
Abstract
Introduction
Sudden sensorineural hearing loss (SSNHL) is characterized by a rapid onset within 72 h, manifesting as a decline in hearing of at least three adjacent frequencies exceeding 30 dB. 1 Severe cases are frequently accompanied by tinnitus, vertigo, nausea, and vomiting, making it an emergency in the field of otorhinolaryngology. One of the recent studies indicates that the incidence of SSNHL ranges from 5 to 30 per 100,000 individuals, 2 with the younger population disproportionately represented. It is widely accepted that SSNHL may be associated with factors such as viral infections, circulatory disturbances, autoimmune deficiencies, tumors, and ototoxic medications. Some researchers propose that chronic inflammation could play a role in the pathogenesis of SSNHL. 3 On the one hand, the cochlea’s blood supply predominantly relies on a singular labyrinthine artery; prolonged inflammation can lead to vascular sclerosis and alterations in permeability, resulting in inadequate blood flow to the inner ear and diminished endolymphatic potential production—thereby impairing auditory conduction. 4 On the other hand, inflammation induces endothelial dysfunction and promotes a hypercoagulable state within the bloodstream, which accelerates thrombosis and disrupts auditory function. 5 An increasing body of research has demonstrated that various inflammatory and metabolic markers 6 —including white blood cell count, neutrophil count, platelet-related parameters, low-density lipoprotein levels, high-density lipoprotein levels (HDL), high-sensitivity C-reactive protein, serum albumin levels—and C-reactive protein are closely linked to the occurrence of SSNHL.7-12 Currently-available treatment modalities such as pharmacotherapy and hyperbaric oxygen therapy have been shown to enhance microcirculation within the ear and augment its blood supply for most patients; however, some individuals continue to experience persistent symptoms posttreatment, which significantly affect their daily lives along with their physical and mental well-being. Identifying factors contributing to unfavorable outcomes in SSNHL patients is crucial for improving prognosis through targeted interventions. This study aimed to conduct a comprehensive analysis of relevant risk factors associated with poor prognoses among patients suffering from SSNHL while formulating a tailored therapeutic strategies—thus providing valuable insights for enhancing prevention efforts against adverse outcomes.
Materials and Methods
General Information
This retrospective analysis included 123 patients diagnosed with SSNHL who received treatment at Zhongxian People’s Hospital in Chongqing from March 2022 to March 2024. In accordance with the Chinese Medical Association’s Guidelines for the Diagnosis and Treatment of SSNHL, a comprehensive set of inclusion and exclusion criteria was established for this study. The inclusion criteria comprised no prior use of steroid medications, unilateral SSNHL, and exclusion of hearing loss attributable to organic lesions confirmed by magnetic resonance imaging. Exclusion criteria encompassed coronary heart disease, chronic liver disease, pulmonary conditions, infectious diseases, autoimmune disorders, any ear-related pathologies (such as chronic otitis media, otosclerosis, history of ear trauma, and Meniere’s disease), vestibular schwannoma, or traumatic lymphatic fistula. This study received ethics approval from the Ethics Review Committee at Zhongxian People’s Hospital in Chongqing.
Preoperative Peripheral Blood Laboratory Examination
Prior to the initiation of therapy, peripheral blood samples were collected from each participant between 7:00 AM and 8:00 AM while ensuring that subjects were in a fasting state. The following parameters were measured: neutrophils, lymphocytes, platelets, C-reactive protein, fibrinogen, HDL, average platelet volume, serum albumin, and globulin. Additionally, the ratios of neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-C-reactive protein (LCR), fibrinogen-to-high-density lipoprotein (FHR), mean platelet volume-to-platelets ratio (MPR), and serum albumin-to-globulin (SGR) were calculated.
Hearing Test
All 123 patients diagnosed with SSNHL underwent pure-tone audiometry both prior to and following therapy. Bone and air conduction thresholds were assessed at frequencies of 250, 500, 1000, 2000, 4000, and 8000 Hz. Therapeutic outcomes were categorized as “cure” (complete restoration of hearing to normal), “significantly effective,” “effective,” or “ineffective” based on the efficacy evaluation criteria outlined in the Chinese Medical Association’s Guidelines for Diagnosis and Treatment of SSNHL. The average hearing threshold recovery at the affected frequency was deemed a cure. A decrease in hearing threshold greater than 30 dB was classified as significantly-effective treatment; a reduction between 15 and 30 dB was considered effective treatment, while a decrease of less than 15 dB was regarded as ineffective treatment. Cures, significantly-effective treatments, and effective treatments were collectively included in the effective group, whereas ineffective treatments were categorized into the ineffective group.
Interventions and Dosage
The following protocol was implemented for the treatment of 123 patients with SSNHL. Dexamethasone, at a dosage of 5 mg, was administered via injection into the tympanic cavity of the affected ear every other day for a total of three injections. Additionally, intravenous administration of methylprednisolone and ginkgo biloba extract was conducted at doses of 40 and 20 mg respectively over a duration of 7 to 10 days (Figure 1).
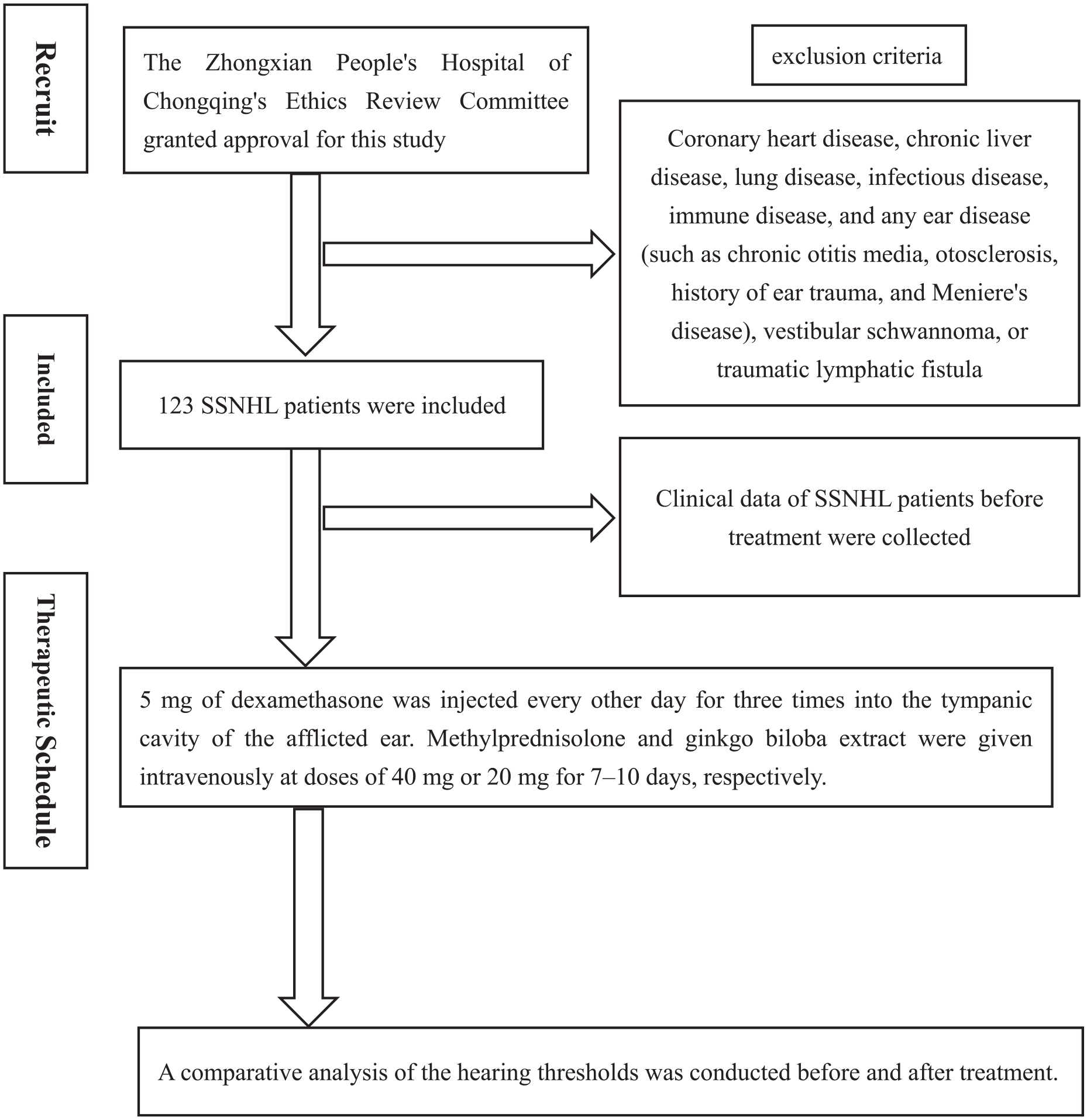
Protocol flowchart of this studies.
Statistical Procedures
The data were analyzed using the SPSS 26.0 statistical software. A chi-squared test was employed for the comparison of categorical data, while a t-test was utilized for the assessment of continuous variables. Additionally, binary logistic regression analysis was conducted to evaluate multiple factors simultaneously. To assess the predictive value of these factors on treatment efficacy, receiver operating characteristic (ROC) curves were generated, and the area under the ROC curves (AUC) was calculated. The significance level was established at .05 with a two-tailed approach.
Results
Univariate Analysis of Poor Prognosis in Patients With Sudden Sensorineural Hearing Loss
A univariate analysis was performed to evaluate the prognostic factors associated with SSNHL. The findings indicated that a poor prognosis for SSNHL is significantly correlated with disease onset time ≥7 days (X² = 35.54, P < .01), past hearing loss (X² = 5.05, P = .03), combined vertigo (X² = 9.45, P < .01), and NLR (t = 0.46, P = .04). Conversely, no significant associations were found with gender, age, diabetes mellitus, chronic kidney disease, hyperthyroidism, MRI evidence of inner ear hemorrhage, LCR, FHR, MPR, or SGR (P > .05). (Table 1).
Univariate Analysis of Poor Prognosis in Patients With Sudden Sensorineural Hearing Loss.
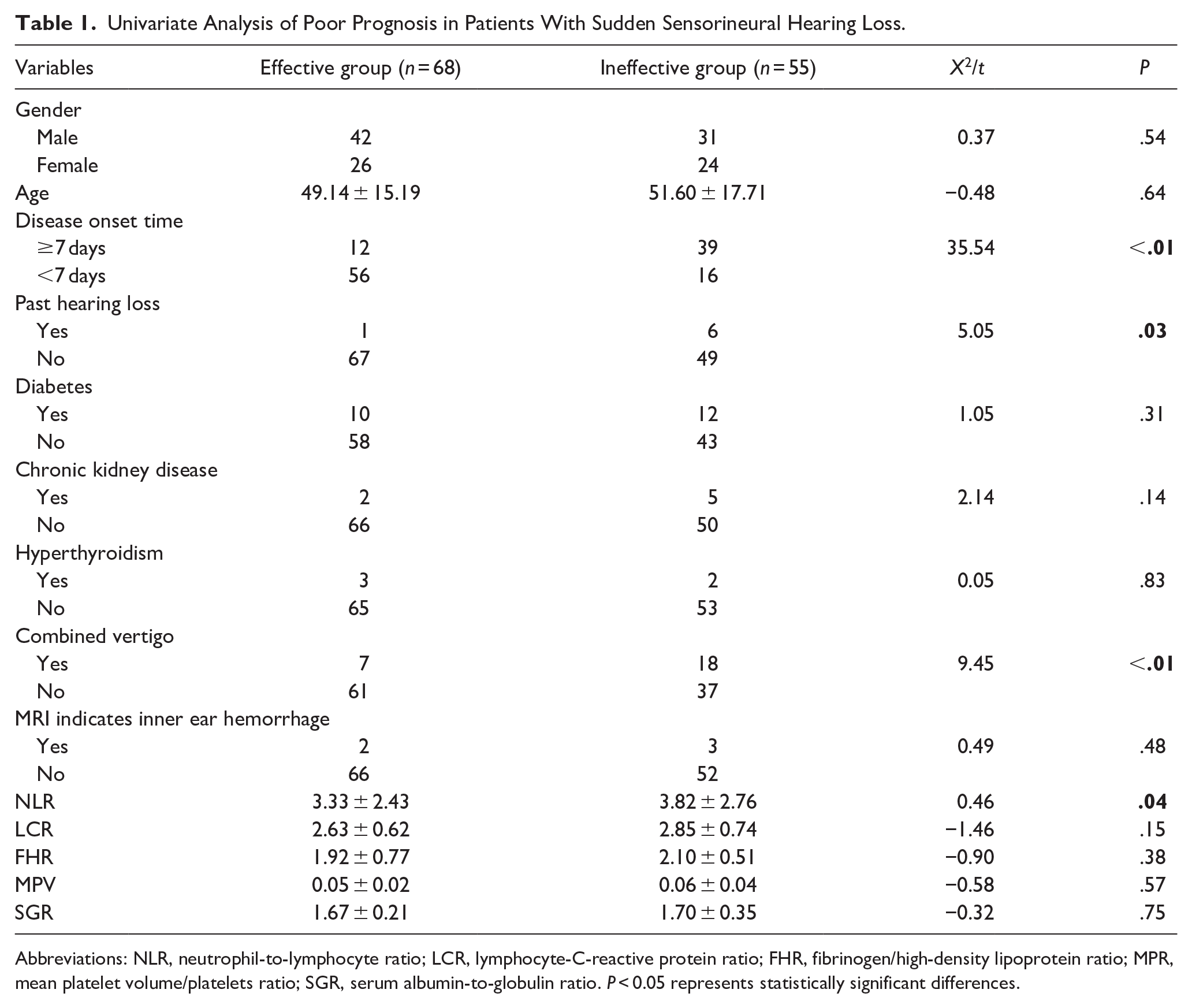
Abbreviations: NLR, neutrophil-to-lymphocyte ratio; LCR, lymphocyte-C-reactive protein ratio; FHR, fibrinogen/high-density lipoprotein ratio; MPR, mean platelet volume/platelets ratio; SGR, serum albumin-to-globulin ratio. P < 0.05 represents statistically significant differences.
Multivariate Logistic Regression Analysis of Poor Prognosis in Patients With Sudden Sensorineural Hearing Loss
A multivariate analysis was performed to identify the prognostic factors associated with SSNHL. The findings from the multivariate logistic regression analysis indicated that disease onset time ≥7 days (OR = 0.09, P < .01), combined vertigo (OR = 0.24, P < .01), and NLR (OR = 0.92, P = .036) were identified as independent risk factors for poor prognosis in SSNHL. (Table 2).
Multivariate Logistic Regression Analysis of Poor Prognosis in Patients With Sudden Sensorineural Hearing Loss.
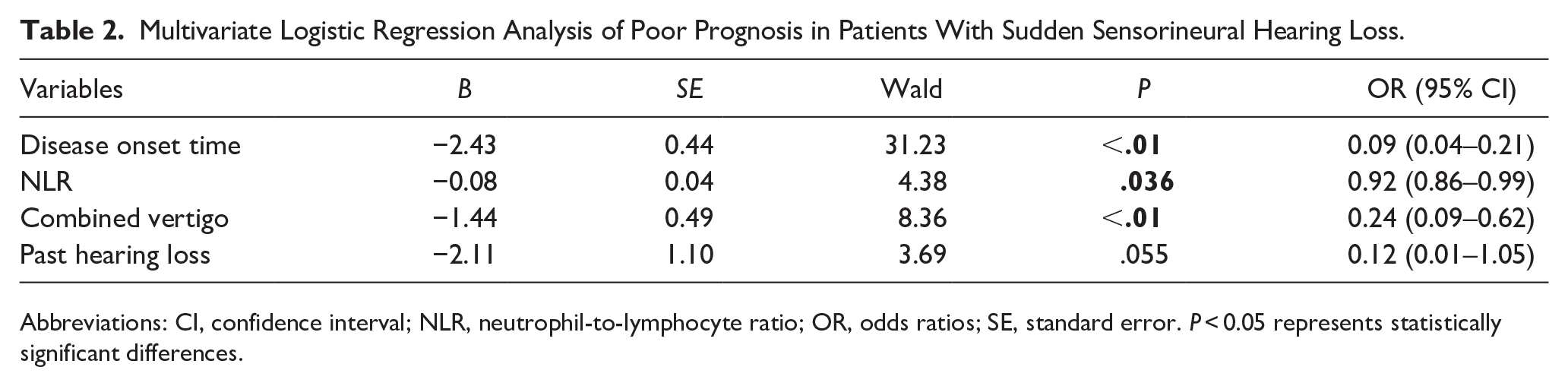
Abbreviations: CI, confidence interval; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratios; SE, standard error. P < 0.05 represents statistically significant differences.
Analysis of Predictive Value for the Treatment Effect of Sudden Sensorineural Hearing Loss
We employed ROC curve to evaluate the predictive value of treatment effects in SSNHL. The AUCs for disease onset time, combined vertigo, and NLR were 0.766, 0.612, and 0.553, respectively, indicating their substantial predictive value for SSNHL prognosis (Table 3).
Analysis of Predictive Value for the Treatment Effect of Sudden Sensorineural Hearing Loss.
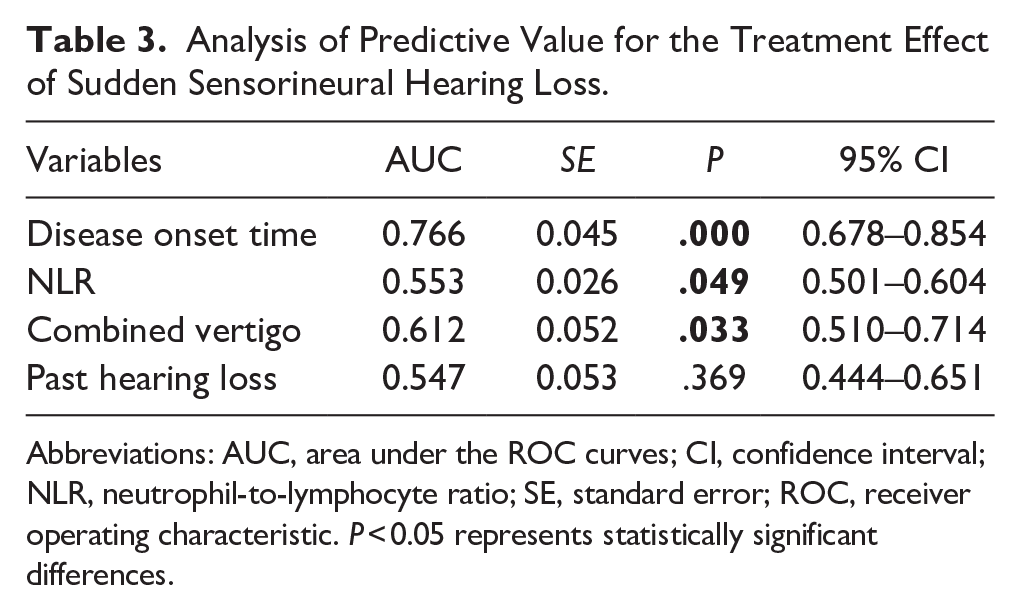
Abbreviations: AUC, area under the ROC curves; CI, confidence interval; NLR, neutrophil-to-lymphocyte ratio; SE, standard error; ROC, receiver operating characteristic. P < 0.05 represents statistically significant differences.
Discussion
In recent years, the rapid development of the social economy has led to an increase in individuals’ stress levels, which correlates with a rising incidence of SSNHL, particularly among younger populations. Early intervention is critical for preserving residual hearing; thus, understanding the pathogenesis of SSNHL is essential. Although the exact mechanisms underlying SSNHL remain unclear, many patients experience symptom relief through comprehensive clinical treatment; however, poor prognoses still occur in some cases. Therefore, investigating relevant risk factors associated with unfavorable outcomes and developing preventive strategies are vital for enhancing clinical prevention and management of SSNHL with poor prognosis.
Generally-recognized mechanisms contributing to SSNHL include viral infection and immune response theory, 13 endolymphatic hydrops, stress theory,14,15 and microcirculation disturbances.16,17 Corresponding treatments encompass anti-inflammatory hormones (such as methylprednisolone and dexamethasone), neurotrophic agents (such as mecobalamin), and vasodilators (including tanshinone injection and ginkgo biloba extract injection). However, their efficacy varies.
The findings from both univariate and multivariate logistic regression analyses in this study indicate that disease onset time ≥7 days (X² = 35.54, P < 0.01) (OR = 0.09, P < 0.01) and combined vertigo (X² = 9.45, P < 0.01) (OR = 0.24, P < 0.01) are independent risk factors for poor prognosis in SSNHL. Disturbances in inner ear circulation represent one potential pathophysiological mechanism underlying SSNHL, characterized by distinct stages of vascular distribution. Consequently, blood flow within the inner ear is typically slow and stable, predisposing it to lipid deposition; subsequent blockage can lead to capillary damage. Prolonged intervals between symptom onset and treatment hinder functional recovery and complicate auditory improvement efforts, ultimately resulting in unfavorable prognoses.18,19 Therefore, prompt medical intervention following SSNHL onset is crucial to minimize the duration before treatment initiation. Our analysis revealed that patients with a history of SSNHL or recurrent hearing loss posttreatment exhibit poorer prognoses than those experiencing isolated episodes (X² = 5.05, P = 0.03). Thus, enhancing clinical diagnostic accuracy is essential for early identification of hearing loss and timely implementation of appropriate treatments aimed at mitigating poor prognostic risks. Patients presenting with vertigo often experience vestibular dysfunction accompanied by extensive damage to auditory systems; such cases are more likely associated with adverse outcomes.20,21 Special attention should be directed toward these individuals through tailored treatment strategies while monitoring relevant indicators to reduce the incidence of poor prognoses in clinical settings. The impact of systemic diseases such as hypertension and diabetes on SSNHL efficacy remains contentious within existing literature; some studies identify conditions such as hypertension, diabetes mellitus, chronic kidney disease, and hyperthyroidism as risk factors for SSNHL,22,23 whereas other research suggests no correlation exists regarding their influence on prognosis. 24 Our study’s results indicated that diabetes (X² = 1.05, P = .31), chronic kidney disease(X² = 2.14, P = .14), and hyperthyroidism(X² = 0.05, P = .83 ) were not significantly related to SSNHL prognosis. Age-related outcomes concerning SSNHL have been reported variably across different studies: Some suggest worse prognoses among elderly patients, 25 while others assert age does not correlate with prognosis severity—our findings align with the latter perspective, indicating no association between age and SSNHL prognosis. Routine MRI examinations were conducted on patients diagnosed with SSNHL to exclude organic lesions; five subjects exhibited bleeding lesions within the inner ear region—a condition where batroxobin (Botropase can dissolve fibrinogen, reduce blood viscosity, increase blood fluidity, expand peripheral blood vessels and other mechanisms to increase the effective perfusion volume, and improve local hypoxia state) usage warrants caution due to its potential implications despite showing no direct relation to overall prognosis in cases involving inner ear hemorrhage, 26 consistent with our study’s conclusions (X² = 0.49, P = 0.48).
Recently, an increasing number of scholars have posited that chronic inflammation may play a role in the onset of SSNHL. SSNHL typically manifests acutely, triggering the body’s stress response mechanisms. 27 Inflammatory cells release various inflammatory and chemotactic factors. Given the cochlear vascular system’s heightened sensitivity to these inflammatory mediators, such exposure can result in vascular damage and compromise the blood-labyrinth barrier, thereby hindering endolymphatic potential generation and auditory conduction. Furthermore, the surface of endothelial cells is coated with glycocalyx, 28 which serves as a protective barrier against immune cell infiltration and serum macromolecule damage to the vascular endothelium. When an inflammatory state arises within the body, it stimulates endothelial cells to produce adhesion molecules that can detach glycocalyx and disrupt tight junctions; this allows inflammatory factors to infiltrate surrounding tissues and disturb auditory homeostasis. Conversely, prolonged chronic inflammation induces a hypercoagulable state in patients with SSNHL,29,30 predisposing them to thrombosis formation that leads to microcirculatory disturbances within the inner ear system. The inner ear primarily relies on labyrinthine arteries for its blood supply; thus, insufficient perfusion adversely affects cochlear hair cell growth and development, impairing auditory conduction capabilities. Various inflammatory markers—including white blood cells, neutrophils, lymphocytes, platelets, HDL, fibrinogen, CRP, and albumin—have been implicated in both the occurrence and progression of SSNHL; however, their predictive value remains limited. Recent studies have indicated that composite inflammatory markers such as NLR, PLR, Systemic Immune-Inflammation Index (SII) exhibit greater prognostic significance regarding SSNHL incidence than single markers due to their stability over time while being cost-effective (it can be obtained by blood test without any additional cost, economical and practical) for calculation purposes.31,32 In this study, we explored the relationship between some novel immune complexes and SSNHL. Our retrospective analysis revealed that NLR values were significantly higher in the ineffective group than those in the effective group, demonstrating statistical significance between groups—a finding consistent with prior research. 33 Other indices including LCR, FHR, MPR, and SGR showed no correlation with SSNHL prognosis. The AUC values for disease onset time ≥7 days, combined vertigo, and NLR were found to be 0.766, 0.612, and 0.553, respectively, indicating their potential utility as reliable prognostic indicators for SSNHL.
Meantime, the study included a number of restrictions. For instance, we studied the peripheral blood inflammatory markers of 123 patients with SSNHL in few existing clinical data. These SSNHL patients only had data available at the time of admission, and the follow-up time was brief. Secondly, the study has only remained at the level of cells, and no in-depth studies have been performed. Future prospective studies with larger sample sizes and exploration at the level of gene are required. It is still worth noting the results of our study despite these limitations.
Conclusion
In conclusion, through comprehensive factor and predictive analyses, it has been demonstrated that disease onset time ≥7 days, the presence of combined vertigo, and an NLR are independent risk factors influencing the prognosis of patients with SSNHL. Clinically, appropriate preventive measures should be implemented for high-risk patients exhibiting these characteristics to mitigate the likelihood of poor prognostic outcomes. However, this study is limited by an insufficient sample size; therefore, further investigations are warranted to enhance the sample size through diverse channels and centers.
Footnotes
Acknowledgements
Author’s Contributions
The study’s concept and layout were proposed by Maohua Wang. The data collection and analysis were carried out by Gang Deng and Xiangling Jiang. The literature search was completed by Gang Deng and Xiangling Jiang. The core manuscript was written by Gang Deng, while editing and critical revision were carried out by Maohua Wang. The study was managed by Maohua Wang. The final draught of the paper has been approved by all authors once they have read it. The final manuscript was read and approved by all writers.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from Research on the Evolution Mechanism of Hearing Impairment and Stepwise Rehabilitation Strategies for Middle-aged and Young Nasopharyngeal Cancer Patients Undergoing Radiotherapy Based on Big Data Mining Technology, The 2023 Guangdong Provincial Medical Science and Technology Research Fund Project (A2023382).
Ethical Statements
The study was approved by the Ethics Committee of the Ethics Review Committee of the Zhongxian People’s Hospital of Chongqing.
Grant Number
None.