
Abstract
Objective:
The purpose of this study was to demonstrate the prognostic role of inflammatory biomarkers in patients with laryngeal squamous cell carcinoma.
Methods:
For this study, we enrolled 151 patients who had undergone surgery for laryngeal squamous cell carcinoma. We assessed the preoperative neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), monocyte to lymphocyte ratio (MLR), mean platelet volume, red cell distribution width, and alkaline phosphatase. The chi-square test, Kaplan-Meier survival analysis, and Cox proportional hazards model were conducted on overall survival, progression-free survival, locoregional recurrence-free survival, and distant metastasis-free survival of patients with laryngeal squamous cell carcinoma.
Results:
Both Kaplan-Meier analysis and univariate analysis showed significant prognostic differences with age, laryngectomy methods, Tumor Node Metastasis (TNM) staging, tumor location, NLR, PLR, MLR, and mean platelet volume. Multivariate analysis indicated that NLR (overall survival: hazard ratio [HR] = 3.02, 95% confidence interval [CI]: 1.28-7.10, P = .011), PLR (overall survival: HR = 0.33, 95% CI: 0.14-0.78, P = .011; progression-free survival: HR = 0.016,95% CI: 0.10-0.79, P = .016), and MLR (overall survival: HR = 0.29, 95% CI: 0.11-0.76, P = .012) were independent prognostic factors for 5-year survival. However, red cell distribution width and alkaline phosphatase had no significant difference in overall survival and progression-free survival.
Conclusions:
Preoperative high NLR, PLR, and MLR were associated with poor prognosis. They were found to be effective and reliable inflammatory biomarkers for patients with laryngeal squamous cell carcinoma.
Keywords
Introduction
Laryngeal squamous cell carcinoma (LSCC) is one of the most common head and neck malignancies with poor prognosis. Its 5-year survival rate is approximately 75% in patients with localized disease, 44% in patients with regional disease, and 35% in patients with distant disease. 1 When there is regional or distant metastasis, the 5-year survival rate drops significantly. Laryngeal squamous cell carcinoma accounts for 85% to 95% of all laryngeal carcinomas, and the age of onset for this disease is now earlier than it was in the past. 2 Therefore, it is appropriate to urgently find effective and reliable biomarkers that will help in predicting the prognosis of LSCC, the possibility of recurrence, and the nature of distant metastasis. Laryngeal carcinogenesis is a multifactorial process that has not been fully elucidated. Preoperative inflammatory biomarkers have been widely studied in recent clinical literature probably because of their characteristics, which include easy access, low cost, high specificity, and high sensitivity. A high neutrophil to lymphocyte ratio (NLR) reflects systemic inflammation and poor prognosis for several types of cancer. It is indicative of early recurrence, tumor aggressiveness, distant metastasis, and death. 3 Platelets can form platelets–tumor cell complexes that protect tumor cells from immune responses and contribute to tumor cell proliferation and metastasis. 4 Therefore, platelet to lymphocyte ratio (PLR) and mean platelet volume (MPV) were also widely used to predict the survival outcome of patients with LSCC. The combined action of the tumor infiltrating neutrophils (TINs) and tumor-associated macrophages (TAMs) produces interleukin 6 (IL-6) and granulocyte colony-stimulating factor (GCSF) to stimulate tumor cell proliferation, metastasis, and angiogenesis. 5–6 The TAMs were derived from peripheral blood monocytes (PBM). The monocyte to lymphocyte ratio (MLR) was also demonstrated to have prognostic function in patients with LSCC. Red cell distribution width (RDW) was increased in several cancers. The RDW represents the degree of heterogeneity of the erythrocyte volume. A high alkaline phosphatase (ALP) was often found in liver lesions or bone metastatic tumors and was found to be prognostically relevant in several solid tumors. 7,8 Complete blood count (CBC) is a routine preoperative examination done within a week prior to biopsy or surgical intervention. It helps assess surgical risks, including the quantities of leukocytes, lymphocytes, neutrophils, and platelets as well as the MPV, RDW, NLR, PLR, or MLR. Hence, we purposed to investigate and compare the prognostic value of preoperative inflammatory biomarkers (NLR, PLR, MLR, MPV, RDW, and ALP) on overall survival (OS) and progression-free survival (PFS) in patients with LSCC having different tumor sizes and stages in this study.
Materials and Methods
Patient Characteristics
In this retrospective study, we enrolled a total of 151 patients who were diagnosed with LSCC in the Clinical Medical College, Yangzhou University (Jiangsu, China) from April 2008 to March 2014. We excluded certain patients from our study based on the following criteria: (1) patients who had concurrent acute inflammatory diseases. (2) Patients who had hematological, rheumatoid, or immune system disorders as well as renal insufficiency. These disorders potentially affect the levels of inflammatory biomarkers. (3) Patients with incomplete clinical information. (4) Patients whose follow-up period was less than 5 years. (5) Patients who had undergone laryngectomy after chemoradiotherapy. We obtained patients data on demographics, laboratory tests, imaging reports, and histopathology from electronic medical records. We then gathered and calculated parameters of CBC within a week before the biopsy or surgical excision. Additional parameters that were gathered included NLR, PLR, MLR, MPV, RDW, and ALP. The TNM stages of patients with LSCC were determined according to the criteria of the 8th edition of American Joint Committee on Cancer. After partial or total laryngectomy, the patients were routinely reviewed for imaging as well as both physical and laboratory examinations. The patients were on follow-up via telephone until March 2019 or their death.
Statistical Analysis
The study population was divided into 3 groups based on preoperative NLR, PLR, and MLR values that were evaluated by chi-square test and dichotomized according to cutoff values. All statistical analysis was performed using SPSS version 21.0. We calculated the optimal cutoff values of NLR, PLR, MLR, MPV, RDW, and ALP based on maximum Youden index (sensitivity + specificity − 1) through receiver–operating curve (ROC) analysis. Survival analysis was performed by Kaplan-Meier analysis, and variables were compared using log-rank test. Both univariate and multivariate analyses used the Cox proportional hazards model in order to explore the association between inflammatory biomarkers and survival outcomes. The significance was set at P < .05, and the results were expressed as hazard ratios (HRs) with 95% confidence interval (CI). In addition, 2 end points (5 years: OS and PFS) were selected to evaluate the survival outcome of patients with LSCC.
Results
Optimal Cutoff Values of Inflammatory Biomarkers
According to ROC analysis, the optimal cutoff values of preoperative NLR, PLR, MLR, MPV, RDW, and ALP were 2.2, 106, 0.18, 10.8, 12.8, and 79.5 (U/L), respectively. The areas under the curve (AUCs; 95% confidence interval [CI]) were 0.780 (0.718-0.843, P < .001) for NLR, 0.926 (0.889-0.962, P = .001) for PLR, 0.654 (0.584-0.724, P < .001) for MLR, 0.810 (0.757-0.863, P = .004) for MPV, 0.784 (0.727-0.841, P = .006) for RDW, and 0.688 (0.623-0.753, P < .001) for ALP. We found that there were statistically significant differences to evaluate the prognostic value of these inflammatory biomarkers.
Clinicopathologic Characteristics of Study Population
The entire cohort (N = 151) was composed of 147 males (97.3%) and 4 females (2.6%) with median age of 65 years (range: 44-84). The histopathologic cancer type for all patients was LSCC. There were 67 patients who had comorbidities. In all, 39, 14, and 5 patients had hypertension, diabetes, and coronary heart disease, respectively. In addition, 5, 3, and 1 patients had hepatitis B, phthisic, and typhoid fever, respectively. The descriptive statistics of patient about clinical, histopathological, and treatment characteristics is presented in Table 1. The tumor location between high NLR and low NLR was found to have statistically significant differences. Moreover, higher level of NLR, PLR, and MLR was associated with worse T-stage, N-stage, and advanced TNM stage. Similarly, NLR, PLR, and MLR were highly correlated with the surgical method (Table 1).
Relevant Between Preoperative NLR, PLR, MLR, and Clinicopathological Characteristics of Patients.
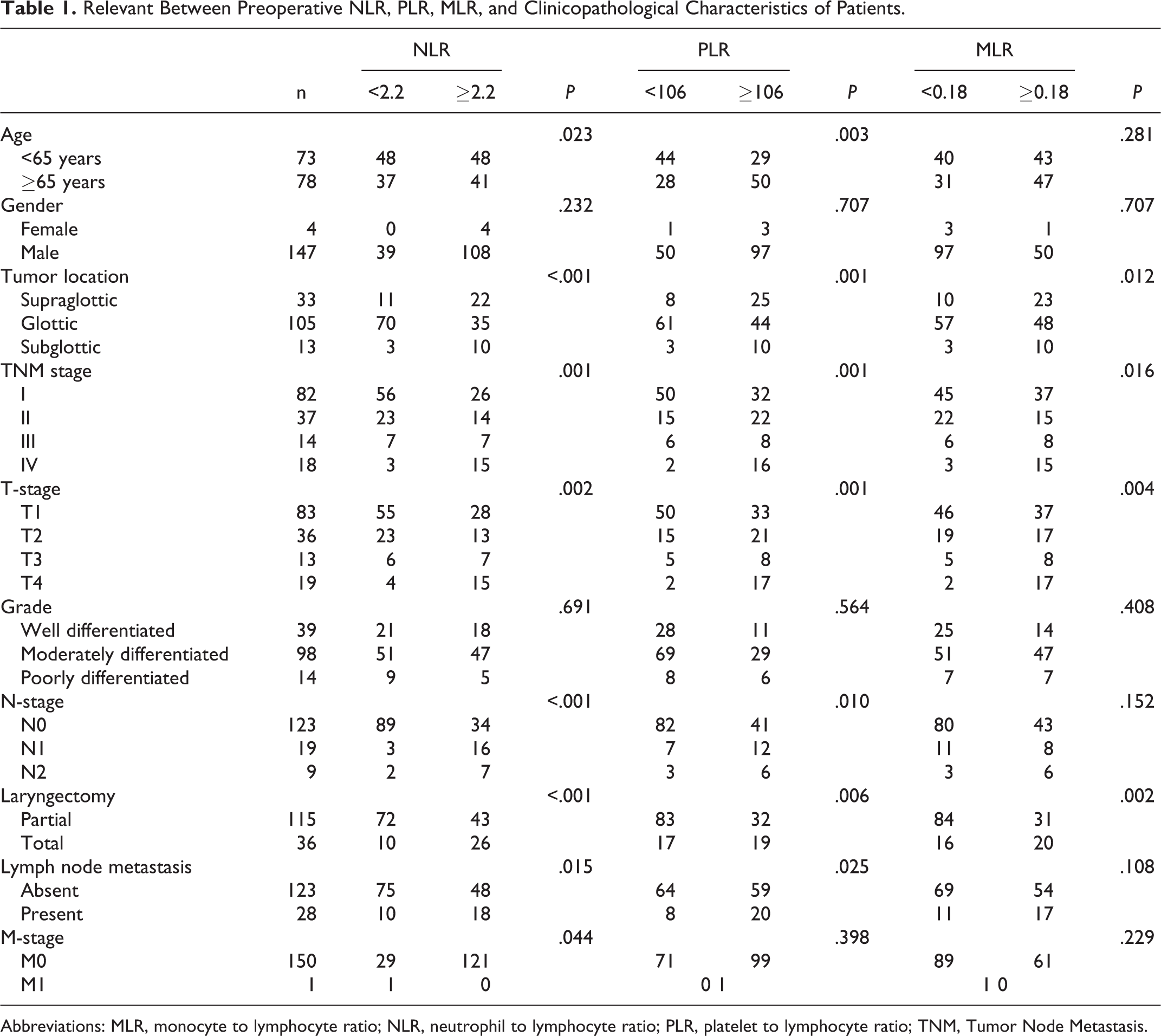
Abbreviations: MLR, monocyte to lymphocyte ratio; NLR, neutrophil to lymphocyte ratio; PLR, platelet to lymphocyte ratio; TNM, Tumor Node Metastasis.
The Prognostic Value of Inflammatory Biomarkers on Univariate Analysis
Five-year OS and PFS of patients with LSCC were 65.1% and 66.4%, respectively. In the NLR <2.2 and NLR ≥2.2 groups, 5-year OS: 83.5% vs 57.5%, P < .001 and PFS: 87% vs 59%, P < .001, which revealed high NLR had significantly poor survival outcome. The difference was statistically significant between PLR <106 and PLR ≥106; 5-year OS; 90.2% vs 56.9%, P < .001; PFS: 93% vs 56.9%, P < .001. Similarly, patients with high MLR values ≥0.18 had a poor prognostic outcome when compared to MLR <0.18 (Table 2; Figure 1). In univariate analysis, the patient’s age and laryngectomy methods were found to be statistically significant between OS and PFS. The 5-year OS and PFS were 0.45 (0.26-0.78, P = .004) and 0.50 (0.29-0.84, P = .010) for age-groups, respectively. The TNM stages and tumor location supported significant predictive values for OS and PFS in Table 2. In addition, there were no significant differences between low and high RDW values that were determined for 5 year OS (P = .892) and PFS (P = .948). Similarly, no statistically significant differences were observed for 5-year OS and PFS according to ALP values (P = .663, and .889, respectively). The result showed that preoperative high NLR, PLR, MLR, and MPV were associated with poor prognosis. The patient’s age, methods used for laryngectomy, the TNM stages, and tumor location were found to be statistically significant between OS and PFS. However, RDW and ALP had no significant difference in OS or PFS (Table 2; Figure 2).
Univariate Analysis for 5-Year OS and PFS.
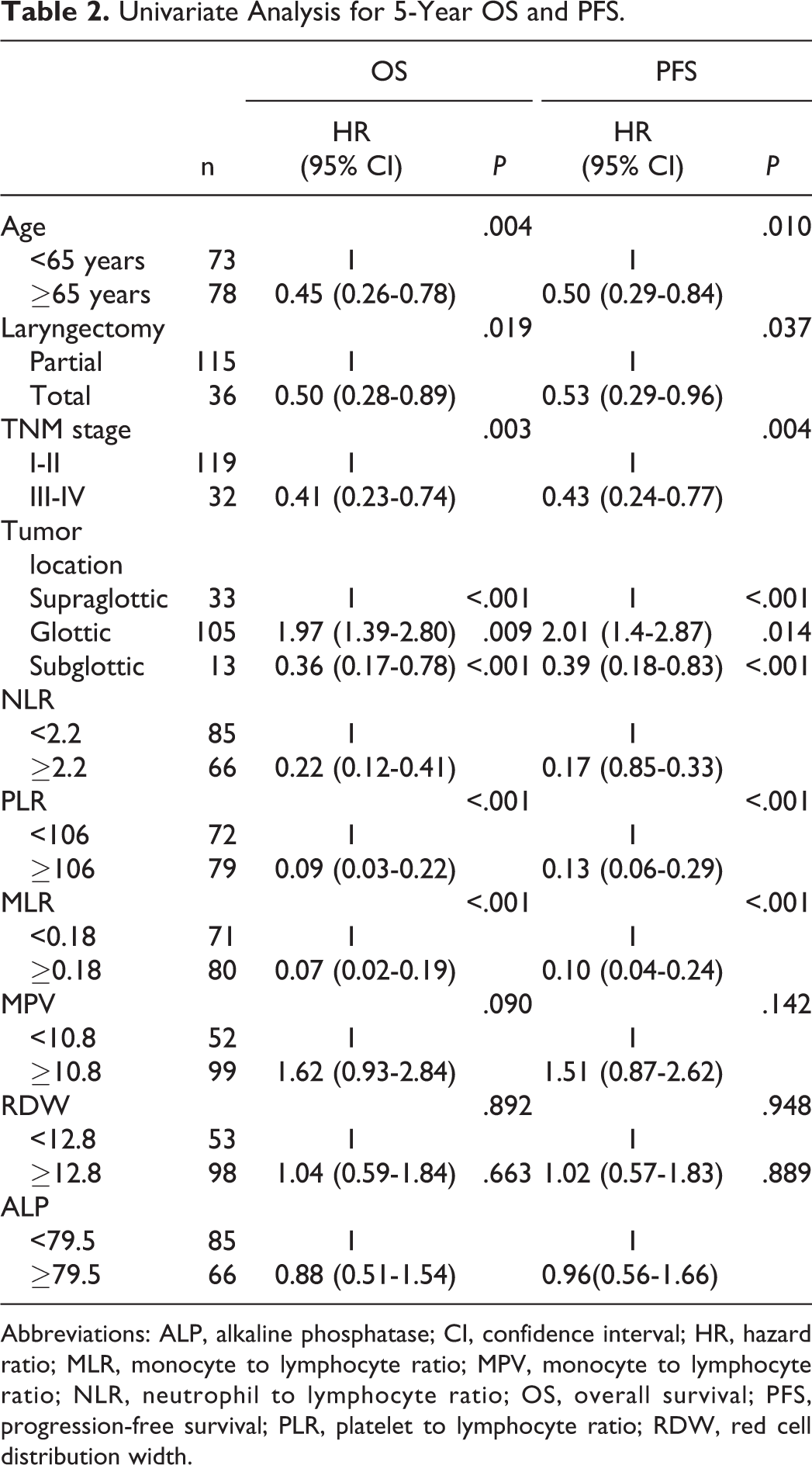
Abbreviations: ALP, alkaline phosphatase; CI, confidence interval; HR, hazard ratio; MLR, monocyte to lymphocyte ratio; MPV, monocyte to lymphocyte ratio; NLR, neutrophil to lymphocyte ratio; OS, overall survival; PFS, progression-free survival; PLR, platelet to lymphocyte ratio; RDW, red cell distribution width.

Kaplan-Meier survival curves for neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and monocyte to lymphocyte ratio (MLR) on 5-year overall survival (OS) and progression-free survival (PFS).
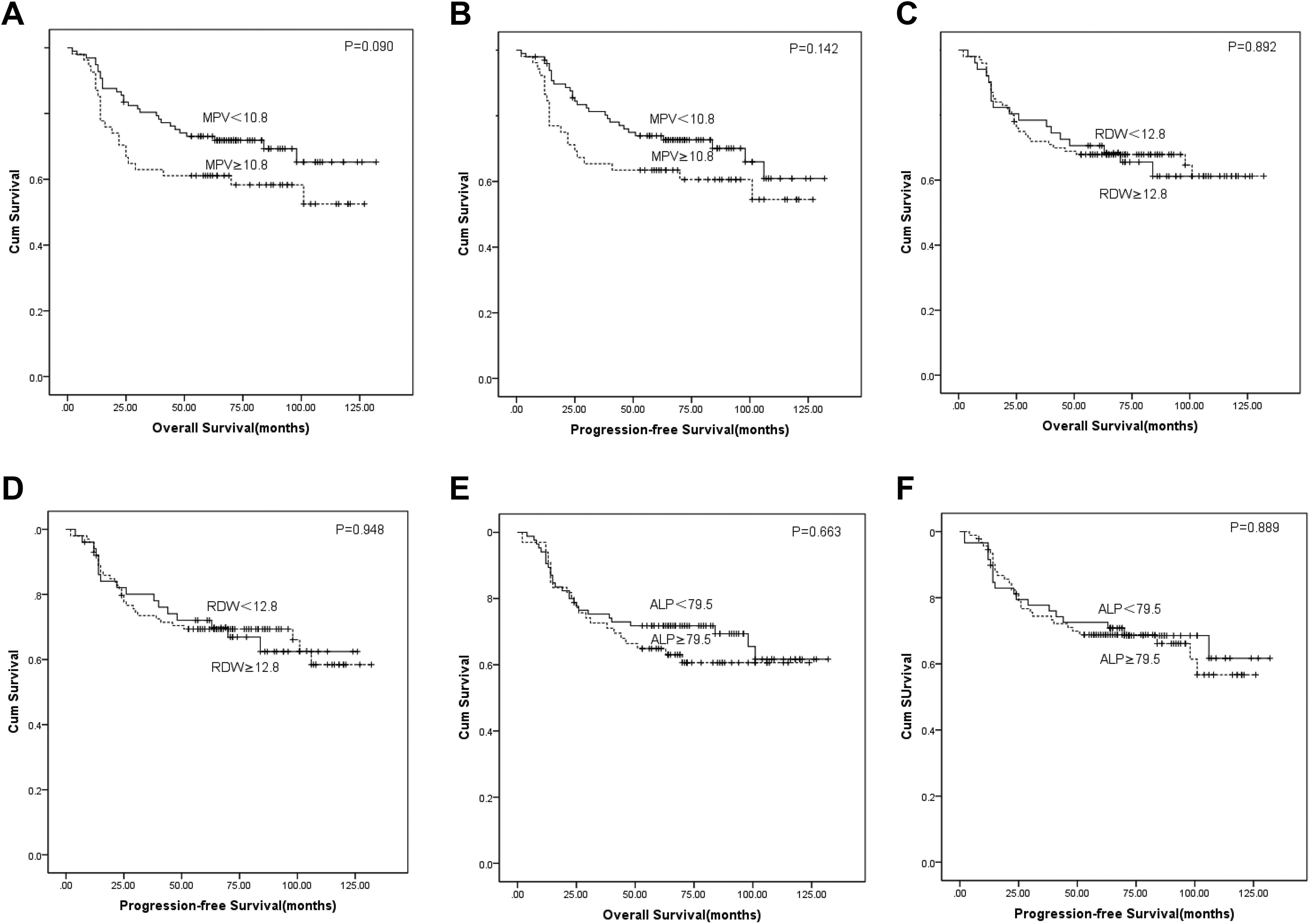
Kaplan-Meier survival curves for monocyte to lymphocyte ratio (MPV), red cell distribution width (RDW), and alkaline phosphatase (ALP) on 5-year overall survival (OS) and progression-free survival (PFS).
The Prognostic Value of Inflammatory Biomarkers on Multivariate Analysis
Multivariate analysis indicated that NLR (OS: hazard ratio [HR] = 3.02, 95% CI: 1.28-7.10, P = .011; PFS: HR = 3.56, 95% CI: 1.47-8.62, P = .005), PLR (OS: HR = 0.33, 95% CI: 0.14-0.78, P = .011; PFS: HR = 0.016, 95% CI: 0.10-0.79, P = 0.016), and MLR (OS: HR = 0.29, 95% CI: 0.11-0.76, P = .012) were independent 5-year prognostic factors in this study (Table 3; Figure 1).
Multivariate Analysis for 5-Year OS and PFS.
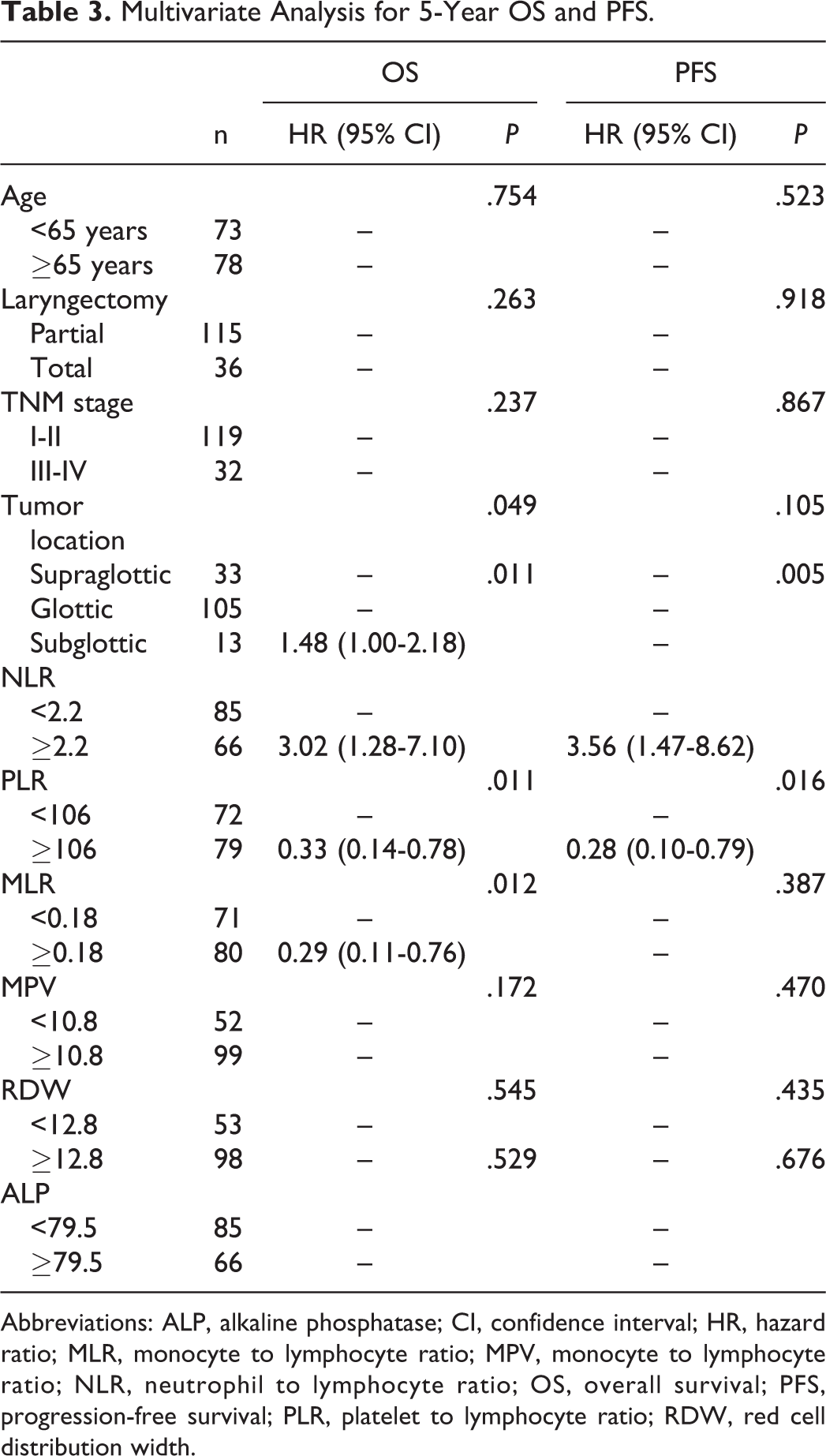
Abbreviations: ALP, alkaline phosphatase; CI, confidence interval; HR, hazard ratio; MLR, monocyte to lymphocyte ratio; MPV, monocyte to lymphocyte ratio; NLR, neutrophil to lymphocyte ratio; OS, overall survival; PFS, progression-free survival; PLR, platelet to lymphocyte ratio; RDW, red cell distribution width.
Discussion
Chronic inflammation caused by alcohol and tobacco use plays a crucial role in the development of LSCC. In cancer, inflammation is a link between intrinsic (oncogenes, genome stability, and tumor suppressors) and extrinsic (immune and stromal components) factors. 9–10 The inflammatory cells together with the cytokines or chemokines which they produce are involved in almost every step of tumor development and progression. Zhang et al confirmed by immunostaining of clinical samples that tumor-associated neutrophils displayed immunosuppressive capabilities and inhibited T-cell activity when the microenvironment changed. Secreted factors, such as cytokines and chemokines, generally help in regulating angiogenesis. These factors include interleukin (IL) 1, IL-13, and vascular endothelial growth factor (VEGF) and are basic factors for promoting angiogenesis. Angiogenesis ensures constant and steady supply of oxygen and nutrients to cancerous cells and tissues. 11 Chronic inflammation is responsible for the induced immunosuppression in the tumor microenvironment. This was established by creating a pathology-free chronic inflammation mouse model in the laboratory. The outcome was surprising that the ex vivo and in vivo functions of both T- and natural killer cells in mice were impaired. Moreover, lymphocytopenia is usually indicative of immunosuppression. 12–13
Our study showed that NLR in the peripheral blood of patients with LSCC is an independent prognostic biomarker and has significant prediction effects on OS and PFS. A high NLR means relative increase in neutrophils and decrease in lymphocytes. This may suppress lymphokine-activated killer cells and decrease survival time in patients with LSCC. The ultimate principle of NLR is to compare the inflammatory response (ie, the neutrophils) of the host to cancer with the immune response of the host (ie, the lymphocytes). The TINs can produce VEGF, IL-8, IL-25, matrix metalloproteinase 9 (gelatinase B), and gelatinase-associated lipocalin, which can increase the risk of tumor differentiation, angiogenesis, invasiveness, and metastasis. 14 –16 Zhang et al reported that the CD8+ T cells specifically control the tumor activity by apoptosis and cytotoxic effect so that the lymphocyte counts are inversely proportional to the severity of cancer. 17 Several clinical studies have determined that a high NLR value is associated with poor prognosis and survival in cancers of the head and neck. Fu et al were among the first to demonstrate that preoperative NLR ≥2.59 in patients with LSCC was an independent prognostic factor for long-term, cancer-specific survival (CSS) and OS. 18 Rassouli et al showed that a higher pretreatment NLR values (>4.27) is connected with higher rates of recurrence. Moreover, NLR/PLR combination was reported to be as good as TNM staging in predicting survival rates. 19 Similarly, Haddad et al advocated that NLR values (≥5) had a high mortality and were related to a remarkable decrease in OS. 20 In addition, the effect of NLR on OS and PFS also exists in other cancers, including nasopharyngeal carcinoma, lung cancer, colorectal cancer, and renal cancer. 21 –24
Platelets trigger blood clotting by aggregation and interaction with endothelial cells when body tissues are damaged. If platelets bind to immune cells, they can modulate an immune response. When tumor cells are lysed by natural killer cells and remain circulating in the blood stream, platelets get into direct contact with these tumor cells and platelet-derived growth factor through releasing transforming growth factor-β. The overall effect is the induction of epithelial–mesenchymal transition. Therefore, they release VEGF and promote tumor angiogenesis. Furlan et al reported that antiplatelet therapies had a better prognosis in patients with head and neck squamous cell carcinoma. 25 Moreover, tumor cells release soluble molecules such as adenosine diposphate and thrombin to activate platelets. Tumor cells also secrete IL-6 and augment thrombopoietin synthesis, resulting in paraneoplastic thrombocytosis. Therefore, these experimental results suggest that the interactions between tumor cells and platelets can lead to poor prognosis in patients with LSCC. 26 Zhong et al proved the changes in PLR have strong predictive significance of LSCC recurrence and mortality. 27 In univariate analysis, we found that PLR has significant predictive role, and statistically significant difference in PLR was determined for 5-year OS and PFS. The MPV may be an independent prognostic biomarker to significantly affect the distant metastasis.
In addition, the prognostic values of MLR, MPV, RDW, and ALP were also analyzed. The MLR may be an independent prognostic factor for 5-year OS. Tumor-associated macrophages derived from monocytes can stimulate tumor cell proliferation, angiogenesis, and metastasis. 28 The ALP showed some prognostic function in metastatic prostate cancer, bone metastatic cancer, and other solid tumors. Inflammation inhibits red blood cell maturation through destroying the red blood cell membrane, leading to an increase in RDW. One study indicated that higher RDWs (>14.4%) increased the locoregional recurrence rate 5.8-fold and was independently prognostic of distant metastasis-free survival in patients with LSCC. 29 Kara et al also found that a high RDW increases mortality by up to 4.6 times. 30 However, RDW and ALP had no important significance on OS or PFS in this study. Univariate analysis showed significant prognostic value of age, laryngectomy methods, TNM stages, and tumor location. In clinicopathology, TNM stages are widely used as standards for evaluating the degree of tumor progression and prognosis. Brandstorp-Boesen et al studied 1615 patients with laryngeal cancer. Recurrence rates increased in those patients who had the following characteristics: those who had supraglottic cancer, those who were younger, those whose tumors had progressed to T2 to T3 stage, and those who had obtained earlier treatment. 31 Haapaniemi et al’s study on patients with T2 glottic and T2 supraglottic cancer in Finland showed poor survival outcomes. Moreover, total laryngectomy had the highest local control rate for advanced tumors. 32 However, these factors only exists in univariate analysis and need to be verified further by additional research.
There were several limitations in our study. For instance, there was a retrospective study based on only 151 patients. There was certainly a possibility of selection bias. Besides, a possible bias related to the treatment should be considered. As a result, these analyses need additional more prospective and multicentered studies to support the prognostic role of inflammatory biomarkers.
Conclusions
High NLR, PLR, and MLR had significantly poor survival outcome in patients with LSCC. Based on the 5-year survival prognostic assessment of results from this study, PLR and MLR are potential independent prognostic factors worth considering. The NLR in the peripheral blood of patients with LSCC was an independent 5-year prognostic biomarker and was associated with worse OS and PFS. The NLR as a key component of prognosis among patients with LSCC is important when evaluating the survival time in patients or when using anticancer therapies to decrease laryngeal carcinoma cell proliferation and metastasis. Additional prospective, randomized studies with larger samples are required to validate our results.
Footnotes
Authors’ Note
Youfang Xun and Maohua Wang are co-first authors. No informed consent from patients is required because this is a retrospective study.
Acknowledgments
Special thanks were given to Dr Bing Guan and Dr Chenjie Yu for their support and Mr Maohua Wang for his writing assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The Project of Invigorating Health Care through Science, Technology and Education (ZDXKB2016015) and Nanjing Medical Science and Technique Development Foundation (QRX17051).