
Abstract
Primary thyroid lymphoma is rare. Hashimoto’s disease is usually found as a risk factor. Among thyroid lymphoma, diffuse large B-cell lymphoma (DLBCL) is the most aggressive and frequent one. A 56-year-old man with a medical history of Hashimoto’s disease presented with a neck mass and dysphonia. A computed tomography scan revealed a large thyroid mass. Fine-needle aspiration cytology (FNAC) was consistent with lymphoma, confirmed by a core needle as a DLBCL. The patient was transferred to the Department of Hematology and Oncology for chemotherapy with good results. Primary thyroid lymphoma accounts for less than 5% of all thyroid gland malignancies and less than 2% of extranodal lymphomas. It frequently affects women in the sixth or seventh decade. Hashimoto’s disease is a major risk factor. DLBCL is the most common histological subtype with aggressive evolution. Radiology and FNAC are not usually very precise and a biopsy is needed. Treatment includes surgery, radiotherapy, chemotherapy, and targeted therapy.
Introduction
Thyroid involvement in lymphoma is a rare occurrence accounting for 1% to 2% of extranodal lymphomas. Thyroid lymphoma is divided into 2 categories: primary thyroid lymphoma affecting the thyroid gland first, before spreading, and secondary thyroid lymphoma affecting the lymph nodes and other organs first, before spreading to the thyroid gland. Given that, the thyroid is not a lymphoid organ; a lymphoplasmacytic infiltrate appears to be a prerequisite for the development of thyroid lymphoma, as observed in Hashimoto’s thyroiditis. 1
Case Report
A 56-year-old man with a medical history of type 2 diabetes and Hashimoto’s disease presented with a 2-week history of neck mass and dysphonia. He was found to have a non-tender anterior neck swelling fixed to the surrounding structures and without skin changes (Figure 1A and B). Thyroid blood tests were normal on levothyroxine. Neck computed tomography (CT) scan revealed a large thyroid mass (Figure 1C). Ultrasound-guided fine-needle aspiration cytology (FNAC) was consistent with lymphoma, confirmed by a core needle biopsy which showed a morphological appearance and immunohistochemical profile consistent with diffuse large B-cell lymphoma (DLBCL). In fact, histological examination revealed massive infiltration of the thyroid tissue by a population of round large lymphoid cells with visible nucleoli and scarce cytoplasm, foci of necrosis were noted. Immunohistochemical studies were carried out and showed that tumor cells were diffusely immunoreactive to CD20 (Figure 2). Chest and abdominal CT scans were without other findings. Hence, the assigned Ann Arbor classification was IE. Moreover, the patient was transferred to the Department of Hematology and Oncology for 6 courses of chemotherapy (R-CHOP: rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) with good results.
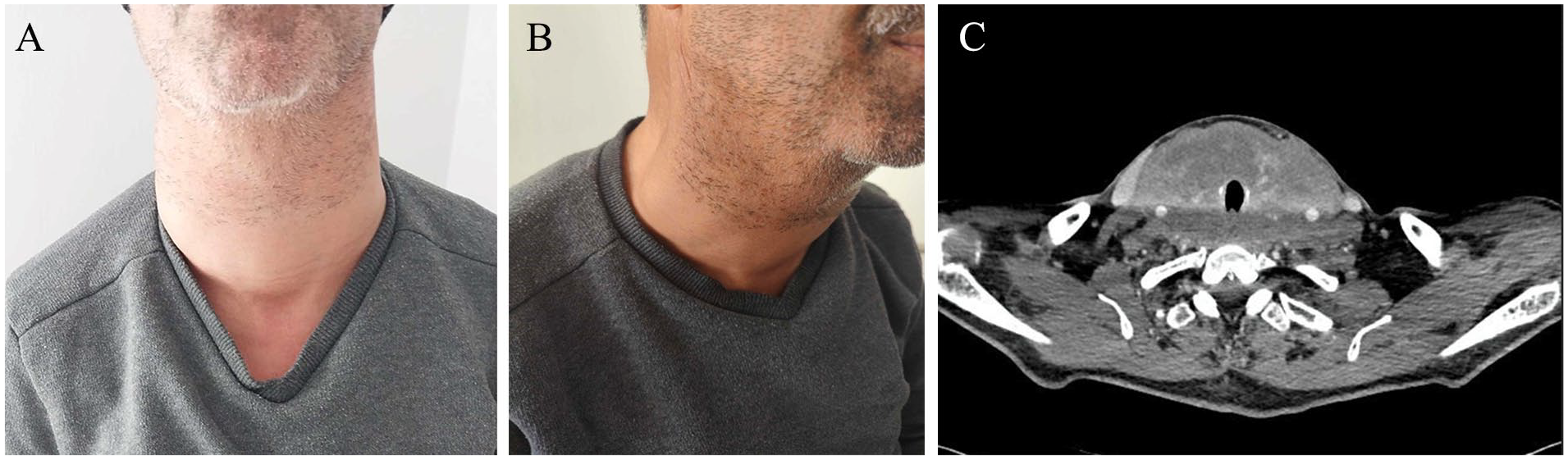
(A and B) Anterior neck swelling. (C) Axial CT of the neck shows a thyroid enlargement.
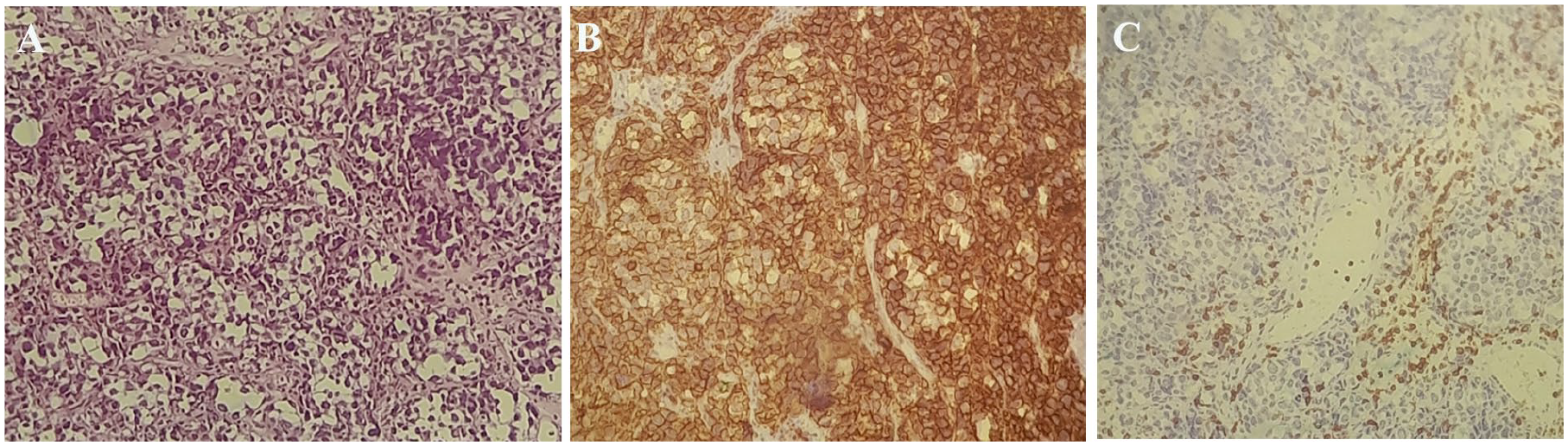
(A) Diffuse proliferation of round large lymphoid cells on the H&E stain. (B) Lymphocyte proliferation is positive for the CD20 marker on the immunohistochemical stain. (C) Lymphocyte proliferation is negative for the CD3 marker on the immunohistochemical stain.
Discussion
Primary thyroid lymphoma accounts for less than 5% of all thyroid gland malignancies and less than 2% of extranodal lymphomas, making it an infrequent disease. It affects women more frequently, especially in the sixth or seventh decade. Hashimoto’s disease is a major risk factor. 2 Patients with Hashimoto’s disease are at least 60 times more likely to develop thyroid lymphoma than healthy patients. Such an association may be attributable to chronic antigenic stimulation paving the way for malignant transformation. No additional factors have been linked to thyroid lymphoma. 3
DLBCL is the most common histological subtype (70%), followed by mucosa-associated lymphoid tissue (MALT) lymphoma (10%-20%), then follicular lymphoma, lymphocytic lymphoma, Hodgkin’s lymphoma, and T-cell lymphoma.2,4,5 Unlike MALT lymphoma, which has an indolent course, DLBCL is more aggressive and rapidly progressive. In addition, MALT lymphoma can transform into DLBCL, giving a mixed form that is just as aggressive as pure DLBCL. 2
Thyroid lymphomas tend to present as a neck swelling (>70% of the cases). This enlargement can progress rapidly, particularly in cases of DLBCL, with anaplastic thyroid carcinoma as the differential diagnosis. Compression signs may be associated in one-third of the patients, such as dyspnea, dysphonia, and stridor. As well as general signs (10%-20%) such as weight loss, night sweats, and fever.2,3,6,7
Primary thyroid lymphoma is often accompanied by a normal thyroid function. Hypothyroidism is observed in 10% of cases, secondary to coexisting Hashimoto’s disease or diffuse infiltration of the thyroid gland by tumor cells. Rarely, patients may develop hyperthyroidism as a consequence of the destruction of thyroid follicles releasing thyroid hormones into the circulation. 3
Radiographic features of thyroid lymphoma are not specific and similar to those of other primary malignant thyroid tumors and Hashimoto’s thyroiditis. Ultrasonography is a basic examination for thyroid enlargement. Some researchers have found features frequently associated with thyroid lymphoma, such as hypoechogenicity, enhancement of posterior echoes, the absence of microcalcifications, linear echogenic septations, and associated Hashimoto’s disease.8-11 Full body CT scan is required for staging according to Ann Arbor classification. 3
If lymphoma is suspected, an FNAC is performed to guide the diagnosis which can be confirmed by core needle biopsy or surgical biopsy. 12 Although FNAC is widely used for thyroid masses, it has limited use for lymphomas and variable accuracy since the identification of the lymphoma subtype by immunohistochemistry cannot be carried out with FNAC. 13 FNAC accuracy can be improved using flow cytometry, immunoperoxidase studies, and polymerase chain reaction. 14 The increasing use of ultrasound-guided core biopsy for accurate diagnosis has led to a reduction in the necessity for surgical procedures. Nevertheless, an open surgical biopsy may still be required not only to confirm a definitive diagnosis but also to ascertain the specific subtype of lymphoma when other less invasive procedures fail. 14
Treatment options vary considerably from one pathological subtype to another. The main treatment modalities include surgery, radiotherapy, chemotherapy, targeted therapy, and combination therapies. The core purpose of surgery is to establish a definitive diagnosis and relieve pressure on the respiratory tract. The main treatment for DLBCL, as it is an aggressive lymphoma, is combination therapy based on monoclonal antibody rituximab, chemotherapy (cyclophosphamide, doxorubicin, vincristine, and prednisone), with radiotherapy.3,15-17 MALT lymphoma, on the other hand, has an indolent course, and radiotherapy alone can be adequate.18,19
Overall prognosis depends on pathological subtype, staging, and age. DLBCL has a worse prognosis compared to MALT lymphoma. Stages III and IV of Ann Arbor classification and age >60 years have a poor prognostic.7,20
Conclusion
Hashimoto’s thyroiditis is a well-documented risk factor for thyroid lymphoma. DLBCL are characterized by their rapid progression and significant compressive symptoms. A biopsy is the gold standard for confirming the diagnosis and enables immunohistochemical and molecular analysis, which is necessary for subsequent therapeutic management.
Footnotes
Author Contributions
Makram Tbini: Writing – Original draft. Salma Bessioud: Writing – Original draft. Oumayma El Mabrouk: Writing – Original draft. Rihab Laamouri: Writing – Review & editing. Meriem Ksentini: Writing – Review & editing. Ahlem Blel: Data curation. Mamia Ben Salah: Supervision.
Consent
Written informed consent for publication of the clinical details and images was obtained from the patient.
Data Availability
Data used during this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Case reports are exempt from ethical approval at our institution.