
Abstract

In the late 1800s, Schwartze’s technique of “modern mastoidectomy” 1 with a hammer and gouge was considered a great refinement compared to the primitive and dangerous trephines previously used for opening the mastoid antrum. It would take a half-century of innovation before otolaryngologists would have the experience of drilling off the mastoid cortex and skeletonizing the middle fossa dura with the smooth, vibration-free strokes of a high-speed mastoid drill.
The story of the mastoid drill parallels the development of rotatory dental instruments. In the late 1780s, John Greenwood a cabinet maker turned dentist adapted his mother’s spinning wheel foot treadle and used it to rotate a dental hand drill. He used a fluted bur to shape hippopotamus ivory dentures including some for President George Washington. 2 Within 50 years, tooth dissection in live patients became possible. Elliott’s suspension engine used a treadle and an articulated pulley system to rotate a bur held in a pencil-like handpiece (Figure 1). Such dental drills removed diseased tooth enamel and dentin to create a smooth depression to which fillings were applied.
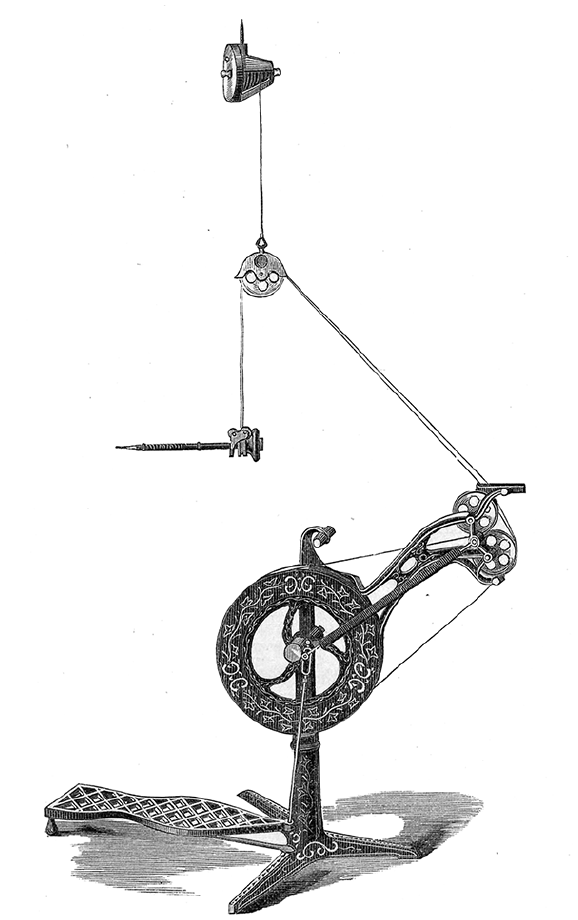
Elliott’s suspension dental drill. 3
In 1876, the surgeon Arthur Mathewson took the bold step of using Elliott’s dental engine to remove external auditory canal exostoses. 3 He wrote, “In comparison with any of the methods of operation employed in the cases collated, that with the dental engine seems to me the best, as being less tedious, less dangerous, and more effective.” He explained that the drill was safer because its rapid rotation allowed “perforations to be quickly made with so slight a pressure that there is little risk of injuring the deeper parts of the ear.”
George F. Green a mechanical engineer and inventor working in Philadelphia began developing an electric dental engine for the SS White Company. In 1875, he patented an engine with a battery-powered motor connected by gears to the drill handpiece. It generated little torque and was noisy and costly. It did not catch on (Figure 2).
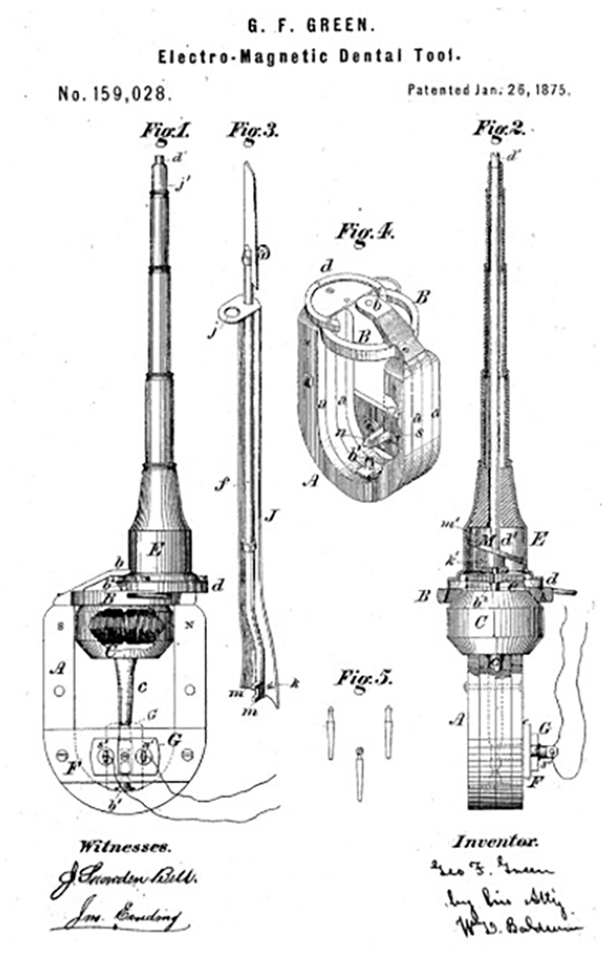
Patent for George F. Green’s Electro-magnetic dental tool (US Patent 159028).
In 1893, William Macewen, the Scottish pioneer neurosurgeon advocated the use of a dental engine to expose the mastoid antrum. 4 He used globular fluted burs to remove the mastoid cortex and, when necessary, drill along the tegmen to expose the tympanic attic. “This instrument applied lightly to the bone removes osseous flakes, leaving a smooth, almost polished surface, upon which any dark objects, such as are presented by the interstices of the mastoid antrum or any of the adjoining cells, are readily recognized previous to being opened.” 5
By the 1920s, Julius Lempert described endaural subcortical mastoidectomy performed entirely with a dental drill. Despite his enthusiasm, the mallet and gouge approach dominated otologic surgery into the 1950s. Existing drills, usually powered by a small motor and belts or pulleys, had a maximum speed of 2500 to 10,000 rpm (Figure 3). Dissection with these low-speed drills progressed slowly as they skipped and stalled during the procedure. 6
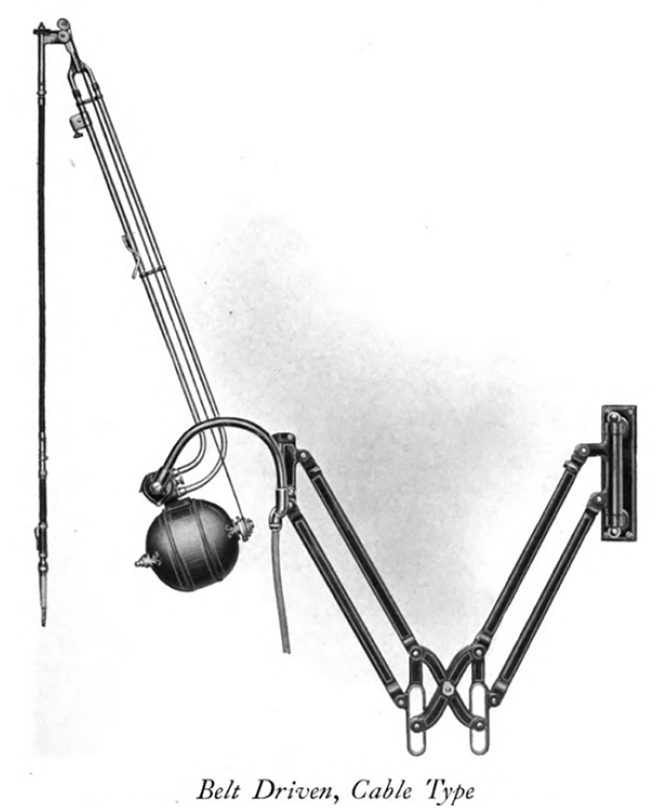
A belt-driven dental engine (a catalogue of Ritter dental equipment: chairs, engines, lathes, distributing panels, air compressors, unit equipment, ionization equipment, spray bottle warmers, air fittings, supplies and accessories for the above. Ritter Dental Manufacturing Co., Inc. Rochester, N.Y. [c1919] p.27.)
Then, in 1945, George F. Green of New Zealand patented a pneumatic turbine that used compressed air to drive a dental drill. By 1956, the first successful air-driven turbine handpiece became available. By suspending the turbine in air, friction and vibration were reduced, allowing speeds up to 300,000 rpm. 7 Within a decade several manufacturers had marketed high-speed, low-torque air-driven and micro-motorized handpieces. The age of controlled temporal bone dissection had begun.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Level of Evidence
5 – expert opinion.