
Abstract

Introduction
Walsham, Asch, and Goldman are familiar names in Otolaryngology operating suites throughout the world (Figure 1). The instruments that carry their names are commonly used for closed reduction of displaced nasal fractures. The stories of these instruments’ inventors, and why they created these tools, are less well known.
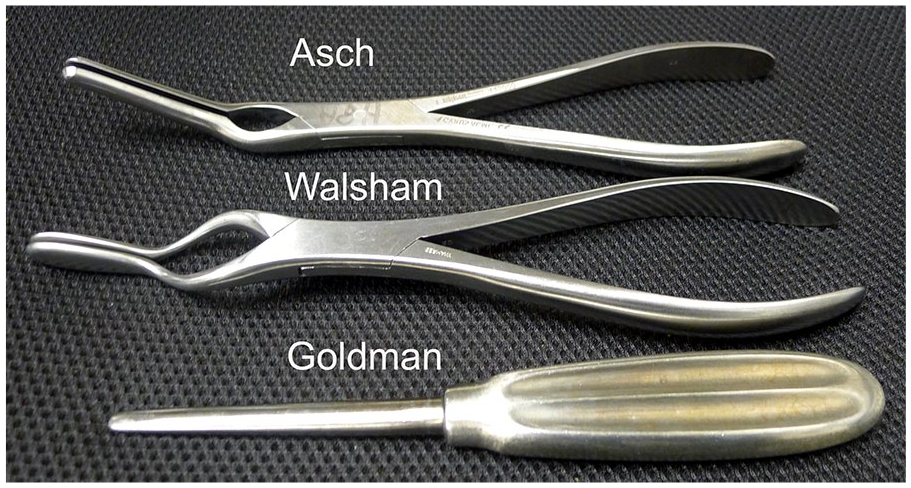
Asch and Walsham forceps and the Goldman displacer septum elevator.
Walsham Forceps
William Johnson Walsham 1847 to 1903—Lecturer on Surgery and on Anatomy, St Bartholomew’s Hospital, London.
In the latter half of the 19th century, methods for correction of the deviated nasal septum were a subject of intense debate. The advent of ether and chloroform for general anesthesia and the Lister’s promotion of antisepsis led to a boom in elective surgery. Nasal septal manipulation was considered safer than open surgery. Walsham, using his experience in orthopedics, advocated relocation of the deflected septum with forceps of his own design followed by a protracted period of postoperative splinting (Figure 2). His textbook, “Surgery, its theory and practice”
1
describes the procedure as follows: Treatment—The septum may generally be forcibly straightened by the forceps and then retained in position for the first few days while parts are being consolidated, by the retention apparatus shown in the figure, and subsequently by ivory or vulcanized plugs.
Walsham did use his forceps to correct chronically deviated nasal bones as well as the nasal septum, but notes that, “Great force is required, and care must be taken, by properly padding the forceps, not to injure the soft parts.”
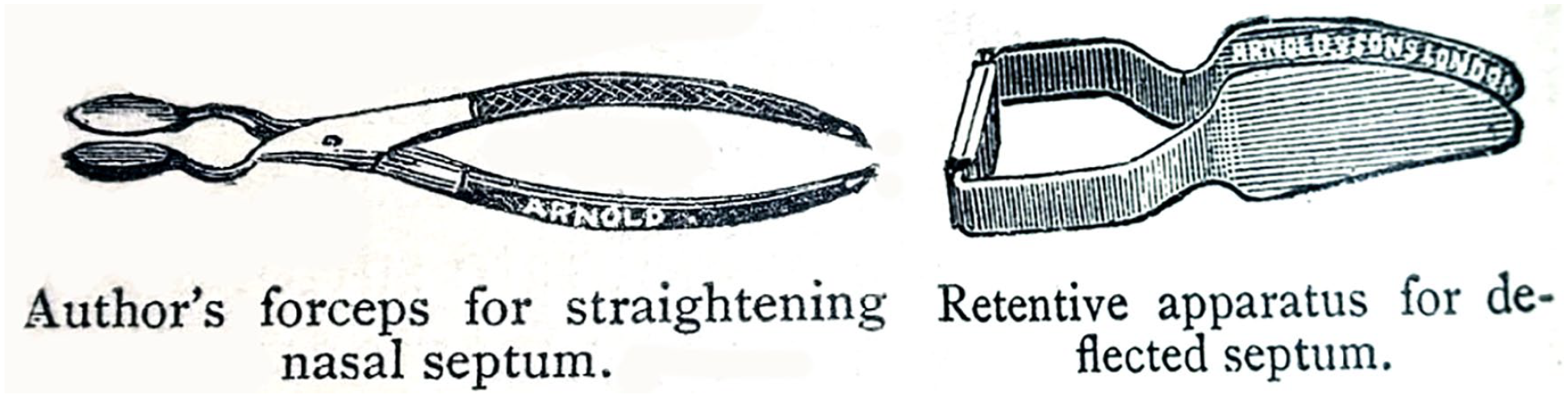
Walsham forceps, retentive apparatus. 1
Asch Forceps
Morris Joseph Asch (1833-1902) was born in Philadelphia and educated at the University of Pennsylvania and Jefferson Medical College. 2 Following graduation, he served as an assistant to the pioneering Jefferson surgeon Samuel D. Gross until the start of the American Civil War. He joined his 3 brothers in volunteering for the Union Army and cared for the wounded at the battles at Chancellorsville, The Wilderness and Gettysburg. After 8 years as staff surgeon to General P. H. Sheridan, he left the Army of the Potomac and began the private practice of surgery focusing on the ear, nose, and throat. He was eventually named Professor of Laryngology at the New York Polyclinic Institute and cared for the poor at the New York Eye and Ear Infirmary.
As one of the founding members of the American Laryngological Association he presented his work on correction of nasal septal deviations in 1890. 3 Asch describes septal manipulation but only to denounce the method as ineffective. He advocated “destroying the resiliency of the septum” using “a pair of strong cartilage-scissors, one blade blunt and narrow. . . the other a cutting blade” 4 (Figure 3). The Adams compressing forceps (now commonly called Asch forceps), described 15 years earlier by William Adams, 5 were used to align the fragments prior to splinting.

(A) Adams compressing forceps, (B) Asch straight septal scissors. 4
The Goldman Bar
The Goldman displacer septum elevator has a sturdy handle and broad, blunt blade (Figure 1). It is well suited to forceful manipulation of depressed nasal bones and is widely used for this purpose. Irving B. Goldman, a New York rhinologist of the early 20th century, had another purpose in mind, however. In his presentation before the AMA Section on Laryngology, Otology, and Rhinology in 1955, 6 he describe the used of his strong elevator to dissect the mucoperichondrium and periosteum of the nasal septum through a transfixion incision, then, “the second phase of the operation consists in shifting the bony septum into midposition with a ‘displacer’. This step is carried out in a low plane without force. It is surprising how easily the intermaxillary ridge (bony base of septal skeleton) and vomer can be fractured and swung mesially.” Goldman did recognized the value of the displacer septal evevator for closed reduction of nasal fractures. 7 In his 1964 article on correction of recent nasal fractures he describes the combined use of Walsham forceps and the large version of his septal displacer.
The depresssed side is grasped with a lateral Walsham forceps at the (nasomaxillary) suture line, and the blades are closed to reduce the dislocation. . . The external deformity is then corrected by elevating the bones into their proper position with a heavy, flat elevator on the depressed side (the Goldman displacer) and by adequate thumb pressure on the opposite, convex side. A click will often become audible as the bones are replaced into their normal site.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.