
Abstract
Bullous pemphigoid (BP) is an autoimmune blistering disease that affects primarily the skin and rarely involves the mucosa of the oral cavity, larynx, pharynx, or esophagus. Diagnosis is based on the clinical presentation, histology, and immunopathological examination. Laryngeal involvement in BP is extremely rare and patients may be asymptomatic or may present with dysphonia, dysphagia, and/or respiratory distress. The authors of this article report a rare case of BP with laryngeal involvement with a review of the literature. Early diagnosis and initiation of treatment is highly recommended to prevent any long-term complications.
Introduction
Bullous pemphigoid (BP) is an autoimmune disorder predominantly diagnosed in elderly. It affects primarily the skin, resulting in subepidermal blistering mostly over the flexor surfaces, axilla, lower trunk, and groin. In rare cases, it involves the mucosa of the oral cavity, larynx, pharynx, and esophagus. 1 Laryngeal involvement in BP is extremely rare with only few cases reported in the literature.1-4 Patients may be asymptomatic or may present with dysphonia, dysphagia, and/or respiratory distress. 3 The most common findings on laryngeal examination are erythema and diffuse white plaques mostly seen in the supraglottic region. 3 The diagnosis of BP is challenging given the alternating periods of flares and remission and the wide differential diagnosis that includes disorders such as pemphigus vulgaris, IgA dermatosis, epidermolysis bullosa acquisita, and mucous membrane pemphigoid. 1
Based on a literature review of PubMed, Scopus, and EMBASE using keywords “bullous,” “pemphigoid,” “larynx,” “laryngeal,” “hoarseness,” “dysphonia,” and “dysphagia,” only 4 articles in the English language on laryngeal involvement in patients with BP have been reported. The authors of this article describe a rare case of laryngeal BP with a review of the literature.
Case Report
An 86-year-old female presented to the dermatology clinic with itching and small blisters in her upper extremities, chest, and thighs for the past 3 months. A skin biopsy revealed IgG and C3 immune reactant deposits at the dermo-epidermal junction. Microscopic examination also showed superficial perivascular and interstitial lymphocytic inflammatory cell infiltrate (Figure 1). These findings were consistent with the diagnosis of BP based on the histopathological and immunofluorescence criteria described by Bağcı et al. 4 The patient was started on Dermovat cream (topical steroids) with no significant improvement. One month later, she started complaining of severe sore throat with a change in voice quality that prompted an ear, nose, and throat consultation. On presentation to the voice and swallowing clinic, her voice was perceived as mildly dysphonic with asthenia. Laryngeal endoscopy revealed diffuse whitish lesions, ulcerative in nature involving the laryngeal and lingual surfaces of the epiglottis (Figure 2a). An office-based biopsy of these lesions was performed under local anesthesia and showed necrosis and inflammatory cells (Figure 2b). Direct immunofluorescence staining on the specimen was nonrevealing. The patient was started on a course of prednisone 20 mg along with proton pump inhibitor twice daily. On follow-up 1 month later, she had marked improvement in her swallowing and voice quality. Repeated laryngeal examination showed disease regression.
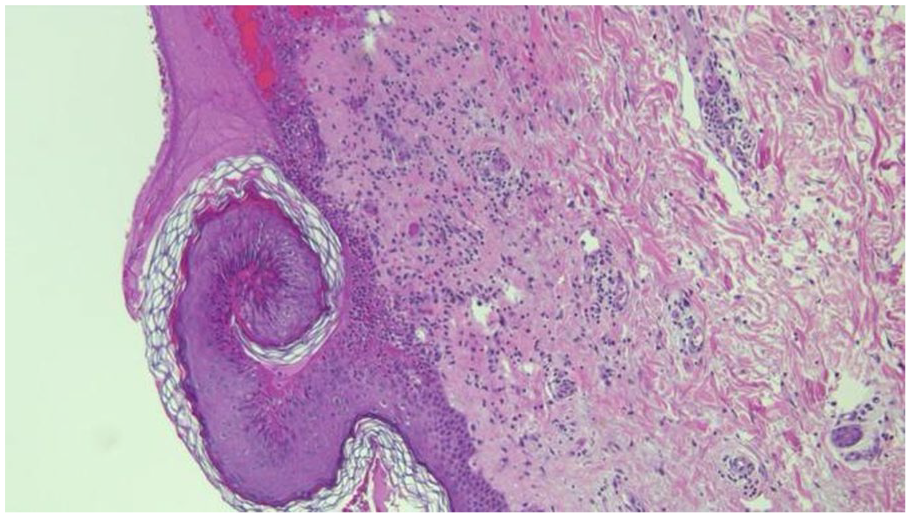
Microscopic findings showing superficial perivascular and interstitial lymphocytic inflammatory cell infiltrate.
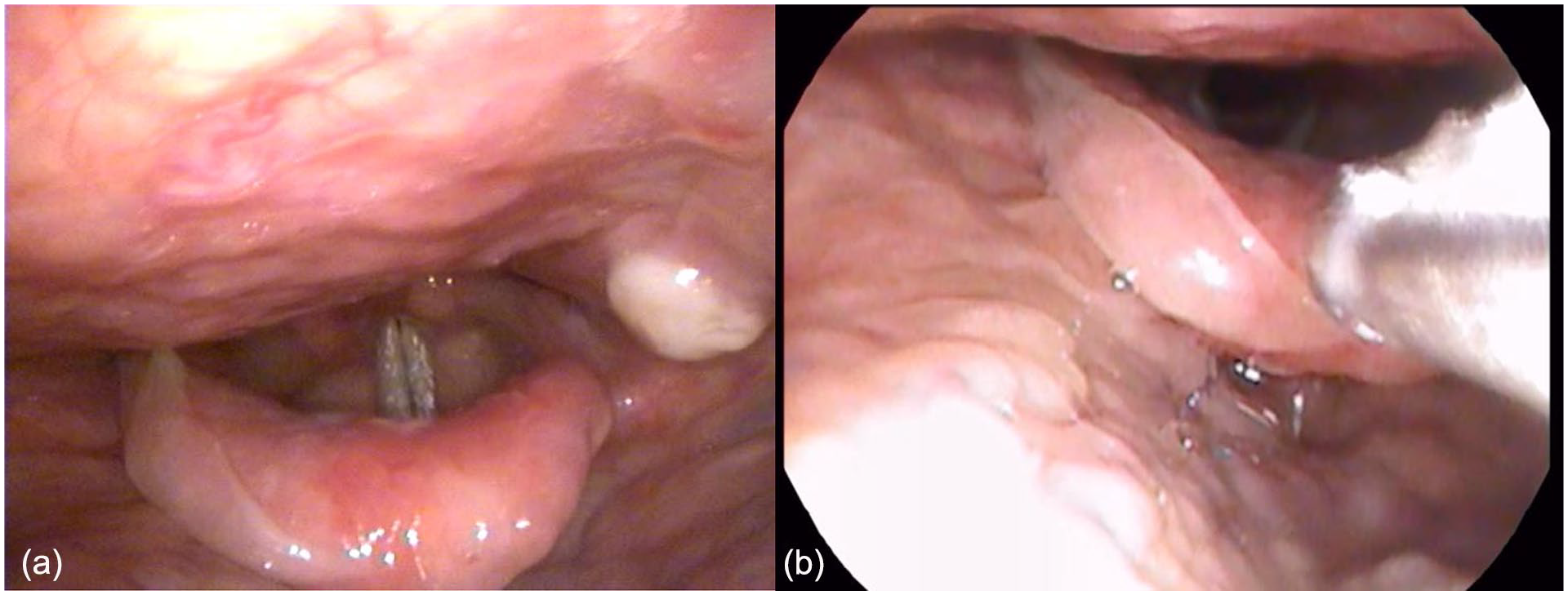
(a) Endoscopic image of the larynx showing white ulcerative lesions on the epiglottis and lateral pharyngeal wall. (b) Endoscopic image of the larynx showing biopsy of the epiglottic lesions.
Discussion
BP is an uncommon autoimmune disorder with many systemic manifestations. The clinical course depends on the extent of the disease and affected sites. 3 The workup of BP is challenging and other nonimmunological diseases such as drug reactions, porphyrias, or bullous erythema multiforme must be excluded. 1 The diagnosis is based on the clinical presentation, histology, and immunopathological examination. BP can be distinguished by the presence of circulating autoantibodies against hemidesmosomes located in the epidermal basement membrane targeting 230 kDa (BP230) and 180 kDa (BP180) antigen proteins, which are linked to hemidesmosomes.2,5
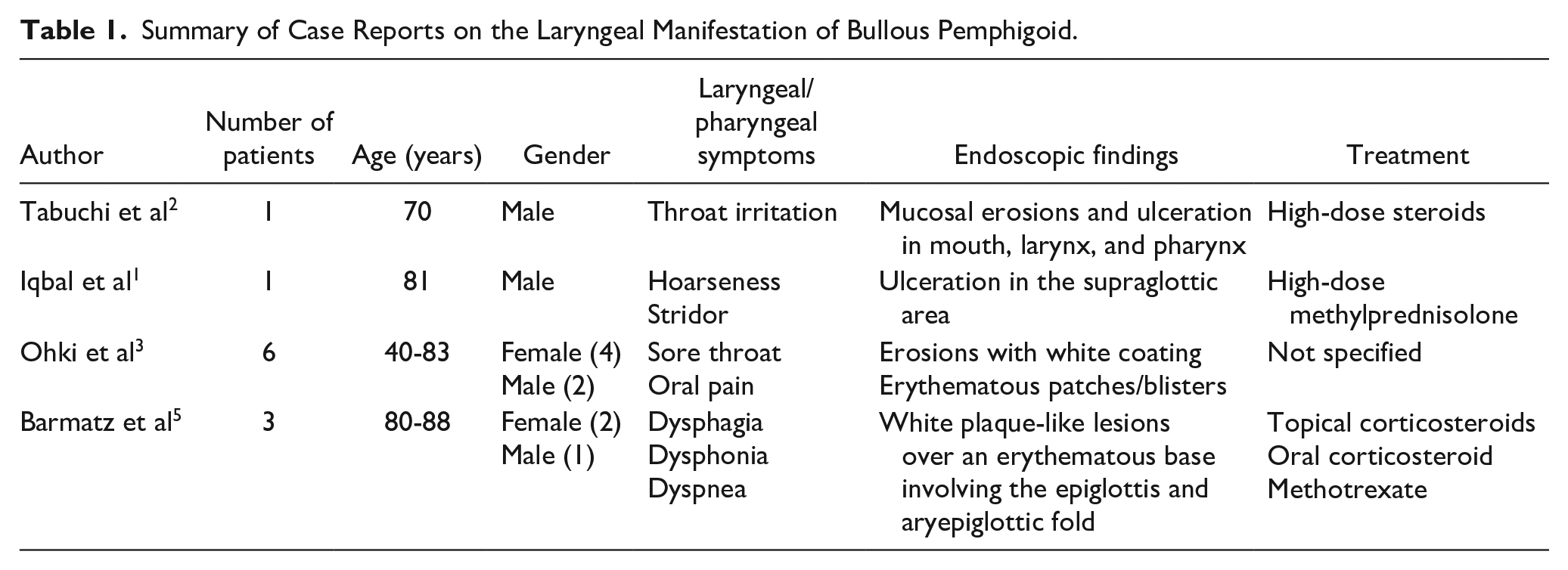
Laryngeal involvement in BP is extremely rare. In 2006, Iqbal et al 1 reported an elderly male who presented with shortness of breath and hoarseness. On examination, he had multiple bullae with an inflamed base involving the extremities as well as the mucosal lining of the buccal area and the supraglottis. Histopathology and immunofluorescent examination of a skin biopsy revealed subepidermal bullae with scant perivascular inflammation and linear deposition of fibrinogen and C3 at the dermo-epidermal junction. These findings were consistent with BP. Patient was treated with a high dose of methylprednisolone followed by immunosuppressive therapy which resulted in significant regression of his disease within the course of 6 months. 1 In 2006, Tabuchi et al 2 described a patient who presented with several small blisters on his trunk associated with throat irritation. Otolaryngologic examination revealed mucosal ulcerations in his mouth, larynx, and pharynx. A biopsy taken from the oral cavity showed IgG deposition along the basement membrane. Enzyme-linked immunosorbent assay revealed the presence of BP180 autoantibodies consistent with the diagnosis of BP. Treatment was initiated with high-dose prednisolone and the mucosal lesions responded gradually. 2 In 2016, Ohki et al 3 described 6 patients with BP who presented with sore throat and oral discomfort. Physical examination revealed skin and mucosal lesions involving different subsites of the upper airway such as the soft palate, epiglottis, gingiva, tongue, nasal cavity, and buccal mucosa. The lesions were described as erythematous and erosive with the presence of white blisters. 3 In 2023, Barmatz et al 5 reported 3 patients with BP who presented with dysphagia, dyspnea, and dysphonia. The most common site of laryngeal involvement was the epiglottis followed by the aryepiglottic fold. The mucosal lesions were described as erythematous and erosive with the presence of adhesions to the surrounding structures. Serology was positive for BP180 antigen in all 3 cases, and skin/mucosal biopsies showed IgG and C3 immune reactant deposits in 2 cases. The first line of treatment was topical corticosteroids followed by high-dose oral corticosteroids and methotrexate 3 (Table 1).
Summary of Case Reports on the Laryngeal Manifestation of Bullous Pemphigoid.
The case described in this article is in alignment with the cases previously reported in the literature. The clinical presentation of chronic sore throat and dysphagia prompted endoscopic examination of the larynx and pharynx, which revealed diffuse ulceration and whitish discoloration of the epiglottic mucosal lining. A mucosal biopsy was taken and the patient was started on systemic steroids, which resulted in disease regression and improvement in symptoms.
Conclusion
The authors of this article report a rare case of BP with laryngeal involvement. Patients with BP who present with voice and/or swallowing symptoms need to be thoroughly examined to rule out any lesion in the laryngopharyngeal complex. The diagnosis hinges on immunopathologic examination of a skin or mucosal biopsy. Early initiation of treatment is highly recommended to prevent any long-term complications. The mainstay therapy is topical and systemic steroids, particularly in the presence of mucosal involvement. For patients who fail initial treatment or those with extensive or recurrent disease, the use of steroid-sparing immunosuppressive agent such as azathioprine and cyclophosphamide is recommended.
Footnotes
Acknowledgements
None.
Author Contributions
All authors contributed to the study’s conception and design. Material preparation and data collection was performed by Jonathan Abou Chaar. The first draft of the manuscript was written by Abdul-Latif Hamdan and Jonathan Abou Chaar, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The American University of Beirut Institutional Review Board has determined that this is not a “Human Subject Research” and hence no ethical approval is required. Therefore, this article does not contain any studies with human participants performed by any of the authors.
Informed Consent
Consent for publication was obtained for every individual person’s data included in the study.