
Abstract
We report a life-threatening post-intubation cricoid abscess in a 29-year-old diabetic male, highlighting the challenges of airway compromise management. Following 7 days of mechanical ventilation for severe pneumonia, the patient developed acute dysphonia, inspiratory stridor, and progressive dyspnea culminating in resting respiratory distress (ambulation <10 m). Bedside laryngoscopy revealed a 70% obstructing subglottic mass with inflammatory changes. Contrast computed tomography identified a 23 mm rim-enhancing cricoid abscess causing critical airway stenosis. Immediate tracheostomy secured the airway, with subsequent operative drainage yielding Streptococcus species resistant to first-line antibiotics. Targeted IV ceftazidime and oral ciprofloxacin achieved resolution, permitting decannulation at 21 days. This case underscores 3 critical lessons: (1) the heightened infection risk in diabetics post-intubation, (2) the value of rapid endoscopic airway assessment in post-extubation dyspnea, and (3) the necessity of culture-directed therapy in deep neck space infections. Unlike typical laryngotracheal complications (eg, granulomas or stenosis), abscess formation at the cricoid represents a rare but potentially fatal etiology of post-intubation airway obstruction requiring multidisciplinary intervention. Early imaging and surgical drainage proved pivotal in preventing catastrophic outcomes in this immunocompromised host.
Key Clinical Message
This life-threatening post-intubation cricoid abscess case highlights the critical need for prompt airway evaluation in diabetic patients with post-extubation respiratory distress, emphasizing the diagnostic value of bedside laryngoscopy and computed tomography (CT) imaging, the necessity of culture-directed antibiotics for resistant organisms, and the importance of multidisciplinary ENT-critical care collaboration in managing severe airway stenosis.
Introduction
Post-intubation airway complications typically involve granulomas, stenosis, or laryngeal edema, with cricoid abscesses representing an exceptionally rare but life-threatening entity. 1 While diabetes mellitus is a known risk factor for infections, its association with deep neck space infections following intubation remains poorly documented in the literature. 2 This case report describes a 29-year-old insulin-dependent diabetic male who developed a streptococcal cricoid abscess with 70% airway obstruction following prolonged mechanical ventilation for pneumonia. The clinical presentation mimicked more common post-intubation complications, underscoring the diagnostic challenge.
Current guidelines emphasize prompt recognition of airway compromise, yet specific protocols for managing post-intubation cricoid infections are lacking. 3 We highlight the critical role of urgent endoscopic evaluation, CT imaging, and multidisciplinary management in preventing fatal outcomes. This report contributes to the limited body of evidence on this rare complication while reinforcing the importance of considering atypical infections in immunocompromised patients with post-extubation respiratory distress.
Case Report
A 29-year-old man with type 1 diabetes mellitus (on insulin therapy) and a recent history of severe pneumonia requiring 7 days of orotracheal intubation presented with persistent hoarseness, inspiratory wheezing, and progressive dyspnea following extubation. One day post-discharge from the ICU, he developed worsening dyspnea at rest, limiting his ambulation to 10 m. Clinical examination revealed marked suprasternal retractions, a respiratory rate of 20 breaths/min, and oxygen saturation of 92% on room air without cyanosis. Flexible laryngoscopy identified an inflammatory nodule between the right arytenoid and vocal cord, accompanied by significant salivary stasis and a posterior subglottic bulge causing 70% airway obstruction (Figure 1).
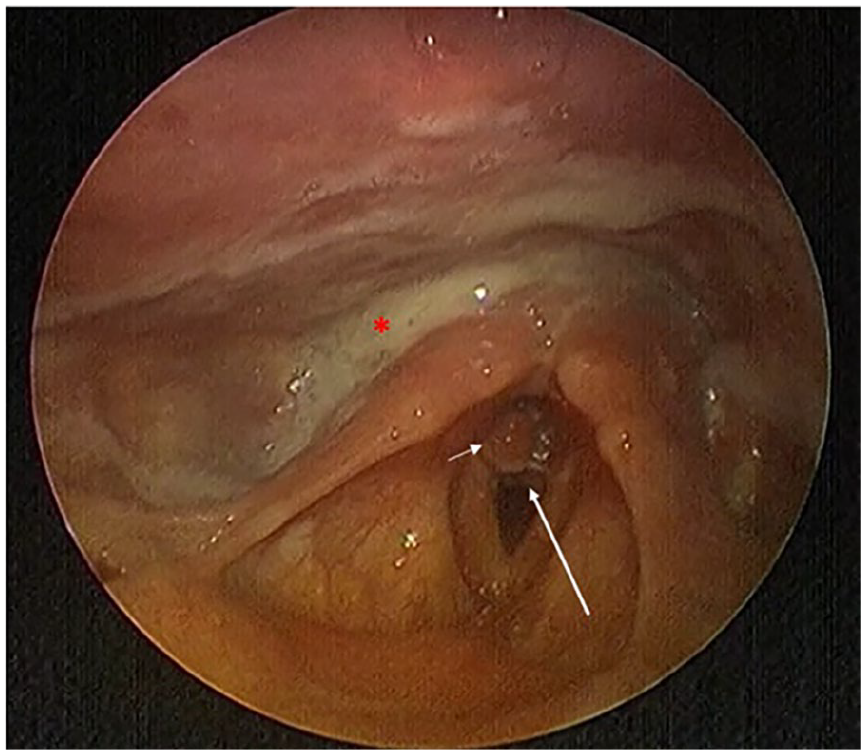
Indirect laryngoscopy demonstrating salivary stasis (asterisk), an inflammatory nodule between the right arytenoid and vocal cord (short white arrow), and posterior subglottic bulge causing airway narrowing (long white arrow).
Emergency CT imaging demonstrated a 23 mm rim-enhancing abscess at the cricoid level, severely narrowing the airway (Figure 2).
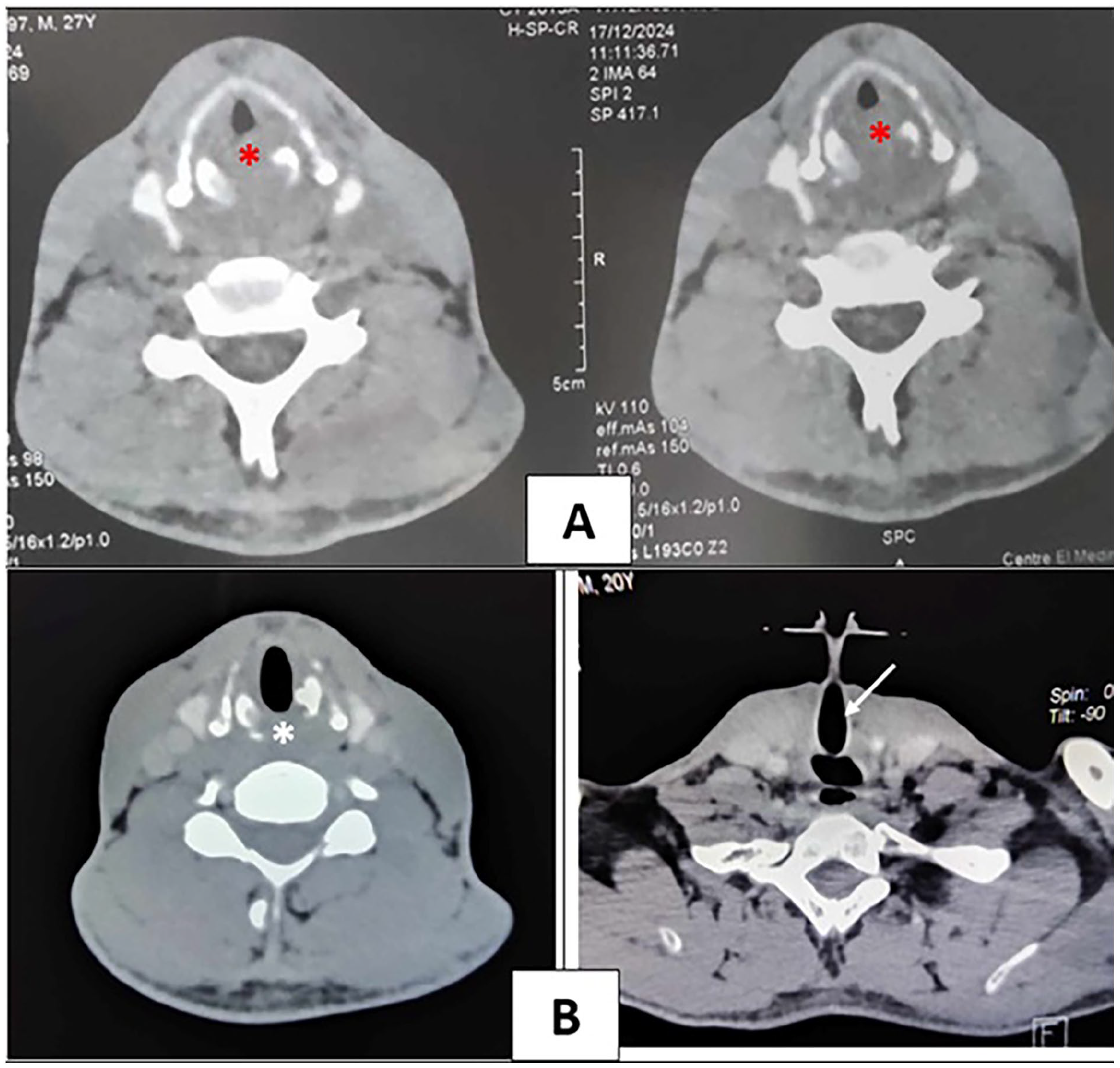
(A) Rim-enhancing abscess at the cricoid level, severely narrowing the airway (red asterisk). (B) Follow-up CT scan showing resolution of the cricoid-associated subglottic abscess (white asterisk) and tracheostomy tube placement above the lesion (white arrow), ensuring airway patency.
Initial management included urgent tracheostomy under local anesthesia to secure the airway, followed by direct laryngoscopy with abscess drainage under general anesthesia. Cultures grew resistant to Streptococcus, prompting a 15-day course of intravenous ceftazidime (1 g TID) and oral ciprofloxacin (500 mg BID). The patient showed rapid clinical improvement, with follow-up CT confirming abscess resolution (Figure 2). Successful decannulation was performed 21 days post-tracheostomy, with complete restoration of airway patency and voice quality.
Discussion
This case of post-intubation cricoid abscess in a diabetic patient represents a critical intersection of infectious disease, airway management, and immunocompromised host pathology that challenges conventional diagnostic algorithms for post-extubation complications. While contemporary literature well characterizes laryngeal injuries following intubation, with meta-analyses reporting incidence rates of 19% to 37%, 4 the development of cricoid abscess remains exceptionally rare, with <20 documented cases in the past decade 5 and none reporting the unique combination of diabetic comorbidity, resistant Streptococcus infection, and degree of airway obstruction (70%) presented here. The patient’s initial symptoms of progressive dyspnea and inspiratory stridor created a diagnostic dilemma by mimicking more common post-intubation sequelae like granuloma formation or tracheal stenosis, 3 highlighting the importance of maintaining broad differential diagnoses in patients with risk factors for atypical presentations. Pathophysiologically, this case illustrates the dangerous synergy between mechanical trauma from prolonged intubation (7 days in our patient) and microbial pathogenesis, where endotracheal tube biofilm formation (documented to occur in 85% of tubes after 48 hours 6 ) enables bacterial invasion of the vulnerable cricoid perichondrium – a process dramatically accelerated in our diabetic patient due to well-documented impairments in neutrophil chemotaxis and phagocytosis 7 combined with microangiopathy-induced local tissue hypoxia. The isolation of ceftriaxone-resistant Streptococcus pneumoniae in our cultures reflects the escalating crisis of antimicrobial resistance in ICU-acquired infections, with recent surveillance data showing 32% resistance rates among respiratory isolates,8,9 necessitating both aggressive empiric coverage and rapid de-escalation based on culture results to balance efficacy and antimicrobial stewardship. Our diagnostic approach, combining immediate bedside laryngoscopy with subsequent contrast-enhanced CT, validated current guidelines recommending multimodal imaging for atypical post-intubation presentations, 10 with the CT findings of a 23 mm rim-enhancing abscess providing both definitive diagnosis and critical surgical planning information that would have been missed by laryngoscopy alone. The severity of airway compromise in our case (70% obstruction) places it among the most critical reported instances of this rare complication, demonstrating the frightening rapidity with which such infections can progress from mild symptoms to life-threatening stenosis. Our successful outcome was achieved through a meticulously sequenced management strategy beginning with immediate airway stabilization via tracheostomy (remaining the gold standard for critical stenosis 11 ), followed by precise surgical drainage under direct visualization to prevent disastrous mediastinal spread (a complication occurring in 22% of delayed cases per thoracic surgery literature 12 ), and concluding with targeted antibiotic therapy adjusted according to microbiological sensitivities. The 21-day decannulation period achieved in our patient compares favorably with the mean 28 ± 6 days reported in systematic reviews,13,14 potentially attributable to our institution’s protocol of daily laryngoscopic surveillance and early mobilization, though this requires validation in larger studies. This case carries several practice-changing implications: first, it establishes diabetes mellitus as a significant risk factor warranting enhanced post-intubation monitoring protocols; second, it demonstrates that resistant organisms must be anticipated in all ICU-related airway infections; and third, it reinforces the lifesaving value of multidisciplinary teams combining ENT, critical care, and infectious disease expertise. Future research directions suggested by this case include the development of validated risk stratification tools for post-intubation infections, investigation of optimal surveillance protocols for high-risk patients, and clinical trials evaluating novel preventive strategies such as antimicrobial endotracheal tube coatings (shown to reduce biofilm formation by 67% 6 ) or post-extubation proton pump inhibitor prophylaxis. While limited by its single-case design and inability to establish causal relationships, this report makes substantial contributions to the sparse literature on this severe complication by providing the first detailed account of multidisciplinary management in a diabetic host, offering quantitative data on obstruction metrics and recovery timelines, and proposing a standardized approach to diagnosis and treatment that could reduce mortality for this underrecognized condition. Ultimately, this case serves as a potent reminder of the need for heightened vigilance when managing post-intubation respiratory distress, particularly in immunocompromised patients where atypical infections may masquerade as routine complications.
Conclusion
This case highlights the critical importance of considering cricoid abscess in diabetic patients presenting with post-intubation airway obstruction, particularly when symptoms progress despite extubation. The rapid progression to life-threatening stenosis underscores the need for immediate endoscopic evaluation and cross-sectional imaging in such high-risk patients. Our experience demonstrates that multidisciplinary management combining urgent airway stabilization (tracheostomy), targeted surgical drainage, and culture-directed antibiotics can achieve excellent outcomes even in severe cases.
These findings suggest that (1) diabetics may require enhanced surveillance following prolonged intubation, (2) resistant organisms should be anticipated in post-ICU airway infections, and (3) the cricoid region merits special attention during extubation assessments. Future studies should investigate optimal preventive strategies and early diagnostic markers for this rare but devastating complication. This report expands the limited literature on post-intubation cricoid infections while providing an actionable management framework for similar cases.
Footnotes
Acknowledgements
All authors approved the final version and agreed to be responsible for all aspects of the work to ensure that accuracy-related questions were addressed.
Ethics Considerations
Our institution does not require ethical approval for reporting individual cases.
Consent to Participate
Obtained from the patient in writing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.