 SNALMs represent an uncommon subset of ALMs, comprising ~10% of head and neck ALMs and <1% of all ALMs. As with other sites, SNALMs are benign with a low recurrence rate (<1%) after primary resection. Most SNALMs present as painless masses (73%) with progressive nasal obstruction (67%) and epistaxis (41%). 7
There are 3 predominant histologic subtypes of SNALMs; solid (44%), venous (42%), and cavernous (14%). 2 In the extremities, pain is often a predominant feature of solid histologic subtypes, present in up to 89% of patients, but is relatively uncommon in tumors of the head and neck, and particularly uncommon in SNALMs. 8 Pain, when present, has been correlated with the presence of nerve fibers within the tumor and is thought to result from smooth muscle contraction leading to local ischemia and compression of intra-tumoral nerve fibers.1,6 When pain is present in SNALMs, it typically manifests as localized facial pain. 2 The patient in this case presented with adipocytic differentiation in a background of mixed venous and cavernous features. Adipocytic differentiation is uncommonly reported and has been poorly characterized in the existing literature. 9
SNALMs typically appear as well-circumscribed, homogeneous masses that exhibit a primarily expansile growth pattern rather than invasive destruction of surrounding structures. On MRI, they demonstrate isointense signal on T1-weighted images and are slightly hyperintense on T2-weighted sequences compared to gray matter with moderate enhancement following contrast administration. 10 SNALMs are generally relatively small at presentation, with an average size of 1.8 cm reported in prior cases, likely reflecting earlier presentation due to nasal obstruction or epistaxis. 2 In this case, our patient presented with a tumor of 3.9 cm in greatest dimension, likely reflecting the more expansile nature of this specific lesion within the PPF.
Involvement of the PPF by SNALM is exceedingly rare, with only 1 case previously reported in the literature. 3 In that case, the tumor was located predominately within the lateral nasal cavity with only mild expansion of the PPF without significant invasion that presented as a painless mass with progressive nasal obstruction. Complete surgical excision was curative without recurrence. The patient in this case presented with a more locally destructive lesion than previously seen in the literature with extension into and destruction of multiple adjacent structures within the PPF and sphenoid sinus in the setting of severe ipsilateral posterolateral headaches and rapidly progressive nasal obstruction. Despite its locally aggressive presentation, surgical excision was curative with complete resolution of the patient’s severe headaches postoperatively.
SNALMs arising from the PPF can be challenging to distinguish from other skull base or sinonasal pathologies based on clinical presentation and imaging alone. Differential diagnoses include myopericytoma, glomus tumor, fibromyoma, schwannoma, leiomyosarcoma, angiofibroma, hemangioma, and angiomyolipoma.2,11 Given the significant radiographic and clinical overlap with other lesions, histopathological confirmation is critical for accurate diagnosis. Gross total surgical resection remains the mainstay of treatment, followed by postoperative surveillance.
Conclusion
SNALMs are exceedingly rare with <90 documented cases in the literature and only 1 other case presenting as a mass within the PPF. We present a discussion on this locally aggressive, highly vascular, but benign tumor that can be managed by gross total resection with excellent prognosis.
Footnotes
Author Note
This article is original and has not been submitted elsewhere in part or in whole.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report.
Author Contributions
Mr Leo Song drafted the manuscript and conducted the literature review. Dr Chana R. Sachs provided histopathological imaging and assisted with figure preparation. Dr Jeffrey D. Suh supervised the project as the attending otolaryngologist and provided radiographic images. Dr Jakob L. Fischer served as the primary advisor, contributing to study design, manuscript development, and critical revisions. All authors reviewed and approved the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.