
Abstract
Keywords
Introduction
Sudden sensorineural hearing Loss (SSNHL) is a common emergency in otolaryngology. SSNHL is commonly defined as SNHL of ≥30 dB over at least 3 frequencies occurring within 3 days. Hearing loss can be detected in any frequencies on an audiogram; 13.29% of patients had low-frequency (up-sloping pattern) hearing loss and 27.97% of patients had high-frequency (down-sloping pattern) hearing loss, while 58.74% of patients had hearing loss in all frequencies (flat, 30.77% or profound, 27.97%). 1 The audiogram shape may indicate different pathogenesis in the inner ear although its real pathogenesis is still unknown. According to the Chinese Medical Association (CMA) 2015 guidelines for the diagnosis and treatment of sudden deafness, SSNHL with low-frequency hearing loss is probably caused by membranous labyrinthine hydrops, high-frequency hearing loss by hair cell injury, flat hearing loss by stria vascular dysfunction or inner ear vasospasm, and profound hearing loss by inner ear vascular embolism or thrombosis. 2 The audiogram shape is also one of the factors that affect the prognosis for hearing recovery. Other factors affecting the prognosis include the severity of hearing loss, patient’s age, and the presence of vertigo. 3
Inflammation and vascular risk factors may play main roles in SSNHL. 4 Recent studies reported that several inflammatory indicators in peripheral blood, such as white blood cells (WBC), neutrophil-to-lymphocyte ratio (NLR), and monocyte-to-lymphocyte ratio (MLR) values, were elevated in SSNHL patients and related to the prognosis: the higher the levels of indicators, the poorer the prognosis.5-10 Systemic immune index (SII), a superior prognostic factor in certain diseases (eg endometrial cancer and acute ischemic stroke11-13), can also predict the prognosis of SSNHL. 13 However, the roles of these inflammatory indicators in SSNHL patients with different audiogram shape are still unknown. Therefore, in this study, we retrospectively analyzed peripheral blood inflammatory indicators in SSNHL patients to explore immune-inflammatory responses and their potential prognostic value in SSNHL patients with different audiogram shapes. The present study was approved by the ethics committee of Nanjing Drum Tower Hospital, the Affiliated Hospital of Nanjing University Medical School (IRB2021-459-02).
Methods
Patient Enrollment Criteria
We retrospectively analyzed 110 SSNHL patients who were hospitalized in the Department of Otolaryngology, Jinling Hospital Qinhuai Medical Center of Nanjing University, and Nanjing integrated traditional Chinese and Western Medicine Hospital Affiliated with Nanjing University of Chinese Medicine from January 2019 to September 2021. The inclusion criteria included ① the diagnostic criteria of SSNHL published by CMA was met 2 ; ② first time onset of unilateral hearing loss; ③ no steroid treatment was received before hospitalization; ④ the whole course of treatment was completed without interruption; ⑤ all hearing test data was collected before and after treatment; ⑥ acoustic neuroma and other immune-inflammatory inner ear diseases were excluded by auditory brainstem response (ABR) testing, internal auditory canal MRI scans, and other laboratory tests; and ⑦ patients with severe cardiovascular and cerebrovascular diseases, diabetes mellitus, hypertension, or liver and kidney diseases were excluded. Seventy-five healthy volunteers were enrolled as the normal control group.
Audiology Evaluation
All 110 patients were evaluated with pure tone audiometry, impedance audiometry, and ABR tests before and after treatment. According to the CMA guidelines, 2 initial audiograms were classified into 4 types: ① low-frequency hearing loss: pure tong average (PTA) in frequencies of .25-1 kHz was increased equal to or greater than 20 dB; ② high-frequency hearing loss: PTA in frequencies of 2-8 kHz (at least in 4k and 8k Hz) was increased equal to or greater than 20 dB; ③ flat type: PTA in frequencies from .25 to 8 kHz was increased equal to or less than 80 dB; and ④profound type: PTA in frequencies from .25 to 8 kHz was increased greater than 80 dB. 2
Hematology Evaluation
Fasting venous blood was collected from each patient before steroid treatment on the second day after admission to avoid the effects of steroids on leukocyte counts. 14 Numbers of white blood cells, neutrophils, lymphocytes, and platelets were counted using a fully automated blood cell analyzer. Neutrophil-to-lymphocyte ratio, MLR, platelet-to-lymphocyte ratio (PLR), and SII were then calculated. Systemic immune index = platelets × neutrophils/lymphocytes.
Treatment and Efficacy Criteria
A daily infusion of 87.5mg Ginkgo biloba extract (Taiwan Jisheng Chemical Pharmaceutical Co. LTD) was administrated immediately after admission. Systemic methylprednisolone (Pfizer Manufacturing Belgium NV, 80 mg/day for 4 days followed by 40 mg/day for 3 days and 20 mg/day for 3 days) was started on day 2 after admission. Lidocaine venous infusion (lidocaine .2 g + normal saline 250 mL/day) or acupuncture treatment was added for patients with severe tinnitus. The treatment course was 7 to 10 days. A post-treatment hearing test was conducted before discharge. Treatment efficacy was determined according to the criteria of the sudden hearing loss guidelines. 2 Pure tong average improvement in the affected frequencies <15 dB was defined as ineffective recovery, ≥ 15 dB but <30 dB as effective recovery, and recovery to normal levels as complete recovery. 2 All patients were followed up for more than one month after discharge.
Statistical Analysis
SPSS 25.0 was applied for statistical analysis. All data were presented as x ± s. ANOVA was used in comparisons among multiple groups and followed by Bonferroni post-test. The F-test was used in comparisons between groups, the independent samples t-test for inflammatory indicators between patients and normal controls, and the χ2 test for comparison of treatment efficacy among patients with different audiogram shapes and was followed by partitions of χ2 test for post-test. An ROC (Receiver Operating Characteristic) curve between inflammatory index and prognosis was analyzed by bivariate correlation. A P-value of <.05 was considered statistically significant.
Results
Comparison of General Clinical Data
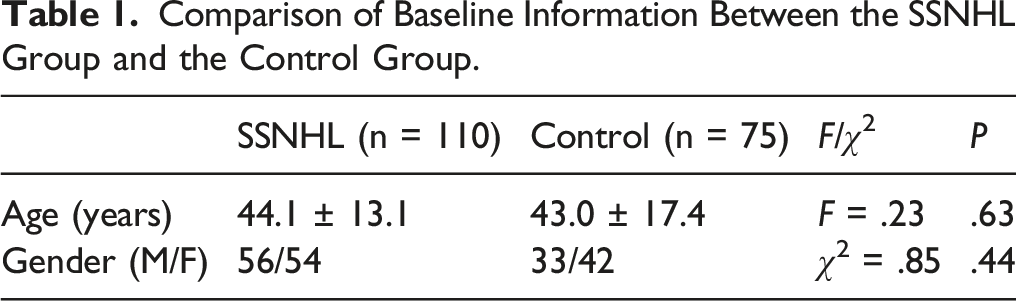
Comparison of Baseline Information Between the SSNHL Group and the Control Group.
Comparison of Baseline Information among 4 Subgroups of SSNHL Patients (n = 110).

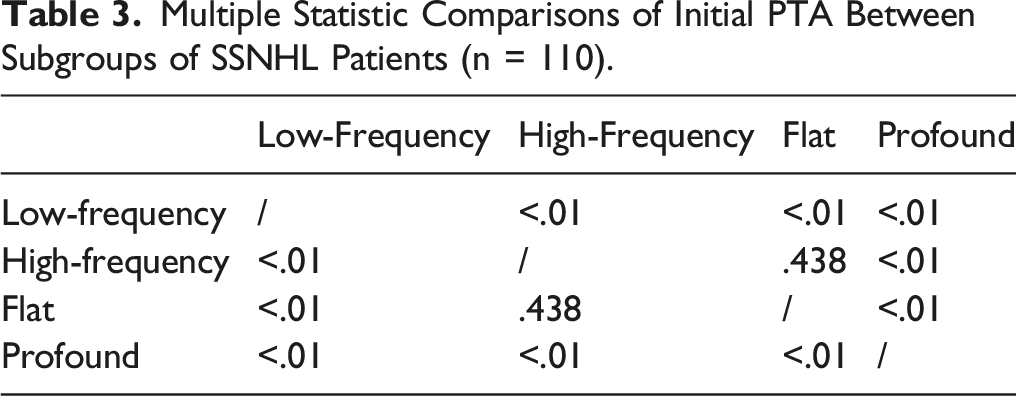
Multiple Statistic Comparisons of Initial PTA Between Subgroups of SSNHL Patients (n = 110).
Comparison of Treatment Efficacy Among Hearing Loss Subgroups
Of the 110 patients, effective recovery was observed in 75 patients, while ineffective recovery was seen in 35 patients. Therefore, the total effective efficiency was 68.2%. Consistent with a previous report,
3
the best recovery was observed in patients with low-frequency hearing loss, and the worst was in patients with profound hearing loss. Significant differences were observed in total treatment efficiency among the 4 subgroups (χ2 = 11.86, P = .008), as well as between the low-frequency and flat subgroups, and between the low-frequency and profound subgroups (all P < .01). Significant differences were observed in the complete recovery rates among the 4 subgroups (χ2 = 23.09, P < .01), as well as between the low-frequency and high-frequency subgroups, between the low-frequency and flat subgroups, and between the low-frequency and profound subgroups (all P < .01, Figure 1). These results may indicate that not only the degree of hearing loss but also the range of damage in the cochlea affects treatment effects. Comparison of treatment efficacy in SSNHL patients with different audiogram shapes. The highest recovery rate was observed in patients with low-frequency hearing loss, while the lowest was in patients with profound hearing loss. Significant differences were observed between the low-frequency and flat subgroups, and between the low-frequency and profound subgroups (** all P < .01). Significant differences were observed in the complete recovery rates between the low-frequency and high-frequency subgroups, between the low-frequency and flat subgroups (** all P < .01), and between the low-frequency and profound subgroups (*** P < .001).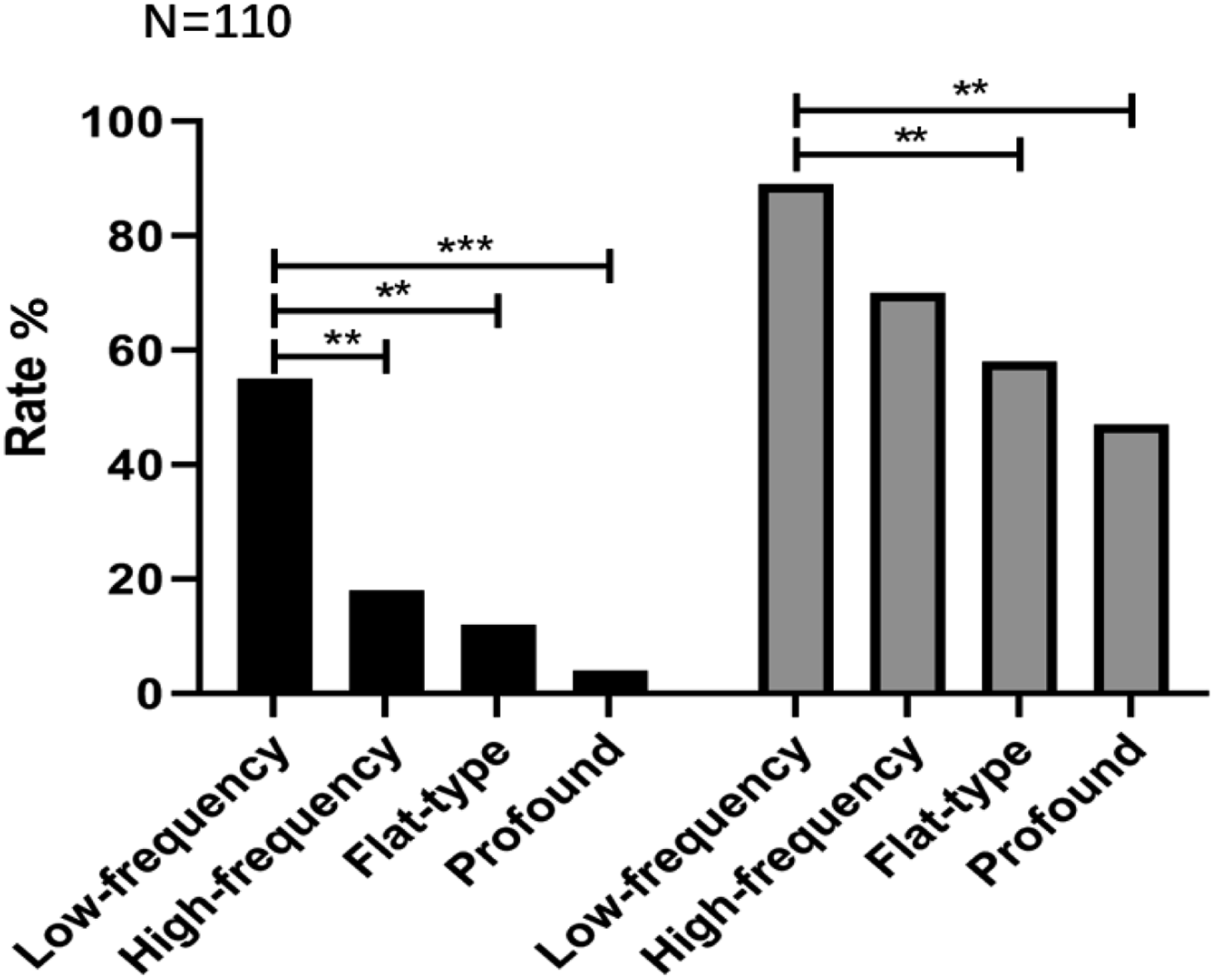
Comparison of Inflammatory Indices in SSNHL Patients and the Control Group
Comparison of NLR, PLR, MLR, and SII Between the Hearing Loss Subgroups and the Control Group.
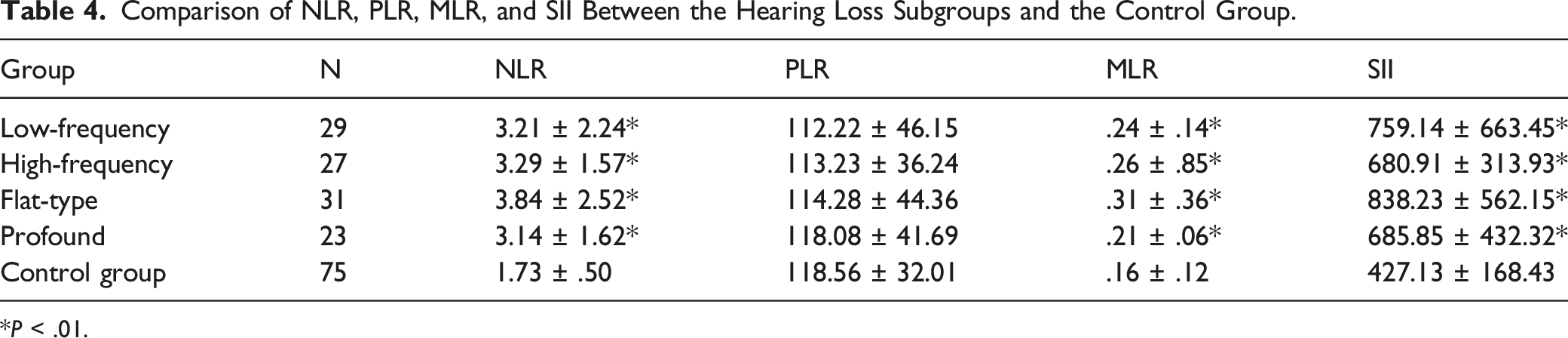
*P < .01.
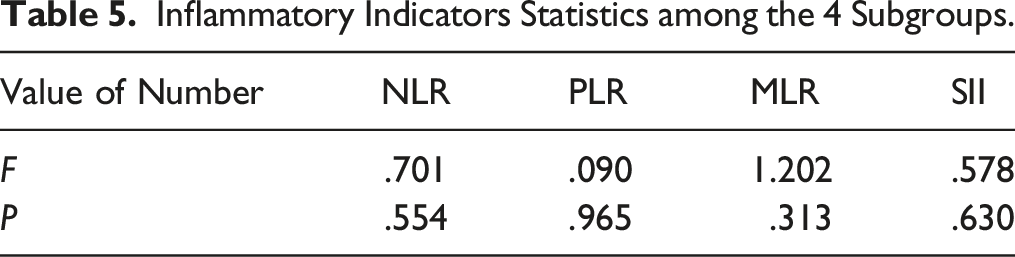
Comparison of Each Inflammatory Indicator Among the Four Subgroups
Inflammatory Indicators Statistics among the 4 Subgroups.
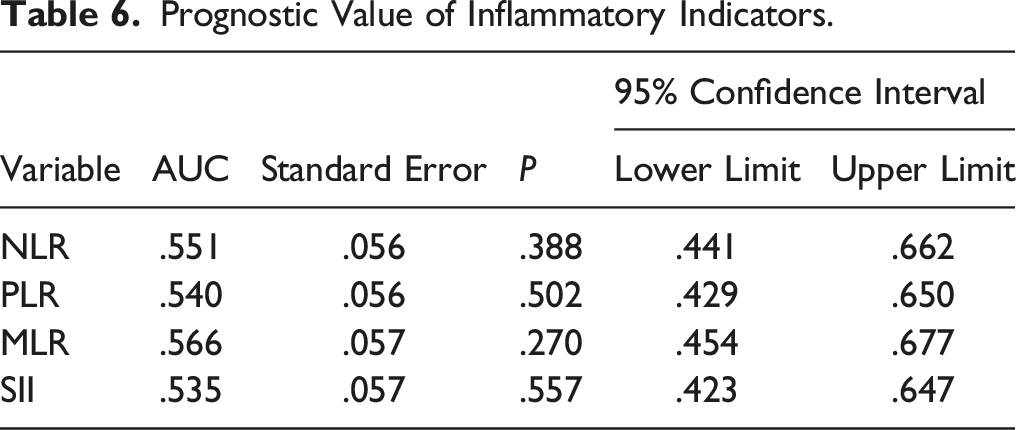
Predictive Value of Inflammatory Indicators in SSNHL
Prognostic Value of Inflammatory Indicators.
Discussion
The etiology of SSNHL remains unknown in the majority of patients, and therefore their hearing loss is still classified as idiopathic. Numerous hypotheses about the pathogenesis of idiopathic SSNHL have been proposed. The most popular and widely accepted theories include vascular compromise, 15 cochlear membrane rupture, 16 viral infection,17,18 and autoimmune responses.19,20 Therefore, identifying potential causes in each individual patient may help to develop personalized treatments. Use of peripheral blood indicators to study inflammatory and immune responses in SSNHL patients has been reported in recent years.21-23 The advantages of these hematological markers include that they are convenient and cheap and the results are available almost immediately. Other more expensive and inconvenient biomarkers, such as DNA (such as GRHL2), RNA (miR-183), proteins (prestin), autoantibodies, and metabolites, have also been reported in SSNHL patients.24-26
It is well known that NLR and MLR are associated with inflammatory activity, and SII plus NLR and PLR may indicate vascular endothelial injury, atherosclerosis, and local microartery inflammation.27,28 In the present study, regardless of the audiogram shape, all SSNHL patients had elevated white blood cells, neutrophils, and monocytes, as well as higher NLR, MLR, and SII compared to normal controls. These results indicate immune and inflammatory responses may be involved in all SSNHL patients regardless of the hearing loss levels and frequencies involved.
Platelet-to-lymphocyte ratio has been used as a marker for peripheral arterial occlusion diseases such as arteriosclerosis and arterial thrombosis. 29 High PLR was reported in SSNHL patients.6,27 However, in the present study, all patients had a normal PLR indicating vascular compromise, such as cochlear artery embolism or thrombosis, may not be a major pathogenesis in SSNHL. The current results also suggest that immune and inflammatory responses in the cochlea may be a common pathophysiology to all SSNHL patients.
Some studies found that NLR was more closely related to the prognosis compared to PLR.27,30,31 Most previous studies demonstrate higher NLR and PLR levels may indicate poor prognosis.27,30,31 However, in one previous study, elevated NLR and PLR may have indicated a better prognosis to SSNHL patients with up-sloping audiograms and mild hearing loss. 6 In the present study, we have not found any prognostic value of these indicators in SSNHL. All patients, recovered or non-recovered, had similar levels of NLR, PLR, MLR, and SII. Therefore, these markers might be not suitable for predicting the prognosis of SSNHL.
Consistent with previous studies,9,22,27,28 we found the audiogram shape and the degree of hearing loss were closely related to the prognosis of SSNHL. In the present study, about 1/4 of patients who had low-frequency and mild hearing loss had the best recovery. About 1/5 of patients who had profound hearing loss had the worst recovery, indicating the audiogram shape and the degree of hearing loss predict the prognosis. The profound hearing loss group might have broad and profound damage in the cochlea. 32
Other biomarkers have also been used in SSNHL patients. Wang and his colleagues have reported that serum levels of NLRP3, Caspase-1, IL-6, and TNF-α were negatively correlated with the prognosis of patients with sudden deafness. They also observed significant differences among patients with different audiogram shapes. 33 These results suggest that NLRP3, Caspase-1, IL-6, and TNF-α may be better markers than the markers we used in reflecting the inflammatory status in the inner ear in SSNHL patients. Activated NLRP3, the inflammasome in cochlear immune cells, induces IL-1β secretion in the cochlea. This pathway could be a common pathological basis of multiple inner ear diseases, including SSNHL. 34 Therefore, more studies are needed to address the prognostic value and pathophysiological functions of these biomarkers in SSNHL patients in the future.
In the present study, we retrospectively analyzed peripheral blood inflammatory indicators in SSNHL patients with different audiogram shapes. Unfortunately, only pre-treatment data was available in these SSNHL patients and the follow-up period was short. Therefore, prospective studies with larger sample sizes and longer follow-up period are needed in the future.
Conclusion
Elevated NLR, MLR, and SII may indicate the involvement of immuno-inflammatory responses in all SSNHL patients.
Footnotes
Acknowledgments
The authors would like to thank Drs. Xiaoping Du and Zachary Yokell in Hough Ear Institute, USA, for critically reviewing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Funds of China (81670931), Nanjing Medical Science and Technology Development Key project (ZKX-21012) and Special Fund for Clinical Research of Nanjing Drum Tower Hospital (2022-LCYJ-MS-01).
Ethical/Consent Statement
Written informed consent was obtained from all the participants prior to the enrollment of this study.