
Abstract
Histoplasma capsulatum is a dimorphic fungus endemic to the Ohio and Mississippi River valleys. Although pulmonary involvement is most common, rare extrapulmonary manifestations such as laryngeal histoplasmosis can mimic malignancy and pose diagnostic challenges, particularly in immunosuppressed individuals residing outside endemic areas. We describe a 40-year-old immunosuppressed male on tumor necrosis factor-alpha (TNF-α) inhibitor therapy who presented with progressive dysphagia, hoarseness, and weight loss. Laryngoscopy revealed verrucous supraglottic lesions concerning for malignancy. Imaging further raised suspicion for neoplastic or granulomatous disease. However, biopsy revealed H. capsulatum and confirmed with fungal staining. The patient failed initial treatment with oral itraconazole and required escalation to intravenous amphotericin B, followed by long-term oral antifungal therapy. Discontinuation of infliximab and close multidisciplinary follow-up led to full clinical resolution. This case highlights the importance of considering histoplasmosis in the differential diagnosis of laryngeal lesions, even in non-endemic regions and HIV-negative patients. Immunomodulatory therapies such as TNF-α inhibitors increase susceptibility to disseminated fungal infections. Early biopsy, appropriate fungal staining, and prompt antifungal therapy are critical for accurate diagnosis and successful treatment of this rare but serious presentation.
Introduction
Histoplasma capsulatum is a fungus endemic to the Ohio and Mississippi River valleys. 1 The clinical spectrum ranges from asymptomatic to life-threatening disseminated disease, depending on host immunity. Immunocompetent individuals may experience mild respiratory illness, whereas immunosuppressed patients, especially those with HIV, are at increased risk of extrapulmonary involvement. 1 Although pulmonary infection is most common, Histoplasma can rarely involve the mucosal surfaces of the head and neck, mimicking squamous cell carcinoma or granulomatous infections.1,2
While laryngeal histoplasmosis is well documented in immunocompromised HIV-positive patients, fewer reports exist in HIV-negative individuals on tumor necrosis factor (TNF) inhibitors. Moreover, outside endemic areas, such diagnoses are often delayed due to low clinical suspicion. This case illustrates the diagnostic challenge posed by such presentations and underscores the importance of maintaining a broad differential.
Case Report
A male patient in his 40s presented to the emergency department (ED) with a 2-month history of progressive dysphagia, odynophagia, cough, hoarseness, otalgia, and a significant weight loss of 20 pounds. He denied hemoptysis, fevers, dyspnea, or shortness of breath. His medical history included rheumatoid arthritis, managed with infliximab (a monoclonal antibody that inhibits TNF-α, used in rheumatoid arthritis and other autoimmune conditions). He was a former 2 pack/day smoker with no recent travel to Histoplasma-endemic areas. The patient appeared clinically stable, and there was no concern of an airway obstruction, as the patient was not in acute distress.
During the patient’s ED visit, Otolaryngology (ENT) was consulted for evaluation. Nasopharyngolaryngoscopy revealed irregular, verrucous mucosa with diffuse thickening of the supraglottic larynx, particularly the epiglottis (Figure 1A). There was no airway obstruction. Computed tomography (CT) of the neck demonstrated asymmetric soft tissue thickening with nodular enhancement involving the epiglottis and aryepiglottic folds, along with left-sided cervical lymphadenopathy (Figure 1B–D). Chest CT revealed bilateral reticulonodular densities (Figure 1E), raising suspicion for a systemic inflammatory or infectious process.
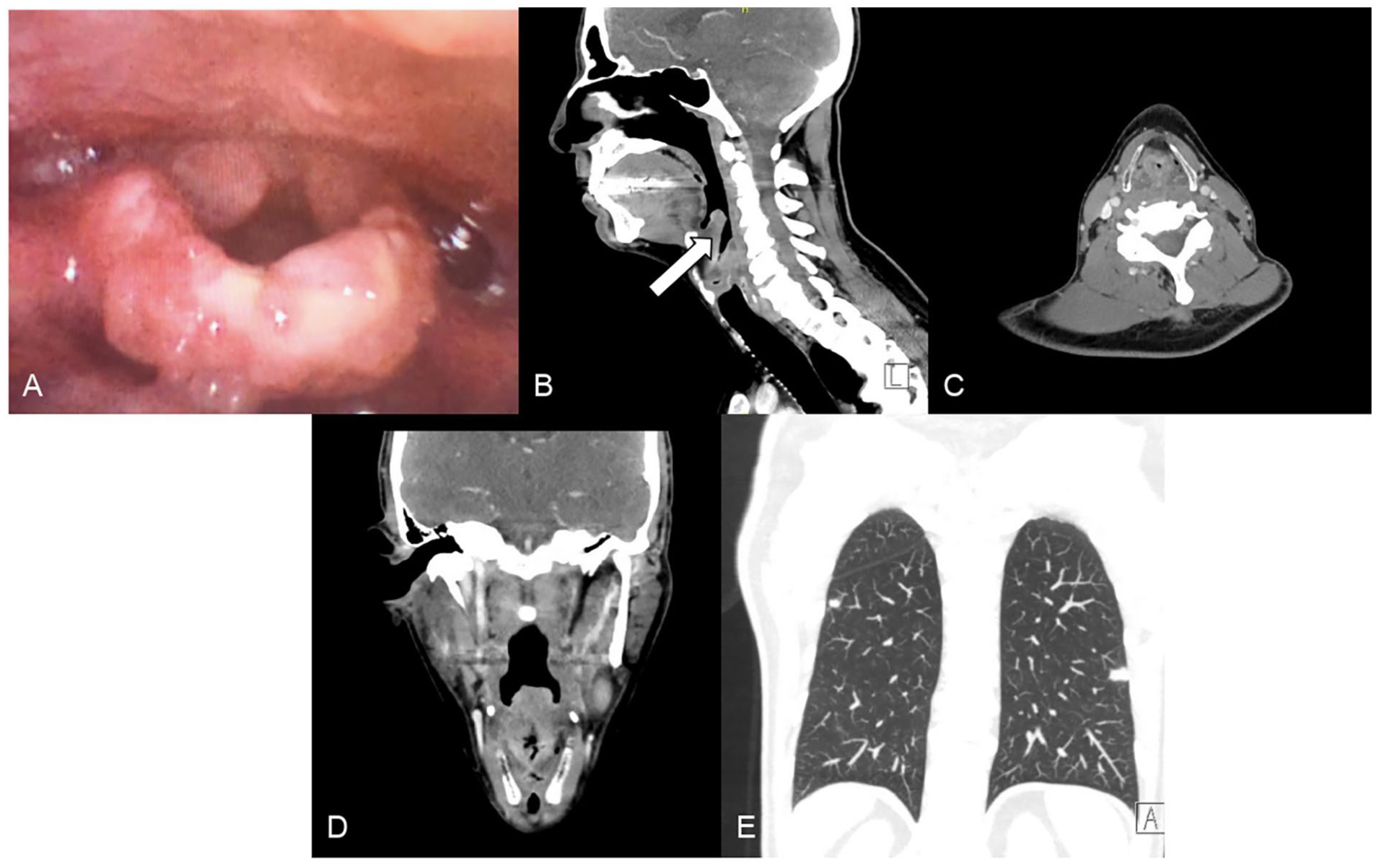
(A) Nasopharyngolaryngoscopy (NPL) demonstrating irregular, verrucous mucosal changes involving the supraglottic larynx. Findings were initially concerning for malignancy. (B) Sagittal, (C) axial, and (D) coronal CT images of the neck demonstrating diffuse thickening and irregularity of the supraglottic laryngeal (arrow in B) structures. (E) Coronal CT of the chest showing bilateral reticulonodular opacities, suggestive of a possible infectious or granulomatous process.
The differential diagnosis included squamous cell carcinoma, given the patient’s smoking history and the verrucous appearance of the laryngeal mucosa. Other considerations included granulomatous diseases such as tuberculosis or sarcoidosis, and less likely fungal infections. Due to the patient’s immunosuppressive therapy with infliximab, invasive fungal disease was also considered. The combination of mucosal thickening and pulmonary findings made malignancy with metastasis or disseminated infection the most probable working diagnoses.
The patient underwent direct laryngoscopy with biopsy the following day. Histopathology revealed reactive squamous mucosa with intracellular yeast-like organisms measuring 2 to 4 microns, morphologically consistent with H. capsulatum (Figure 2). Gomori methenamine silver and periodic acid–Schiff (PAS) stains confirmed the presence of numerous yeast forms (Figure 2). There was no evidence of malignancy. The urine Histoplasma antigen level was mildly elevated at 0.3 ng/mL. Serum antibody testing was negative, likely due to immunosuppression.
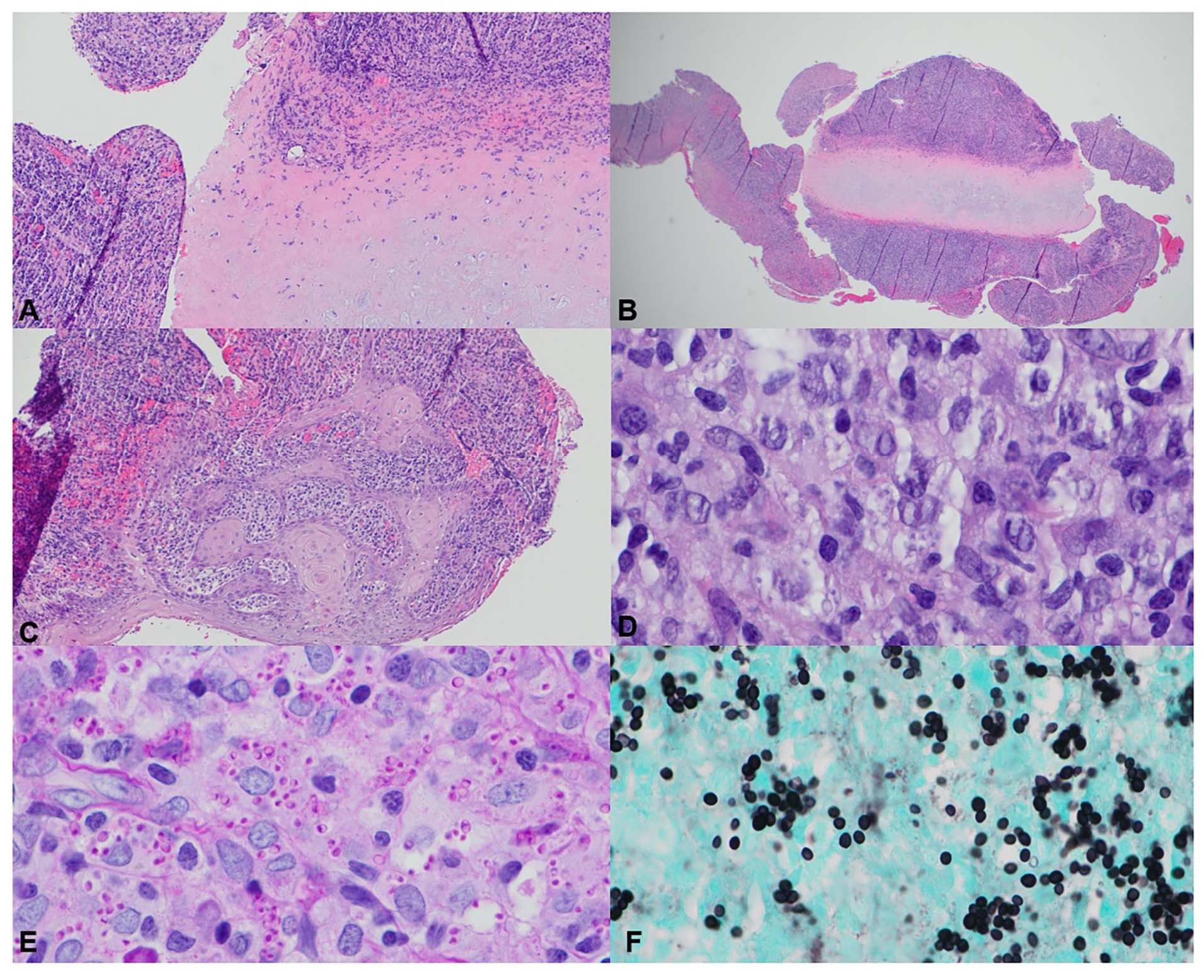
Histopathologic analysis of the epiglottic biopsy. (A) Erosion of the epiglottic cartilage (H&E, 10×). (B) Diffuse inflammation of the epiglottis (H&E, 2×). (C) Reactive squamous mucosa (H&E, 2×). (D) Hematoxylin and eosin (H&E) stain demonstrating intracellular yeast forms (100×). (E) Gömöri’s methenamine silver (GMS) stain highlighting fungal yeast forms (100×). (F) Periodic acid–Schiff (PAS) stain confirming fungal yeast morphology (100×).
He was initially treated with oral itraconazole (200 mg twice daily). Due to minimal symptomatic improvement, he was transitioned to intravenous amphotericin B (1 mg/kg/day) for 14 days. Infliximab therapy was discontinued. He subsequently resumed oral itraconazole with plans to continue for at least 12 months. Repeat CT chest imaging, complete blood counts, liver and renal function tests, serum itraconazole levels, and urine Histoplasma antigen were monitored at regular intervals.
Notably, the decision to escalate treatment to amphotericin B was based on poor initial response and concern for disseminated histoplasmosis. Intravenous amphotericin remains the gold standard for severe or refractory infections, particularly in immunocompromised patients.
At follow-up, the patient demonstrated full resolution of dysphagia and voice changes. He gained back 15 pounds, denied any further respiratory symptoms, and remained stable on oral antifungal therapy. ENT follow-up laryngoscopy showed near-complete normalization of the epiglottic tissue. He continues outpatient care with ENT and rheumatology.
Discussion
H. capsulatum is a dimorphic fungus first described over a century ago. 3 While most cases in the United States arise in the Ohio and Mississippi River valleys, sporadic infections have been reported in other geographic regions. 4 In our patient, who resided in a non-endemic area and denied travel, the source of exposure remains unclear. Environmental reservoirs such as bat droppings, old buildings, or contaminated soil may harbor the organism.
A 2020 review by Mittal et al highlighted that laryngeal histoplasmosis can closely mimic malignancy on both imaging and histology, often resulting in diagnostic delays. 2 Similarly, Miller et al reported that histoplasmosis is frequently misdiagnosed at initial presentation, commonly mistaken for bacterial pneumonia, malignancy, or tuberculosis, with many patients experiencing a delay in diagnosis of over 50 days. 1 This overlap underscores the importance of early tissue biopsy and fungal staining in patients with atypical mucosal lesions, particularly when symptoms persist despite empiric antibiotic therapy.
Our case highlights a less commonly recognized risk factor: TNF-α inhibitors. These biologics, while effective in treating autoimmune conditions, impair granuloma formation, rendering patients more susceptible to intracellular pathogens like Histoplasma. 5 Infliximab and other anti-TNF agents are recognized by the CDC and IDSA as risk factors for disseminated fungal infections.
Histologically, pseudoepitheliomatous hyperplasia and granulomatous inflammation can mimic malignancy or tuberculosis. Thus, special stains (PAS, GMS) are essential for definitive diagnosis. Serum testing may be falsely negative in immunosuppressed patients, making urine antigen and biopsy more reliable.
Management of laryngeal histoplasmosis depends on disease severity and host immune status. Mild, localized disease in immunocompetent individuals may respond to itraconazole alone. By contrast, more severe or refractory infections typically require induction with amphotericin B followed by a prolonged course of oral itraconazole. 6 Our patient’s favorable outcome reflects timely escalation to amphotericin and appropriate de-escalation of immunosuppression.
Conclusion
This case highlights the importance of maintaining a broad differential diagnosis and considering uncommon etiologies in immunosuppressed patients. Histoplasmosis should remain on the diagnostic radar even in HIV-negative individuals receiving immunomodulatory therapy. While pulmonary involvement is the most frequent manifestation, head and neck presentations such as laryngeal lesions may occur and can mimic malignancy. Accurate diagnosis relies on a combination of imaging, tissue biopsy, and fungal staining, but early clinical suspicion is essential to avoid delays in recognizing this rare presentation.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report.
Author Contributions
John J. Alfarone: writing – original draft, writing – review and editing, conceptualization, investigation. Evan B. Hughes: project administration, supervision, conceptualization, investigation. Shridevi D. Karikehalli: resources, conceptualization, investigation. Samantha Terhaar: project administration, supervision, conceptualization, investigation. Nima Vahidi: project administration, supervision, conceptualization, investigation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data relevant to this case report are included within the article. Additional clinical details are available upon request from the corresponding author.