
Abstract
Objective
This study aimed to assess the association of the neutrophil-to-lymphocyte ratio (NLR) with the occurrence of venous thromboembolism (VTE) and arterial thrombosis (AT).
Methods
This was a retrospective cross-sectional study including 585 medical records obtained from all consecutive patients who were suspected of having thrombosis.
Results
The AT group had a higher neutrophil count and NLR and a lower lymphocyte count than the non-thrombosis group. Receiver operating characteristic curve analysis showed the ability of the NLR to predict the presence of AT. The cut-off value for the NLR was 4.44. No distinction was found in the NLR between the VTE and non-thrombosis groups. Regression analysis showed that a high NLR was an independent factor related to the presence of AT. Patients with an NLR ≥ 4.44 had a higher risk of AT than those with an NLR < 4.44 (odds ratio = 2.015, 95% confidence interval: 1.180–3.443).
Conclusion
A high NLR may be considered a predictive factor for the occurrence of AT, but an association with the presence of VTE was not found.
Keywords
Introduction
Thrombosis, including venous thromboembolism (VTE) and arterial thrombosis (AT), is a disease with a high mortality and morbidity rate. Myocardial infarction and thrombotic stroke are the main types of AT and are the most common causes of morbidity and mortality. VTE, including deep venous thrombosis (DVT) and pulmonary embolism (PE), is also the most common vascular disease after acute myocardial infarction and thrombotic stroke. 1 In the 19th century, Rudolph Virchow experimentally showed that the development of thrombosis may be caused by damage to the blood vessels, irritation of the surrounding area, blood coagulation, and interruption of blood flow. His thesis formed Virchow’s triad, which was considered the mechanism of VTE and included endothelial injury, hypercoagulability, and stasis. 2 In contrast, because of the strong flow in the arterial system, coagulation factors do not play a major role in AT. Vessel wall damage (atheroschlerosis, hypertension, vascular anomalies) is considered a major risk factor for AT. This damage allows platelets to easily adhere and aggregate. Thus, platelet hyperactivity plays a role in the pathogenesis of AT.3,4
Currently, the combination of stasis and hypercoagulability is considered crucial to the occurrence of VTE, while endothelial damage and platelets play a role in the development of atherosclerosis and AT. Atherosclerosis is a chronic inflammatory disease; therefore, the role of inflammation in the pathogenesis of AT has been better studied than that in VTE.5–7 Therefore, the neutrophil count and neutrophil-to-lymphocyte ratio (NLR), which are considered indicators of inflammation, would theoretically be associated with AT rather than VTE.1,8 However, inflammation has been gradually accepted as a mechanism of thrombus formation in the veins. Inflammation of the vein wall triggers the coagulation system through the induction of tissue factor.7,9,10 Furthermore, recent studies have demonstrated the role of neutrophils in both VTE and AT through activation of neutrophil extracellular traps (NETs). NETs activate factor XII and increase tissue factor production, leading to activation of the intrinsic and extrinsic pathways, thus augmenting VTE. Some mouse model studies have demonstrated the role of NETs in VTE; however, clinical evidence is sparse.11–14 Although the mechanism of NETs that contributes to VTE has been established, its activation in AT has not been investigated. 11 Several mouse model studies have indicated that NETs play a role in atherosclerosis.15–17 Other clinical observational studies also confirmed that NETosis (the process during which neutrophils undergo programmed cell death and release NET) is associated with greater severity and the extent of coronary artery disease.18,19
The NLR is a simple indicator related to inflammation, as well as NETs, and can be used to study VTE and AT. Although mouse model studies on the role of neutrophils and NETs in thrombosis exist, clinical evidence is lacking. Clinical studies have not satisfactorily determined the value of the NLR in relation to VTE. However, clinical studies on the value of the NLR in AT have mainly focused on coronary artery disease.20–24 Therefore, we conducted this study to assess the association of the NLR with the occurrence of VTE and AT.
Materials and methods
Medical records
This was a retrospective cross-sectional study. Medical data were obtained from all consecutive patients who were suspected of having thrombosis at Bach Mai Hospital, Hanoi, Vietnam, from January to December 2021. Patients with previously diagnosed thrombosis were excluded. The patients were divided into three groups. Group 1 included patients with newly diagnosed VTE. Group 2 included patients with newly diagnosed AT. Group 3 included patients who were not confirmed to have thrombosis. The determination of thrombosis was performed by computed tomography scans, magnetic resonance imaging, or Doppler ultrasound. The Institutional Review Board of Hanoi Medical University waived the need for approval and patient consent because of the retrospective observational nature of the study and because all information was obtained from medical records. All patient details were deidentified.
Collected data
Peripheral blood cell indices including the hemoglobin level and white blood cell, neutrophil, lymphocyte, monocyte, and platelet counts were collected before starting treatment. Biomarkers such as fibrinogen and D dimer were also collected. Data on comorbidities, risk factors, and status, including smoking, overweight, contraception, immobility, cardiovascular disease, postoperative care, cancer, antiphospholipid syndrome, infections, diabetes, and dyslipidemia, were also collected.
Statistical analysis
Differences were compared between two groups: VTE vs. non-thrombosis and AT vs. non-thrombosis. Qualitative variables (sex, smoking, overweight, contraception, immobility, cardiovascular disease, postoperative care, cancer, antiphospholipid syndrome, infections, diabetes, and dyslipidemia) were analyzed using the χ2 or Fisher’s test. Quantitative variables (hemoglobin level; white blood cell, neutrophil, lymphocyte, monocyte, and platelet counts; NLR, and fibrinogen and D dimer levels) were analyzed using an independent samples T-test or Mann–Whitney test according to their normal or nonnormal distribution. Quantitative variables were also compared between the thrombosis group (VTE + AT) and the non-thrombosis group, among the VTE subgroups (including DVT, PE, and other VTE), and between the AT subgroups (including thrombotic stroke and other AT). Data for three subgroups were analyzed using one-way analysis of variance for parametric data or the Kruskal–Wallis test for nonparametric data.
Receiver operating characteristic (ROC) curve analysis was performed to assess the ability of the NLR to predict the occurrence of thrombosis (VTE and AT). Regression analysis was used to examine the relationship between the cut-off value and the presence of thrombosis (VTE and AT). A value of P < 0.05 was considered statistically significant. The bias was controlled because no patient medical records were lost.
The study reporting conformed to the STROBE guideline. 25
Results
Patient characteristics
This retrospective study included medical records of 363 patients with thrombosis including 281 VTE patients (group 1), 82 AT patients (group 2), and 222 patients without thrombosis (group 3). The median ages of groups 1, 2, and 3 were 45, 46, and 41 years, respectively. There was a significant difference in age between the VTE and non-thrombosis group and between the AT and non-thrombosis group (P = 0.039 and 0.012, respectively).
Table 1 shows that patients 45 years or older had a higher rate of thrombosis (VTE or AT) than patients under 45 years of age (P = 0.002, 0001, respectively). The proportion of women in the VTE group was higher than that in the non-thrombosis group (P = 0.002). However, no significant differences were found in the comorbidities, risk factors, or status, including smoking, overweight, contraception, immobility, cardiovascular disease, postoperative care, cancer, antiphospholipid syndrome, infections, diabetes, and dyslipidemia, among the VTE, AT, and non-thrombosis groups (Table 1).
Comorbidities, risk factors, and status of patients.

Note: P1: between the venous thromboembolism and non-thrombosis groups.
P2: between the arterial thrombosis and non-thrombosis groups.
The location and type of thrombosis are presented in Table 2. The VTE subgroups included DVT, PE, and other thrombosis, in which the rate of DVT in the lower extremities was highest (41.0%). The AT subgroups included thrombotic stroke and other thrombosis, in which the rates of thrombotic stroke and AT in the lower extremities were highest (both 20.8%).
Location of thrombosis.

Table 3 shows that the AT group had a higher neutrophil count and NLR and a lower lymphocyte count (P < 0.05) than the non-thrombosis group. However, these differences were not observed when comparing the VTE group with the non-thrombosis group and the thrombosis (VTE + AT) group with the non-thrombosis group. The D dimer and fibrinogen levels in the AT group and the thrombosis group (VTE + AT) were significantly higher than that in the non-thrombosis group (P < 0.05). A significant difference was only observed in the D dimer index when comparing the VTE group with the non-thrombosis group (P = 0.041).
Peripheral blood cell and biomarker indices.

VTE, venous thromboembolism; AT, arterial thrombosis; SD, standard deviation; WBCs, white blood cells, NLR, neutrophil-to-lymphocyte ratio; FEU, fibrinogen equivalent units.
Note: P1: between the VTE and non-thrombosis groups.
P2: between the AT and non-thrombosis groups.
P3: between the thrombosis (including VTE and AT) and non-thrombosis groups.
The results also indicate that there were no differences among the VTE subgroups or between the AT subgroups when comparing the laboratory indices, except for the hemoglobin level (P < 0.001 for the VTE subgroups) and monocyte count (P < 0.001 for the AT subgroups) (Table 4).
Peripheral blood cell and biomarker indices according to the type of VTE or AT.

VTE, venous thromboembolism; AT, arterial thrombosis; SD, standard deviation; WBCs, white blood cells, NLR, neutrophil-to-lymphocyte ratio; FEU, fibrinogen equivalent units; DVT, deep venous thrombosis; PE, pulmonary embolism; TS, thrombotic stroke.
Note: P1: among the VTE, PE, and other VTE groups.
P2: between the TS and other AT groups.
ROC curve analysis for the NLR
ROC curve analysis showed the ability of the NLR to predict the presence of AT. The area under the curve for the NLR was 64.1% with P < 0.001 (Figure 1, Table 5). Based on the sensitivity and specificity analysis, the cut-off value of the NLR was determined to be 4.44 (Table 5). However, this analysis did not indicate an NLR value that could distinguish VTE from non-thrombosis.

Receiver operating characteristic curve analysis of the ability of the neutrophil-to-lymphocyte ratio to distinguish between the arterial thrombosis and non-thrombosis groups.
Receiver operating characteristic curve analysis of the ability of the neutrophil-to-lymphocyte ratio to predict the presence of arterial thrombosis.
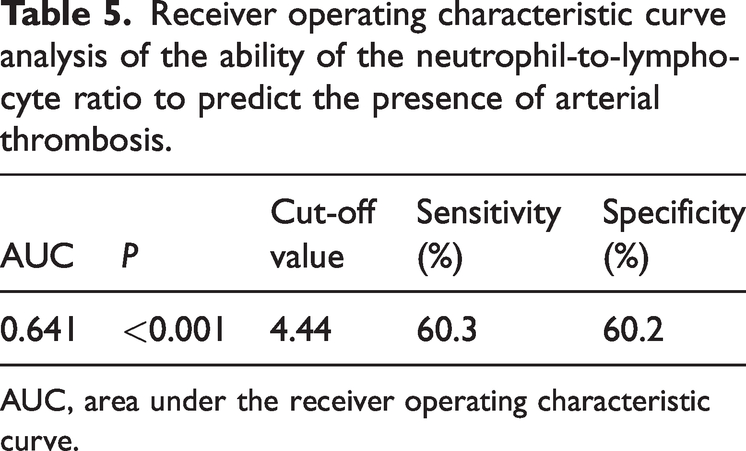
AUC, area under the receiver operating characteristic curve.
Regression analysis of the NLR
The regression analysis showed that a high NLR (≥4.44) and older age (≥45 years) were independent factors related to the presence of AT (Table 6). Patients with a high NLR (≥4.44) had a higher risk of AT than those with an NLR < 4.44 (odds ratio = 2.015, 95% confidence interval: 1.180–3.443, P = 0.01).
Association of the NLR with VTE and AT.

VTE, venous thromboembolism; AT, arterial thrombosis; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; CI, confidence interval.
The regression analysis also indicated that older age (≥45 years) and sex (female) were independent factors related to the presence of VTE (Table 6).
Discussion
Mouse model studies have shown the role of inflammation and NETs in both VTE and AT. Although the NLR is considered a biomarker of inflammation, whether the NLR is a simple index that represents inflammation or NETs in relation to VTE and AT and the scope of its clinical application are unknown. These questions require further research.
Clinical observational studies have shown differing results. Cavuş et al. and Köse et al. suggested that the NLR is an independent prognostic factor for pulmonary embolism.26,27 Zhao et al. also indicated that the NLR can be used as a marker to predict outcomes in patients after cerebral venous thrombosis treatment. 28 However, the more interesting value of the NLR is whether it can be considered a diagnostic marker or predictor of the occurrence of VTE. Grimnes et al. determined that the NLR was not associated with the risk of first time or recurrent VTE. 20 Artoni et al. also suggested that a high NLR was not related to an increased risk of VTE. 21 In contrast, Rinaldi et al. and Hu et al. found that a high NLR can be considered a diagnostic marker for VTE.22,29 Additionally, Farah et al. claimed that a high NLR could be a predictor of acute VTE. 30 Some studies indicated that a high NLR may be a trigger that increases the risk of VTE in comorbidity. Studies by Carobbio et al., including patients with polycythemia vera, and Peng et al., including patients after oral cancer surgery, indicated that a high NLR can increase the risk of VTE.31,32 However, Yao et al. and Niu et al. did not find this association in patients after total joint arthroplasty or after femoral neck fractures.33,34 Similar to Grimnes et al. and Artoni et al., our study did not find an association between a high NLR and the occurrence of VTE. In our study, only older age (≥45 years) and sex (female) were related to the presence of VTE. Furthermore, no differences were found among the VTE subgroups (DVT, PE, and other VTE), with the exception of the hemoglobin level. Some studies have indicated that a high hemoglobin level is a risk factor for VTE; however, no study has shown a difference between VTE subgroups.35–37 In general, studies on the value of a high NLR in increasing the risk of VTE are controversial. There is still a long distance from mouse model study results to their clinical application.
Unlike in patients with VTE, a high NLR was closely associated with the occurrence of AT. Our study showed that patients with AT had a higher NLR than patients without thrombosis (P < 0.05). Multivariate regression analysis showed that patients with a high NLR (4.44) had a 2-fold higher risk of AT than those with an NLR < 4.44. Mouse model studies of Lee et al. and Cha et al. determined that leukocytosis and neutrophilia play a role in the development of AT.38,39 Laridan et al. analyzed thrombi from ischemic stroke patients and suggested that neutrophils and NETs are important constituents of cerebral thrombi. 40 Several clinical observational studies have also supported that a high NLR is associated with AT; however, these studies were associated with coronary artery disease. Sönmez et al. and Kaya et al. showed that a high NLR (2.3 to 2.6) was considered an independent factor in the severity prognosis of patients with coronary artery disease. Kaya et al. also indicated that a high NLR is a predictor of severe atherosclerosis.23,24 Papa et al. suggested that the NLR is an independent predictor of cardiac death. 41 These results focused on the prognostic value of the NLR. More importantly, Angkananard et al. assumed that the NLR may be a useful biomarker of cardiovascular disease; therefore, it should be examined when assessing cardiovascular risk in the population. 42 Moreover, in a rare study of other arteries, Chung et al. suggested that this association depended on the type of artery. This study indicated that a high NLR is related to a large cerebral artery with atherosclerosis, but it is not related to a small cerebral vessel. 43 However, the formation of thrombosis is related to many factors. Unfortunately, in our study, the arteries were not grouped according to size. However, when comparing between thrombotic stroke and other AT, no differences were found, except for the monocyte count. Monocytes can contribute to the development of thrombosis because of the release of pro-inflammatory cytokines, and they can interact with platelets and endothelial cells. The role of monocytes in the pathogenesis of thrombosis is recognized; however, few studies have focused on the differences between AT subgroups. 44
Inflammation and NETs have been associated with thrombosis (VTE and AT). Studies were carried out to examine whether a high NLR may be a predictor of thrombosis. However, it is not yet possible to confirm whether the activity of NETs correlates with a high NLR. Additional research is needed to answer this question.
Our study also showed that D dimer levels in the AT, VTE, and thrombosis groups were higher than that in the non-thrombosis group (P < 0.05). D dimer is a fibrin degradation product and is an important marker for the diagnosis of thrombosis, such as PE. However, for the purpose of this study, we do not discuss this topic.
Limitations of our study
The sample size of the AT group was small, less than one-third of that of the VTE group and the non-thrombosis group. This was a cross-sectional study; therefore, the non-thrombosis group was not followed up. We were unable to assess whether progression of thrombosis occurred in this group.
Conclusion
Our study indicates that the NLR is associated with the occurrence of AT. A high NLR may increase the risk of AT. This significance was not found for VTE. The value of the NLR in thrombosis remains an open question. Additional research is needed to determine how this index can be used effectively, its purpose (diagnosis, prediction, prognosis, indication of treatment), and the type of thrombosis (VTE, AT, type of artery) for which it can be used.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241240999 - Supplemental material for Association of the neutrophil-to-lymphocyte ratio with the occurrence of venous thromboembolism and arterial thrombosis
Supplemental material, sj-pdf-1-imr-10.1177_03000605241240999 for Association of the neutrophil-to-lymphocyte ratio with the occurrence of venous thromboembolism and arterial thrombosis by Ha Thanh Nguyen, Minh Phuong Vu, Thi Tuyet Mai Nguyen, Tuan Tung Nguyen, Thi Van Oanh Kieu, Hai Yen Duong, Phuong Thao Pham and Thi Hue Hoang in Journal of International Medical Research
Footnotes
Acknowledgements
The authors thank all technicians of the Morpho-histological Lab, Hematology and Blood Transfusion Center, Bach Mai Hospital, for their efforts in supporting this research.
Author contributions
Ha Thanh Nguyen: Data curation, Formal analysis, Methodology, Writing; Minh Phuong Vu: Conceptualization, Data curation, Formal analysis, Methodology, Writing; Thi Tuyet Mai Nguyen: Data curation, Formal analysis, Investigation, Writing; Tuan Tung Nguyen: Formal analysis, Methodology, Writing; Thi Van Oanh Kieu: Formal analysis, Investigation, Writing; Hai Yen Duong: Formal analysis, Investigation, Writing; Phuong Thao Pham: Formal analysis, Investigation, Writing; Thi Hue Hoang: Formal analysis, Investigation, Writing. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.