
Abstract
Type I thyroplasty has increasingly been performed on an outpatient basis. Laryngeal reinnervation is recognized for its long-term and functional benefits but is typically performed inpatient under general anesthesia. Herein we report the first published outpatient type I thyroplasty with laryngeal reinnervation performed under monitored anesthesia care (MAC). Three adults underwent type I thyroplasty with ansa cervicalis to recurrent laryngeal nerve (RLN) reinnervation. A 23-year-old female with a history of generalized idiopathic epilepsy s/p vagal nerve stimulator implantation presented with persistent dysphonia. She developed longstanding left vocal fold paralysis. She underwent left type I thyroplasty with silastic implant and ansa cervicalis to RLN neurorrhaphy under MAC-local anesthesia. The patient was discharged home on the day of surgery. Two additional patients underwent the same procedure, including a 58-year-old male with postsurgical dysphonia who was admitted for overnight observation due to a small amount of incisional crepitus and a 23-year-old female with postsurgical vocal cord paralysis who was admitted overnight due to multiple comorbidities. Both were discharged on post-operative day one without issue and demonstrated improvement in voice at follow up. Outpatient type I thyroplasty with laryngeal reinnervation under MAC is feasible with proper patient selection.
Introduction
Unilateral vocal fold paralysis can result in breathy dysphonia, poor vocal endurance, and dysphagia with aspiration. Restoring the glottic valve can be accomplished through a variety of reliable rehabilitation procedures, including vocal fold injection augmentation, vocal fold medialization with thyroplasty or arytenoid adduction (laryngeal framework surgery), or recurrent laryngeal nerve reinnervation. 1 Laryngeal reinnervation has several advantages over other techniques, including potentially restoring voice without changing vocal fold pliability and preventing the loss of thyroarytenoid muscle tone and bulk seen with denervation. 2 Although various techniques have been used, laryngeal reinnervation with ansa cervicalis to recurrent laryngeal nerve (RLN) neurorrhaphy has emerged as the most popular reinnervation technique. 2 It is increasingly used as an approach to rehabilitation, especially in younger patients, either alone or in tandem with laryngeal framework surgery. Combining laryngeal reinnervation with laryngeal framework surgery provides the most comprehensive, long-lasting, and potentially successful approach for restoring function in patients with unilateral vocal fold paralysis. There are limited reports of type I thyroplasty with laryngeal reinnervation in adults. Furthermore, although post-operative care for type I thyroplasty has increasingly been performed on an outpatient basis, with numerous studies demonstrating the safety and cost-effectiveness of same day discharge, there are no published reports of successful outpatient type I thyroplasty with laryngeal reinnervation.3,4
Case Report
A 23-year-old female with a history of chronic left vagal neuropathy presented to clinic. Past medical history was notable for generalized idiopathic epilepsy status post vagal nerve stimulator implantation after which she had persistent dysphonia. The stimulator was ultimately removed when she was 18 years old. She previously had numerous left vocal fold injection medialization procedures that provided limited transient benefit. Initial videostroboscopy demonstrated left vocal fold paralysis and vocal cord atrophy. GRBAS score was 8 with maximum phonation time (MPT) of 8 seconds, fundamental frequency (F0) 244 Hz, and range 340 Hz. 4 months later, she underwent left type I thyroplasty with silastic implant and ansa cervicalis to RLN neurorrhaphy under local anesthesia with monitored anesthesia care (MAC). The patient was then discharged from the post-anesthesia care unit several hours after the procedure concluded. There were no post-operative complications. At follow up 35 days later, the patient as doing well with improved voice. GRBAS score was 2 with MPT of 10 seconds, F0 249 Hz, and range 298 Hz.
Two patients underwent the same procedure and were discharged in the early morning after overnight observation. A 58-year-old male was referred for dysphonia immediately following removal of an 8 cm anterior mediastinal mass, found to be an atypical carcinoid tumor. After more than 1 year of follow up without improvement in voice (GRBAS 12, MPT 1 second), he underwent left type I thyroplasty with laryngeal reinnervation. This was planned as an outpatient surgery, but post-operatively he was found to have a small amount of incisional crepitus, so he was admitted for overnight observation and discharged in stable condition the following morning. Most recent follow up 16 months later demonstrated improvement in voice as well as faint motion of the left vocal cord with subtle paradoxical abduction. Most recent follow up 16 months later demonstrated improvement in voice (GRBAS 3) as well as faint motion of the left vocal cord with subtle paradoxical abduction. MPT was 12 seconds, F0 166 Hz, and range 292 Hz, compared to MPT of 1 second at initial presentation.
Additionally, a 48-year-old female with a right-sided aortic arch and aberrant left subclavian artery leading to dysphagia lusoria underwent left carotid to subclavian bypass and esophageal mobilization. After surgery, she was noted to have persistent dysphonia and mild dysphagia (MPT 6 seconds). Flexible laryngoscopy demonstrated left vocal fold cord paralysis with vocal fold atrophy. She underwent injection medialization with hyaluronic acid filler, with improvement in voice. At follow up 9 months later, the effects of injection medialization had waned. She underwent left type I thyroplasty with laryngeal reinnervation and cricopharyngeal myotomy. She was admitted for overnight observation given numerous comorbidities including advanced lupus, rheumatoid arthritis, pulmonary fibrosis, and psychiatric history. She was discharged the following morning. At follow up 2 months after surgery, videostroboscopy demonstrated medialized left vocal cord, complete glottic closure, and improvement in voice and dysphagia. MPT was 10 seconds and F0 250 Hz (Figure 1). Image stills from videostroboscopy. Panel A, B, G, and H represent images of the 23-year-old female patient. Panel C, D, I, and J represent images of the 48-year-old female patient. Panel E, F, K, and L represent images of the 58-year-old male. The top row shows pre-operative open and closed glottal confirmations. The bottom row shows post-operative open and closed glottal confirmations. Post-operative closed confirmations show improved closure with less supraglottic compression.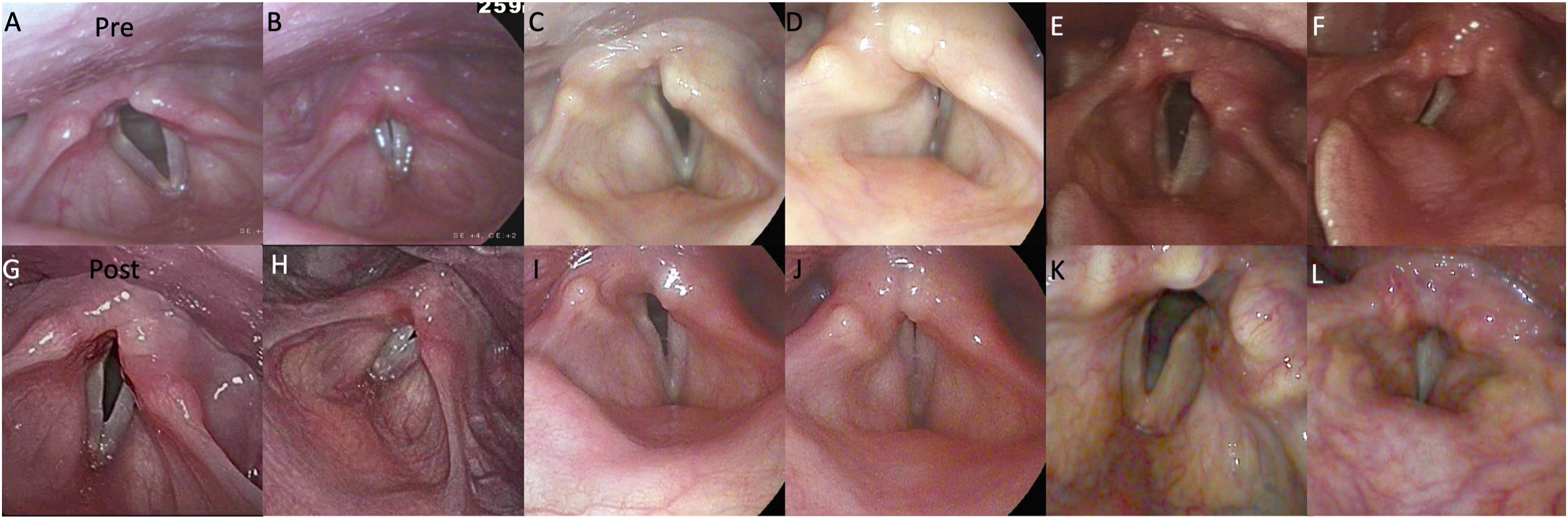
Discussion
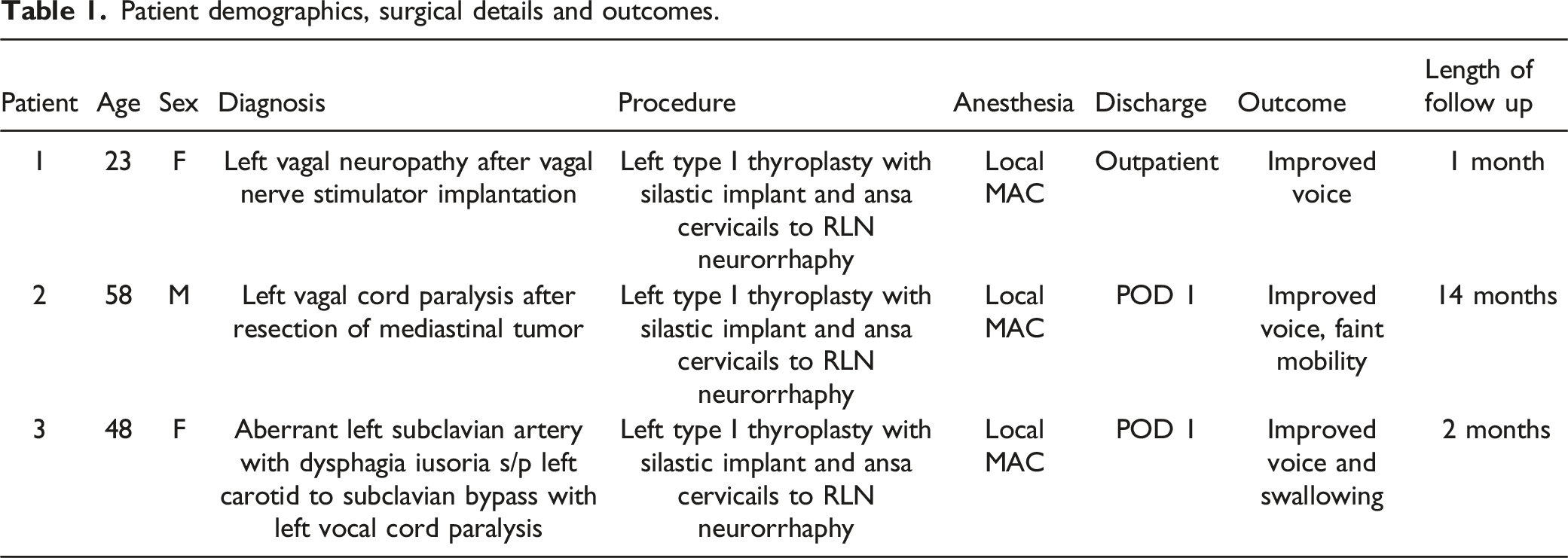
Patient demographics, surgical details and outcomes.
Given its position as an uncommon procedure that requires additional dissection adjacent to the larynx for ansa cervicalis to RLN neurorrhaphy, overnight observation is typical. Numerous reviews have established the safety of outpatient unilateral medialization laryngoplasty, and more surgeons are now comfortable with same day discharge after isolated laryngeal framework surgery in the appropriately selected patient. There are multiple advantages to outpatient surgery including lower cost, higher efficiency, and improved patient comfort. Safely converting surgeries to outpatient procedures is in line with the optimization of quality and efficiency in healthcare. The additional dissection required for laryngeal reinnervation can safely be performed under local MAC and is unlikely to significantly increase post-operative complication rates when compared to medialization laryngoplasty alone. As such, the authors believe type I thyroplasty with laryngeal reinnervation can be safely performed on an outpatient basis. Patients with significant comorbidities, bilateral laryngeal surgery, higher than expected post-operative edema or bleeding, stridor or dyspnea, crepitus, or poor support at home warrant overnight observation. Limitations of this report include the small number of patients, which limits generalizability, and limited follow up. Additionally, not all quantitative voice outcome measures were available for patients post-operatively. In the future, additional evidence regarding the safety and long-term efficacy of outpatient type I thyroplasty with laryngeal reinnervation in a larger, more diverse patient population is needed.
Conclusion
Outpatient type I thyroplasty with laryngeal reinnervation under local MAC is feasible with proper patient selection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
Meeting: This data was presented by poster at the American Laryngological Association Combined Otolaryngology Spring Meeting in April 2022.
IRB
This is a retrospective case report involving a summary of standard clinical care received by 3 patients and was declared exempt from IRB review.
Ethical statement
The authors have no ethical concerns to declare. All data is anonymous with no patient identifiers. Data was extracted by electronic medical record chart review.