
Abstract
The simultaneous occurrence of congenital ossicular anomalies and congenital cholesteatoma (CC) is exceedingly rare. This report describes the case of an 11-year-old boy who presented with conductive hearing loss, characterized by an average air conduction threshold of 50 dB in the left ear, without any prior otologic history. Preoperative assessments suggested the presence of CC, with suspicion of ossicular chain malformation. The patient underwent ear endoscopic surgery, during which the lesion was excised, and the ossicular chain was reconstructed using a titanium ossicular prosthesis. Postoperative follow-up indicated successful healing, with a significant improvement in hearing, as demonstrated by a reduction in the air conduction threshold to 15 and a hearing gain of 35 dB.
Introduction
Congenital cholesteatoma (CC) is a collection of keratinizing squamous epithelia medial to an intact tympanic membrane (TM), without a history of otorrhea, perforation of the TM, or previous otologic surgery, and it may have been present at birth. 1 Due to the lack of otologic symptoms, it can grow in the temporal bone for a long time without being detected and is prone to misdiagnosis and missed diagnosis in clinical practice. It may occur independently or in combination with other ear anomalies. The concurrent occurrence of CC and congenital ossicular anomaly is extremely rare. Only a few cases of CC together with middle ear ossicular malformation have been reported in the English language literatures,2-7 and almost all patients undergo microscopic surgery with a conventional retroauricular incision. Small intratympanic cholesteatoma and ossicular malformations are very suitable for endoscopic surgery. Here, we present a case of CC with stapes malformation through endoscopic surgery, in which CC was prone to be misdiagnosed as tympanic sclerosis, and ossicular chain malformation was almost missed diagnosed. Simultaneously, a review of pertinent literature was conducted.
Case Report
An 11-year-old boy with a 6-month history of hearing loss in the left ear was referred to our hospital. He had no history of otitis media, otorrhea, vestibular dysfunction, trauma, tinnitus, or other otologic symptoms. Otoscopic examination revealed a grayish-yellow irregular mass behind the anterior quadrant of the left TM (Figure 1A), while the external auditory canal was normal. Initially, the mass was identified as a calcified plaque caused by tympanic sclerosis at first glance. A pure-tone audiogram revealed conductive hearing loss, with an average air conduction (AC) threshold of 50 dB on the left side (Figure 1B). The CT scan showed some flocculent soft tissue densities in the anterosuperior region of the mesotympanum (Figure 1C to F). Endoscopic surgery of the left ear was performed under general anesthesia. A transcanal skin incision was made and the tympanomeatal skin was elevated. For the sake of better visulazation, the TM was elevated from the malleus handle and the umbo. We observed that the lesion was not cystic but an “open” or rather a whitish irregular shape clump in the anterosuperior of mesotympanum, part of it located behind the malleus handle (Figure 2A). After removing the whitish clump, a small lump of a cholesterol granulomatous-like substance was found ahead, which was also dissected together. The lesion did not extend to the posterior superior quadrant of the middle ear and thus did not have direct contact with the stapes. Both the anterior and posterior arches of the stapes are missing, leaving only the stapes tendon connected to the remaining stapes head. The incus was removed (Figure 2B) and a total ossicular prosthesis (TORP) was placed on the floor of the stapes to reconstruct the ossicular chain (Figure 2C), with a small tragus cartilage placed on top. Histopathology confirmed a cholesteatoma. A postoperative endoscopy revealed intact TM (Figure 2D). A hearing test revealed an improvement in hearing to 15 dB with a hearing gain of 35 dB (Figure 2E).
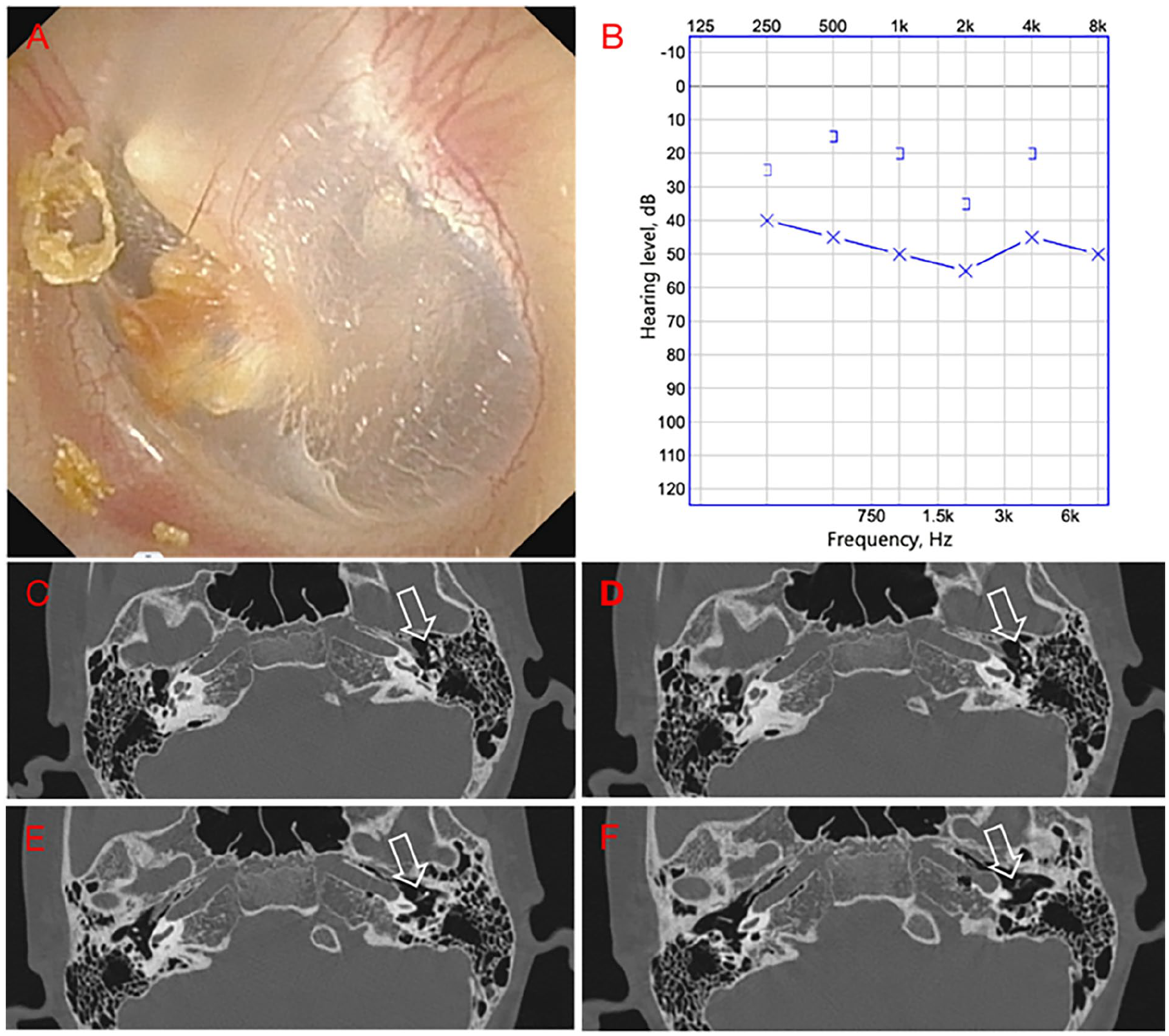
(A) Preoperative endoscopic findings. (B) Preoperative PTA showed conductive hearing loss. (C-F) Densities of flocculent soft tissue in the anterosuperior of mesotympanum (open arrow). PTA, pure tone audiometry.
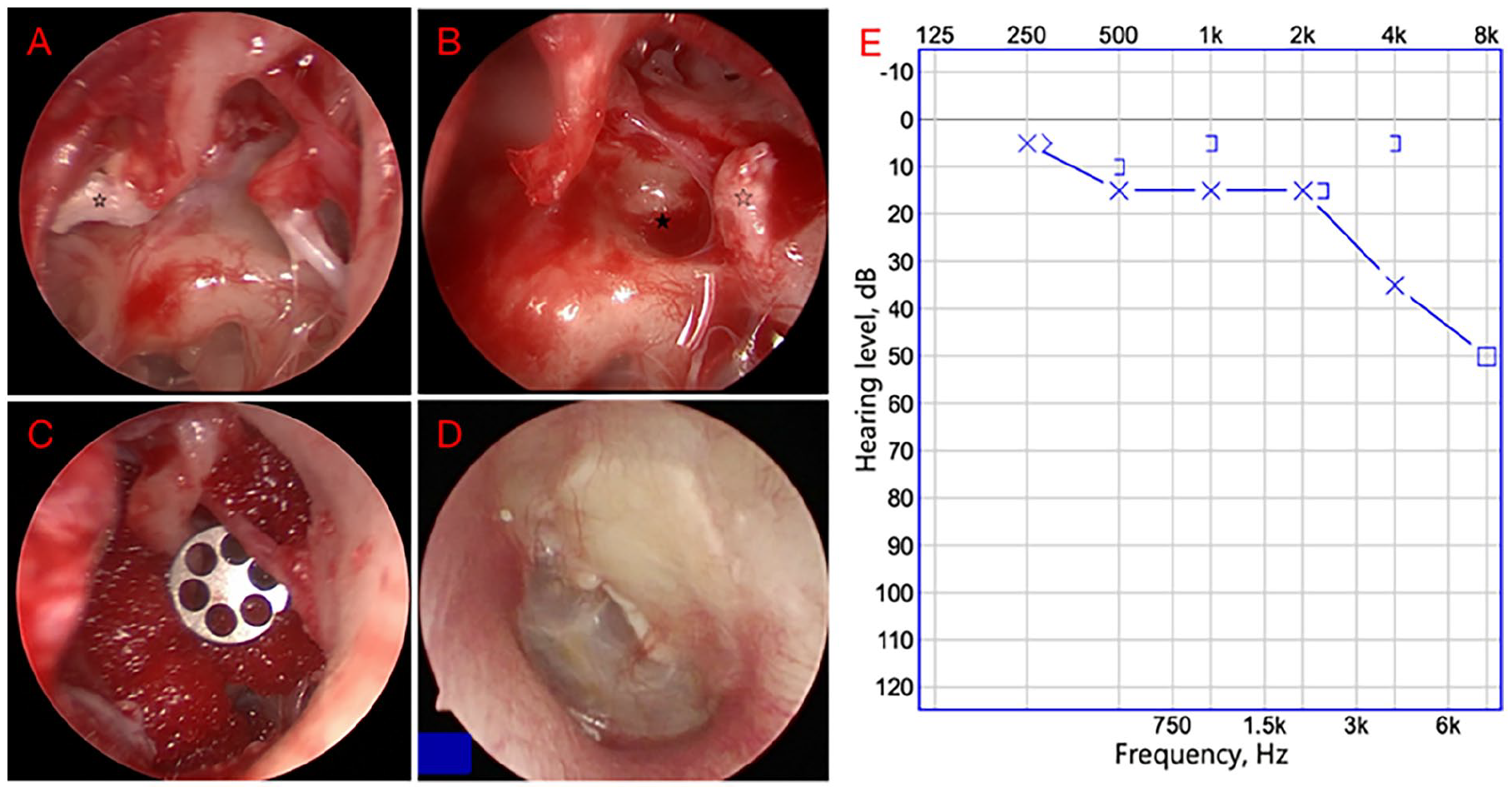
(A) Irregular-shaped keratinized epithelium in the anterosuperior of the mesotympanum (open asterisk). (B) Footplate without suprastapedial structure (solid asterisk) and stapedius tendon (open asterisk). (C) A TORP placed on the stapes floor. (D) Postoperative endoscopy showed intact TM (at 6 months follow-up after the operation). (E) Postoperative PTA demonstrated an improvement in hearing level. TORP, total ossicular prosthesis; TM, tympanic membrane; PTA, pure tone audiometry.
Discussion
CC is a rare disease, accounting for 2% to 5% of all cholesteatomas. 8 In the pediatric population, the incidence of CC is 0.12 per 100,000 children. 9 However, the incidence may have been underestimated, because compared to acquired cholesteatoma in adults with offensive otorrhea and hearing loss, pediatric cholesteatoma is relatively silent. 10 The mean age at diagnosis is 4 to 5 years. 11 Younger children often overlook the symptoms of unilateral deafness, while some even have no otologic symptom, including deafness. The patient in this case had unilateral deafness during adolescence and sought medical attention. A detailed ear examination is necessary, but interestingly, the otoscopic examination in this patient showed that the lesion behind the intact eardrum was not a common round pearl-shaped white mass, but rather a grayish yellow soft tissue shadow with irregular edges. This even led the trainee who performed the patient’s otoscopy to mistakenly believe that it was a calcified plaque in the eardrum caused by tympanic sclerosis. According to Kodama’s report, the absence of a closed cyst shape may be due to spontaneous rupture of the intact pouch, which can lead to complete involution of the lesion. 12 This is such an obscured situation; therefore, a high level of suspicion must be maintained to avoid misdiagnosis and missed diagnosis. In this rare case, we report that an irregularly shaped cholesteatoma mass behind the TM, unlike the typical pearl-shaped round cholesteatoma mass, needs to be differentiated from the calcified plaques of the TM caused by tympanic sclerosis. If this case was misdiagnosed as tympanic sclerosis, conservative treatment may be adopted, which could exclude the possibility of further surgical treatment.
Research on temporal bone pathology has shown that there are 2 different types of CC. 13 The first type of CC is usually located in the anterosuperior quadrant as a localized cystic shape, and the ossicular chain is usually not affected. Surgery for this type is relatively simple, and the hearing loss is small, usually less than 20 dB. 14 The second type is open and extensive. The keratinized epithelium often forms part of the tympanic mucosa, and extends toward the mesoposterior tympanum, and development gradually affects the attic and sinus. In this type, the ossicular chain is usually eroded, mainly at the incus stapes joint, often leading to worse conductive deafness, with hearing loss greater than 30 dB. 15 Based on preoperative ear endoscopy and CT examination, this case is the first type of CC. The disproportionate aspect lies in the degree of hearing loss. The preoperative hearing of 50 dB AC did not match the extent of the lesion, which implied that there may be other signs of a disrupted ossicular chain. Preoperative CT showed that the extent of the cholesteatoma did not protrude into the posterior superior quadrant of the tympanic cavity, which was confirmed during surgery.
The cholesteatoma did not directly contact with the incus and stapes intraoperatively, implying that the absence of suprastapedial structure was due to congenital malformation of the ossicular chain instead of being destructed by the cholesteatoma. Based on the literature on ossicular malformations without CCs,16-19 the most common discontinuity of ossicular anomalies is the absent or underdeveloped long process of the incus and the superstructure of the stapes. The average preoperative AC threshold was between 45 and 60 dB, depending on the degree of mobility of the stapes footplate. A mean hearing gain of 20 to 30 dB was achieved after surgical reconstruction of the ossicular chain. In our case, the ossicular anomaly was the absent of the superstructure of the stapes. The preoperative AC was 50 dB, the postoperative AC was 15 dB, and the hearing gain was 35 dB. These clinical features shared great similarities with those of the previous literature on ossicular malformations, further justifying the congenital nature of the ossicular defects in our case, instead of being destroyed by cholesteatoma.
Conclusion
CC in children is a relatively concealed lesion, and the possibility of CC should be promoted as a matter of awareness of when a mass shadow is found behind the TM. An atypical CC mass behind the TM needs to be differentiated from calcified plaques of tympanic sclerosis. CC of the middle ear can damage the ossicular chain and cause hearing loss. However, if the extent of CC is localized and the AC and bone conduction difference is disproportionately large, the concurrence of ossicular chain anomaly should also be considered.
Footnotes
Acknowledgements
We would like to acknowledge Dr Baolu Jiang for general guidance and providing clinical materials.
Authors Contributions
Haiping Qin data collection and manuscript preparation; Jinxia Xu manuscript preparation and review; Qingli Huang, Lili Gong collect pictures; all authors read and approved the final manuscript.
Availability of Data and Material
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This article was approved by the Ethics Committee of Liaocheng People’s Hospital.
Consent to Participate
Not applicable.
Consent for Publication
The patient’s guardian provided us written informed consent for the publication of this case report.