
Abstract
Malignant lesions and tuberculosis coexisting at the same anatomical site in a patient are extremely uncommon. We present a case of a 53-year-old female with cervical lymphadenitis tuberculosis combined with metastatic papillary thyroid carcinoma. Thyroidectomy was performed on the patient with central and lateral neck dissection. The patient received anti-tuberculosis medication and radioactive iodine ablation. No recurrence was observed during a 2-year follow-up period.
Introduction
Tuberculosis (TB) is a common public health disease. It is the major cause of death due to infectious illnesses. Extra-pulmonary TB in the head and neck region represents 10% of all TB cases and the most frequent sites are the cervical lymph nodes. 1
Cancer is also a worldwide menace. Thyroid cancer is responsible for 1% of all malignant tumors and 0.2% of all cancer fatalities.2,3 Papillary thyroid carcinoma (PTC) is the most common histological subtype of thyroid cancer.
Cervical lymphadenopathy in TB can imitate lateral metastasis of the neck from papillary carcinoma of the thyroid 4 and frequently lead to over-processing. Malignant lesions and tuberculosis coexisting at the same anatomical site in a patient are extremely uncommon. 2
Tuberculosis should be considered before deciding to perform a neck dissection in cases of PTC. Fine needle aspiration (FNA) is effective in diagnosing cervical TB.
Case Report
A 53-year-old female presented with a history of a left supra-clavicular mass that had been progressing for 2 months. Physical examination revealed a painful indurated 2 cm mass in the left supra-clavicular region with 2 enlarged bilateral jugular-carotid lymph nodes.
Ultrasound of the neck found an EUTIRADS IV-classified and 7 mm right thyroid nodule with multiple bilateral enlarged lymph nodes at levels II, III, VI, and Va (Figure 1). CT scan demonstrated the right thyroid nodule with bilateral lymph nodes and no signs of tracheal invasion (Figure 2). FNA was performed from the right thyroid nodule and 1 enlarged lymph node. Cytological analysis revealed a suspicious aspect of malignity classified as Bethesda V and a non-contributive result from the lymph node. Based on the cytology, the patient underwent a right lobo-isthmectomy with right central neck dissection. The extemporaneous histological examination revealed a PTC with recurrent right metastasis. Hence, we completed with a thyroid totalization, right central neck dissection, and selective bilateral lateral cervical lymph node dissection at levels III, IV, and V.
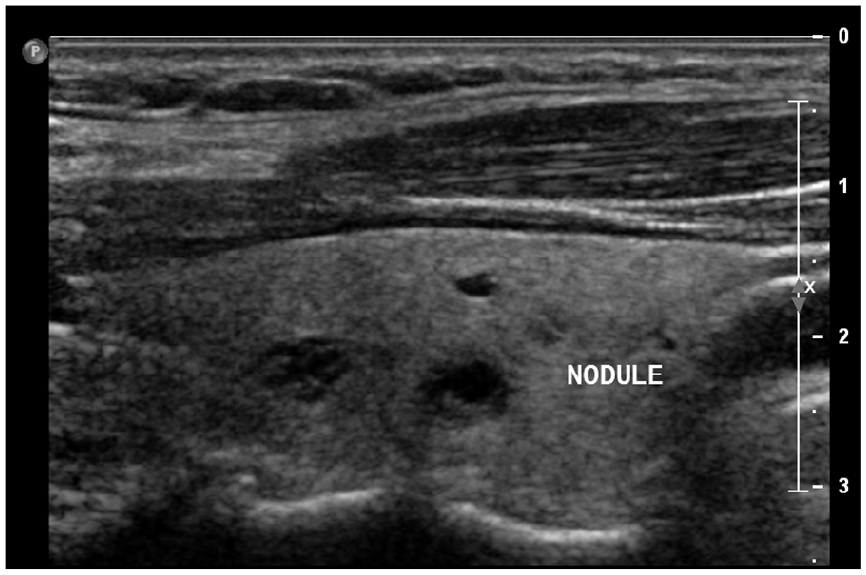
Ultrasonography showing the right thyroid nodule.
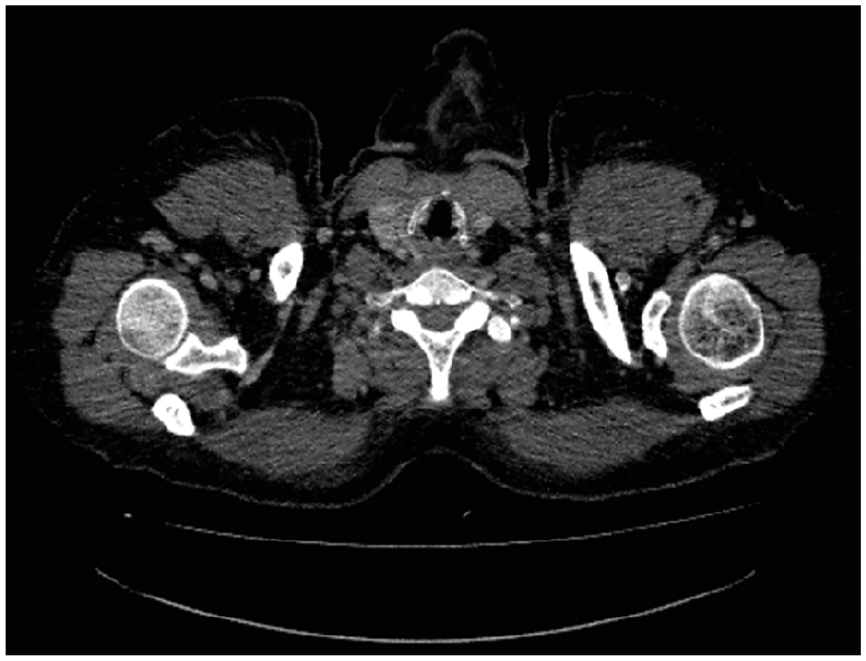
Axial CT scan demonstrating right thyroid nodule with cervical lymphadenitis tuberculosis.
The definitive histological examination confirmed PTC of the right lobe with 4 lymph nodes presenting metastasis with no extranodal extension (levels III, IV, and VI right side), while 5 lymph nodes presented tuberculosis (Figures 3 and 4). The pathological stage of pT1aN1b was determined.
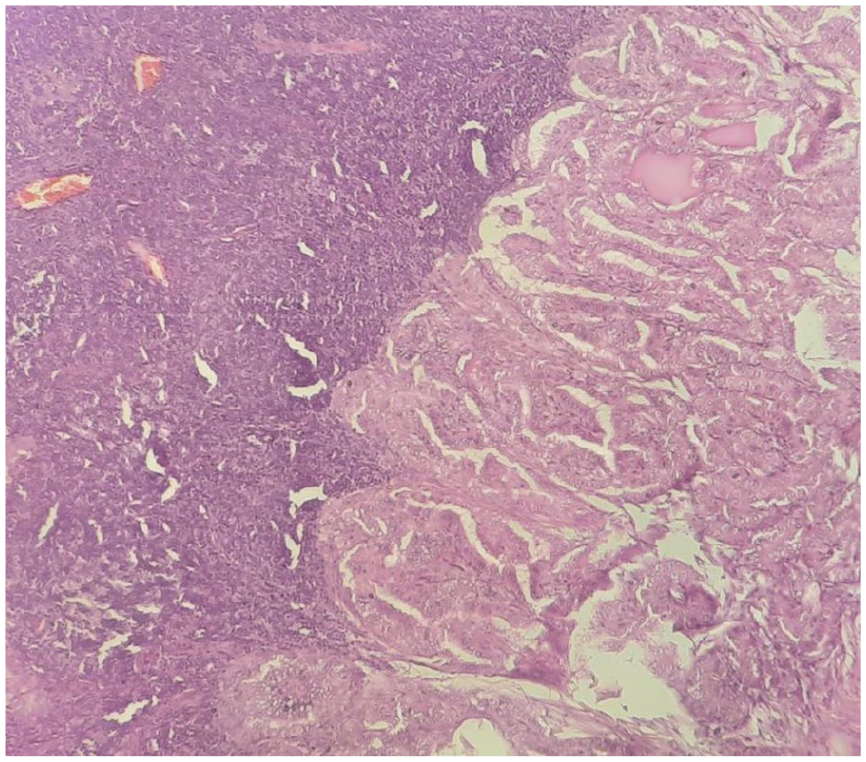
Lymph node metastasis of papillary thyroid carcinoma.
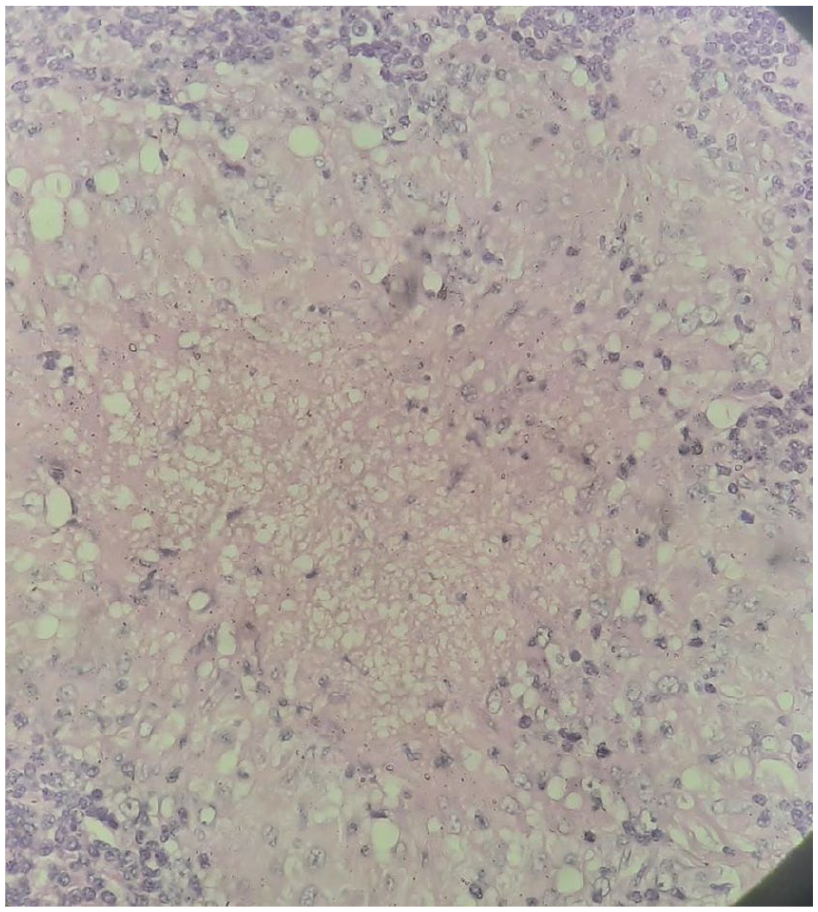
Tuberculosis-related caseating granulomas in lymph nodes.
Following surgery, there were no postoperative complications. The anti-tuberculosis medication was introduced 2 weeks after surgery for 6 months and the patient received radioactive iodine ablation. After 2 years of follow-up, no recurrence of thyroid cancer or tuberculosis was noted.
Discussion
Extra-pulmonary TB in the head and neck region represents 10% of all TB cases and the most frequent sites are the cervical lymph nodes. 1 Thyroid gland TB is uncommon with a frequency of 0.1% to 0.4%. 3 The majority of thyroid gland TB with cervical nodes are diagnosed as metastatic thyroid cancer preoperatively. Thus, proper preoperative evaluation is necessary to avoid unnecessary treatment. Cancer and tuberculosis tend to be similar in clinical, biological, and radiological terms. 5 Yet, a preoperative diagnosis is not easy due to the poor performance of imaging techniques and their failure to discriminate between metastatic lymph nodes resulting from PTC and those caused by TB lymphadenitis.3,4 Ultrasonography findings are similar for cervical TB lymphadenitis and cervical lymph node metastasis of PTC, including the presence of calcifications, cystic changes, and hypoechoic mass.4,6 Therefore, fine needle aspiration cytology with PCR finds its place and it is considered the only method for the diagnosis of TB preoperatively.1,3 FNA is effective in diagnosing cervical TB with a sensitivity of 46% to 90%.1,4,6
At the same time, people with TB are more likely to develop cancer.5,7 At least 2.2 million cancers globally occur each year as a result of pathogens infectious. According to a systematic review and meta-analysis by Luczynski et al, the combined overall risk of cancer after tuberculosis was SIR 1.62. 7 Pathogenic bacteria have been shown to modify and exploit the human host cell niche in various ways during their infection cycle. 5 Oncogenesis can be promoted by chronic inflammation and bacterial toxins, in particular by increasing circulating levels of tumor necrosis factor-alpha (TNF-α) that act as tumor initiators.5,7 In addition, TB activates the nuclear factor-B pathway and exhibits an anti-apoptotic effect on DNA-damaged cells. 8 Tuberculosis-infected macrophages produce epiregulin that stimulates the proliferation of surrounding normal epithelial and stromal cells. 8
In parallel, cancer also leads to the development of TB. It can be caused directly by decreasing immune function or indirectly by the second effects of its treatment such as chemotherapy, radiotherapy, and immunotherapy. Therefore, immunosuppression increases the risk of reactivation of latent or new TB infections. 9 A systematic review and meta-analysis by Dobler et al found that patients with solid organ cancers had an approximately 2-fold increased risk of TB compared to controls. 7
Treatment decisions can be quite complicated when cancer and TB coexist. Hirashima et al reported that concomitant cancer chemotherapy and anti-tuberculosis can be safe and effective. 10 The treatment of TB lymphadenitis is anti-tuberculosis medication while it is neck dissection in metastatic PTC. As cervical tuberculosis commonly emulates neck metastases, vigilance is required during preoperative assessment in advance to avoid over-processing and minimize the different complications associated with neck dissection. 6 A study elaborated by Iqbal et al found that approximately 72% of patients with cervical lymphadenopathy with PTC were due to tuberculosis. 6
Conclusion
It is important to acknowledge the fact that TB disease and cancer coexist, and both of them have the potential to contribute to the development of the other, hence the importance of preoperative evaluation to ensure the optimum treatment.
Footnotes
Author Contributions
H.C. was a doctor in charge of a patient, initiated the study, and wrote the manuscript. A.H. was a doctor in charge of a patient and wrote and edited the manuscript. Y.S. wrote and edited the manuscript. S.B.R. was the doctor who specialized in histopathology and performed the microscopic examination. S.T. wrote and edited the manuscript. All authors read and approved the final manuscript.
Consent for Publication
Written informed consent for publication of the patient’s clinical details and clinical images was obtained from the patient.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its figures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The ethics approval is not required for case reports deemed not to constitute research at my institution “Hospital of FSI Tunis, Tunisia.”