
Abstract
Introduction
Inflammation plays a crucial role in carcinogenesis and the progression of neoplastic diseases, intricately modulating tumor development. Depending on the specific interactions between the tumor and the host, inflammatory cells (neutrophils and lymphocytes) can exert either pro-carcinogenic or anti-carcinogenic effects.1,2
This duality of inflammation paves the way for using inflammatory biomarkers to assess cancer risk and prognosis. Indeed, several studies have shown that inflammatory biomarkers, such as C-reactive protein, the neutrophil-to-lymphocyte ratio (NLR), and the platelet-to-lymphocyte ratio, are reliable diagnostic and prognostic predictors for certain cancers (esophageal, gastric, pancreatic, colon, ovarian, renal, and lung cancers).3,4 However, the application of these inflammatory markers in the preoperative assessment and postoperative monitoring of thyroid carcinomas, including papillary thyroid carcinoma (PTC), remains limited and controversial. 5
The objective of our study was to investigate the correlation between the preoperative NLR ratio and the clinicopathological characteristics of PTCs.
Methods
Study Type
A retrospective longitudinal study of the Ear Nose and Throat department of Charles Nicole Hospital between 2016 and 2020, including patients who underwent a total thyroidectomy.
Study Population
Inclusion criteria
Our inclusion criteria included patients aged between 18 and 90 years who underwent total thyroidectomy for papillary carcinoma or microcarcinoma (≤1.0 cm), either suspected through preoperative fine-needle aspiration or confirmed by final histopathology. Additionally, patients were required to have a white blood cell count between 4000 and 10,000 and complete preoperative data needed to be available.
Exclusion criteria
Patients presenting a concomitant pathology, which could disturb the inflammatory biological assessment, in particular: Diabetes, infection upon admission, another concomitant neoplasia, chronic inflammatory disease, system disease, renal or hepatic failure, hepatitis, and homeopathy. The use of anticoagulants, alcohol, steroidal, and nonsteroidal anti-inflammatory drugs. Patients whose data are missing.
Study Procedure
The study was conducted in the ENT department of Charles Nicole Hospital in Tunis, including patients who met the inclusion criteria. Epidemiological, clinical, Para clinical, surgical, and follow-up data were collected from the patient’s medical records. All information was documented on a pre-established datasheet specific to each patient. Thyroid nodules were classified according to the 2017 EU-TIRADS (European Thyroid Imaging Reporting and Data System) classification, and cytology was assessed following the updated 2017 version of the Bethesda System for Reporting Thyroid Cytopathology. The preoperative NLR was calculated by dividing the absolute number of neutrophils by the absolute number of lymphocytes. Based on the median NLR value, the study population was divided into 2 groups: Group 1, with NLR greater than the median value, characterized by predominant neutrophilia; and Group 2, with NLR less than the median value, characterized by relative lymphocytosis.
Statistics Methods
Continuous variables were expressed as mean ± standard deviation, while categorical variables were expressed as frequencies or percentages. Statistical analysis was performed using IBM Social Package for the Social Sciences (IBM SPSS STATISTIC) software version 26, using Student’s t test and ANOVA test for continuous variables and Kolmogorov-Smirnov in the assessment of independent groups. To analyze the correlation between the preoperative NLR and the clinicopathological characteristics of patients with PTC, we conducted a bivariate analysis followed by a multivariate logistic regression using a stepwise backward model, comparing the likelihood ratios. Statistical significance was set at P <.05.
Results
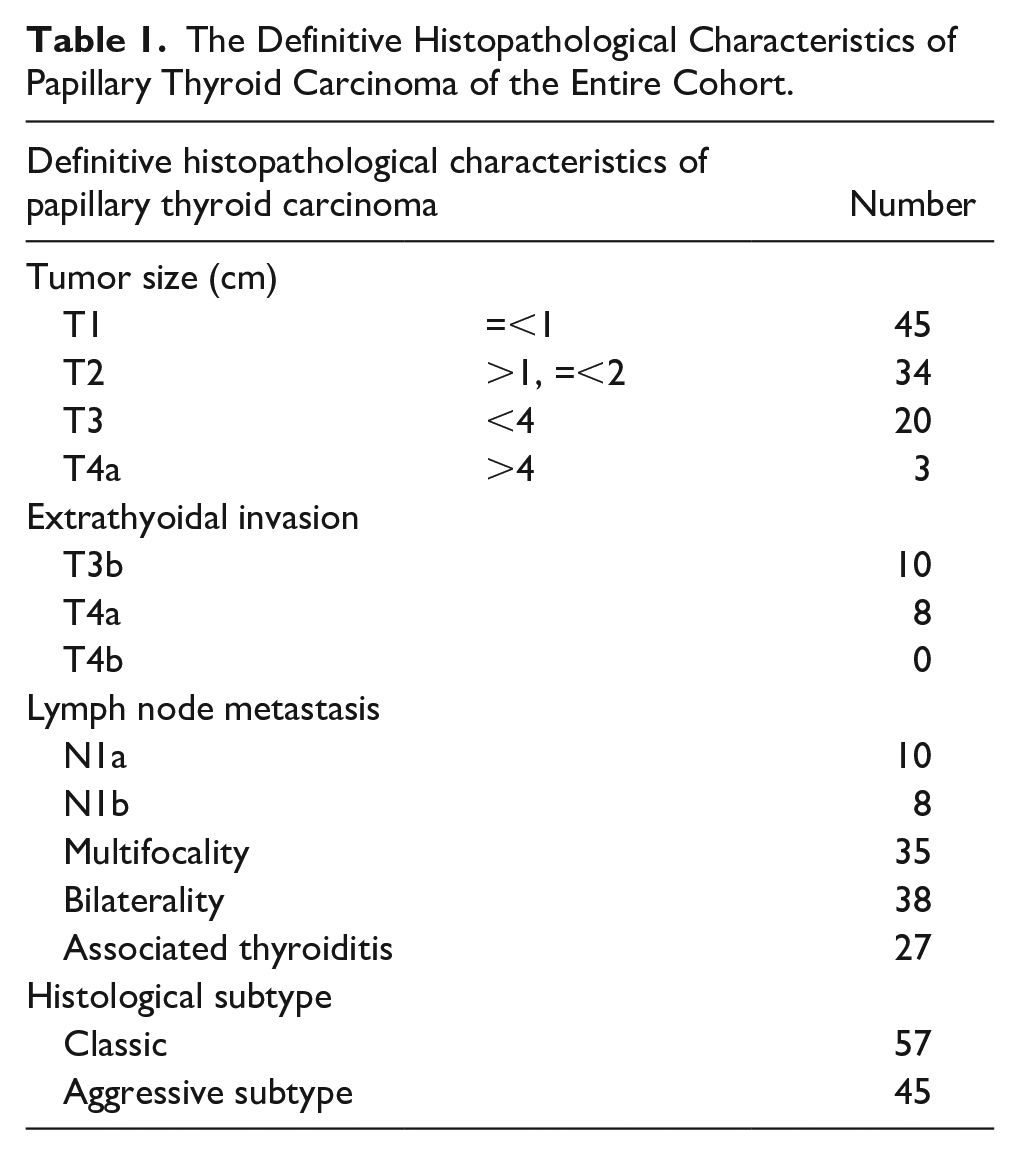
Our study included 102 patients aged 20 to 83 years, consisting of 40 men and 62 women, with a mean age of 52.09 ± 12.55 years. The study population was divided into 2 groups based on the mean NLR, with Group 1 representing patients with a high NLR. In most cases, the diagnosis was incidental. All patients were clinically and biochemically euthyroid. The mean preoperative NLR was 2.01 ± 0.62, with 53% of patients categorized into Group 1. Cervical ultrasound was performed on all patients, revealing that most nodules were classified as EU-TIRADS 5. Fine-needle aspiration was either malignant or suspicious for malignancy in 77% of cases. A total thyroidectomy, along with bilateral mediastinal and recurrent laryngeal lymph node dissection, was performed in 78% of cases. Final pathological examination revealed papillary microcarcinoma in 45 cases. PTC was multifocal in 35 cases and bilateral in 38 cases. An aggressive histological variant was noted in 45 cases. Thyroiditis was associated with carcinoma in 27 cases, and lymph node metastasis was present in 18 cases (Table 1).
The Definitive Histopathological Characteristics of Papillary Thyroid Carcinoma of the Entire Cohort.
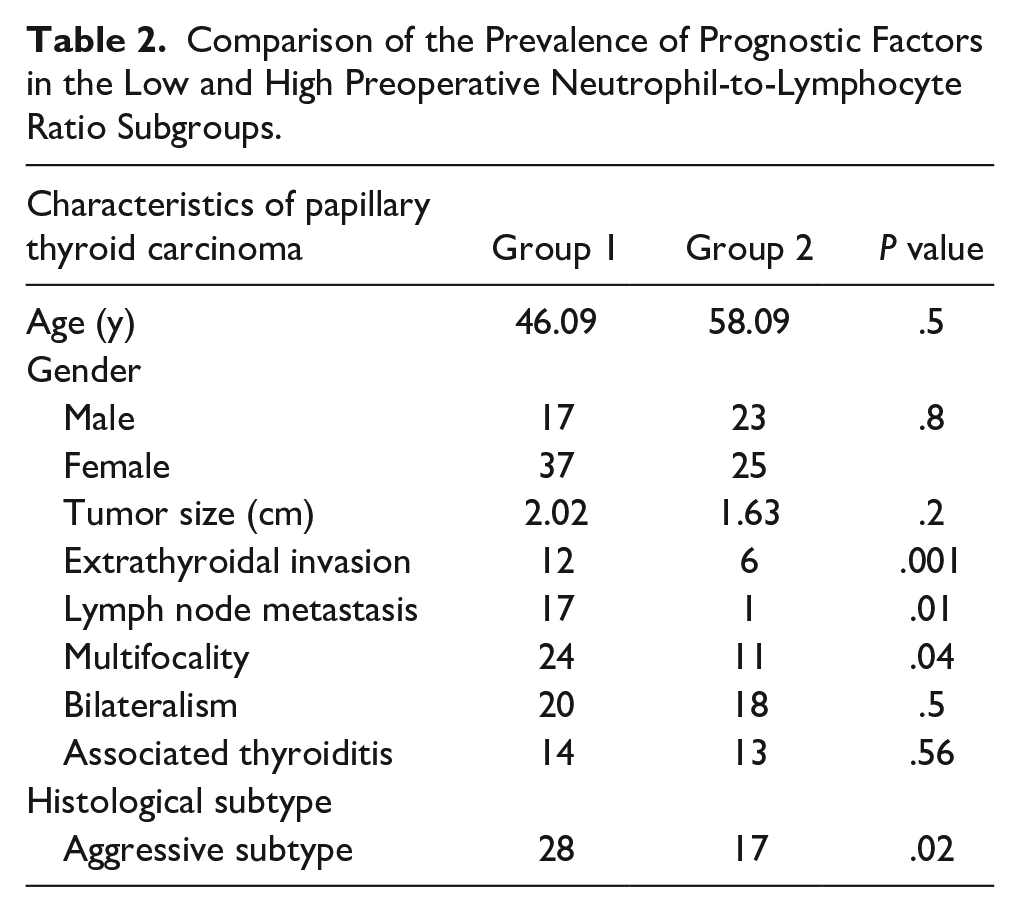
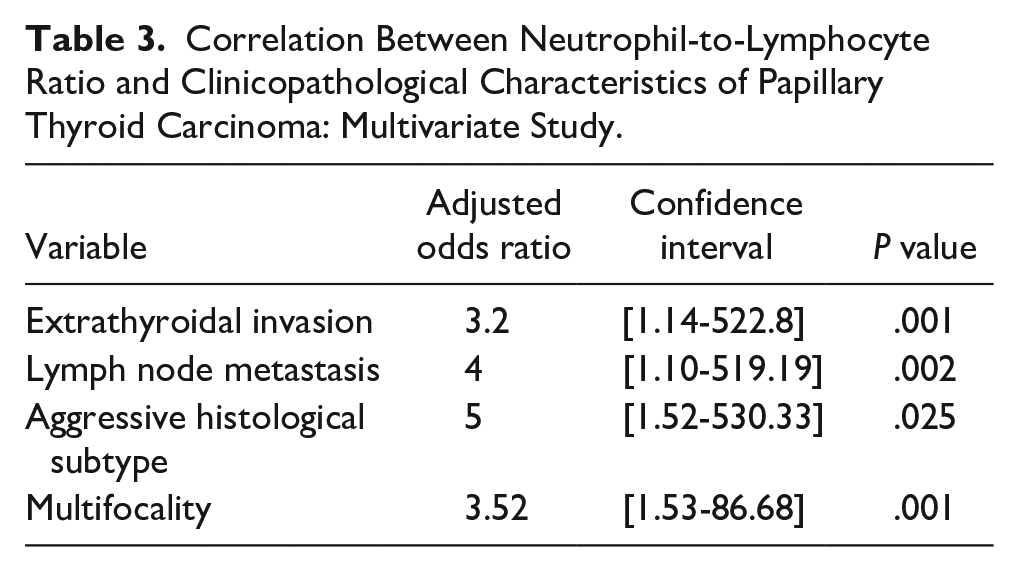
When comparing PTC characteristics between the 2 groups, no statistically significant differences were found in age and sex. However, multifocality, extrathyroidal invasion, lymph node metastasis, and aggressive variants were significantly more frequent in the high NLR group (P = .04). These findings suggest that an elevated NLR may be associated with aggressive features of PTC (Table 2). After adjusting for other variables, independent factors associated with elevated NLR included extrathyroidal invasion, lymph node metastasis, aggressive histological subtypes, and multifocality, with a 5-fold increased risk for aggressive subtypes (Table 3).
Comparison of the Prevalence of Prognostic Factors in the Low and High Preoperative Neutrophil-to-Lymphocyte Ratio Subgroups.
Correlation Between Neutrophil-to-Lymphocyte Ratio and Clinicopathological Characteristics of Papillary Thyroid Carcinoma: Multivariate Study.
Discussion
Chronic inflammation has long been recognized as a key driver of tumorigenesis in various cancers, including thyroid malignancies. It induces genetic instability and promotes uncontrolled cellular proliferation due to prolonged activation of inflammatory mediators. 6 In this study, we explored the relationship between the NLR, a biomarker of systemic inflammation, and the clinical-pathological features of PTC. Our findings provide valuable insights into the potential prognostic utility of NLR in assessing disease aggressiveness.
NLR and Hashimoto’s Thyroiditis
We noted higher NLR levels in patients with concurrent Hashimoto’s thyroiditis, though this difference did not reach statistical significance. Interestingly, prior studies by Liu et al 3 and Kocer et al 7 reported lower NLR levels in thyroiditis-associated PTC. These conflicting results may reflect the complex interplay between autoimmune thyroiditis and the molecular profile of thyroid cancer. Activation of the RET/PTC gene in Hashimoto’s thyroiditis has been implicated in promoting chronic inflammation, potentially increasing the risk of malignant transformation.8-11
NLR and Tumor Aggressiveness
One of the most significant findings of our study was the strong association between elevated NLR and aggressive variants of PTC. Patients with high NLR had a fivefold increased likelihood of harboring aggressive tumor subtypes. These results align with previous studies by Zhang et al 2 and Oba et al, 12 which demonstrated that elevated preoperative NLR is linked to higher rates of local recurrence and distant metastasis in aggressive histological variants. Our data suggest that high NLR reflects a proinflammatory and immunosuppressive tumor microenvironment that fosters tumor progression.
Lack of Association with Tumor Size and Bilaterality
While tumor size and bilaterality are important clinical markers, our study did not find statistically significant associations between these parameters and NLR. This aligns with the findings of Lang et al 13 and Cho et al, 14 who also reported no correlation between NLR and tumor size or bilaterality in PTC. In contrast, Ecin et al 9 observed elevated NLR levels in tumors exceeding 2 cm. The variability in these findings may be attributed to differences in study populations and methodological approaches.
NLR and Extrathyroidal Extension
Extrathyroidal invasion is a poor prognostic factor in PTC, often associated with an increased risk of recurrence.15,16 An elevated NLR indicates a reduced number of cytotoxic T lymphocytes, which are responsible for the antitumor response. This immune situation could facilitate the extension beyond the thyroid gland.8,10 Manatakis et al, in a series of 205 patients with PTC, concluded a significant association between a high NLR and the presence of extrathyroidal extension. 8 Similarly, in our study, the link between NLR and extrathyroidal invasion was significant, with a high NLR increasing the risk of extension by 3 times. These results support the hypothesis that NLR could be a promising preoperative biomarker for identifying aggressive forms of PTC. However, other authors, such as Liu et al 3 and Kim et al, 17 did not find a significant link between NLR and extrathyroidal extension, this underscores the need for further investigation with larger and more homogeneous samples.
NLR and Lymph Node Metastases
Lymph node involvement in PTC is often associated with a more pronounced inflammatory response. An elevated NLR could reflect an increased systemic inflammatory state, indicating an environment more conducive to lymph node metastasis formation.8,18 Our study revealed a statistically significant association between a high NLR and the presence of lymph node metastases. A high NLR increases the risk of lymph node involvement by 4 times. These results are consistent with the series by Gang et al, which also found that patients with a high NLR were more likely to have lymph node metastases compared to those with a lower NLR. 19 However, results are not always uniform. Some studies did not find a significant link between NLR and lymph node metastases in PTC.17,19,20 This may be due to methodological variations, sample size differences, or the heterogeneous nature of the studies.8,17
Clinical Implications
Our study highlights the clinical relevance of NLR as a potential preoperative biomarker for identifying high-risk PTC patients. Elevated NLR was significantly associated with aggressive tumor features, including extrathyroidal invasion and lymph node metastases. These findings support the integration of NLR into routine preoperative risk stratification protocols, aiding in the early identification of patients who may benefit from more aggressive management strategies.
Limitations and Future Directions
While our findings are compelling, the study is limited by its retrospective design and relatively small sample size. Larger, prospective studies are needed to validate the prognostic utility of NLR in thyroid cancer and to further elucidate the mechanisms underlying its associations with tumor aggressiveness.
Conclusion
The NLR, as a preoperative biomarker, offers the advantages of simplicity, easy accessibility, and cost-effectiveness for evaluating the aggressiveness of PTC. Its use could enhance patient stratification based on risk, enabling more personalized therapeutic strategies. Increased monitoring may be warranted in patients with elevated NLR, while a more conservative surgical approach could be considered for those with low NLR, depending on their tumor characteristics. However, larger, multicenter prospective studies are needed to confirm NLR as a reliable predictive biomarker. Additionally, assessing NLR dynamics both pre- and postoperatively could provide further insights into its long-term prognostic value and help refine clinical decision-making.
Footnotes
Author Contributions
C.B.A.: writing – original draft. M.T.: writing – review & editing. I.R.: writing – review & editing. M.B.: supervision.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This is a retrospective observational study. The Research Ethics Committee of our university hospital has confirmed that no ethical approval was required. Archival patient’s data were anonymized.