
Abstract
The pyramidal lobe is an anatomical component of the thyroid gland seen in up to 65% of individuals. It represents the distal, nondegenerate part of the thyroglossal duct. The double pyramidal lobe is a very rare occurrence, and this is the first reported case in Sri Lanka. A 40-year-old woman presented a long-standing goiter. Her evaluation revealed a benign multinodular goiter with a dominant right colloid nodule and background thyroiditis. She was euthyroid and had no compressive symptoms. Considering cosmesis, the patient opted for total thyroidectomy during which two pyramidal lobes were identified. The rest of the thyroid gland and the parathyroids had no anomalies. After an uneventful postoperative stay, she was discharged later. This is a very rare case where the patient had two separate pyramidal lobes; a phenomenon documented in less than 10 cases around the world. In addition to embryology, the pyramidal lobe has significance in clinical practice. It can be associated with benign and malignant disease of the thyroid; focal and diffuse. Incomplete removal may result in recurrence of the disease in the remaining thyroid tissue of the pyramidal lobe. Therefore, active inspection of the lobe including its anatomy during thyroid surgery and complete excision when indicated is of paramount importance.
Introduction
The thyroid gland is an endocrine organ housed in the anterior neck within the pretracheal fascia. 1 It consists of two lobes; left and right, an interconnecting isthmus, and in up to 65% of cases, a pyramidal lobe (PL). 2 It represents the distal end of the thyroglossal duct which develops along the migratory path of the thyroid gland during fetal development. 3
The thyroid gland begins to develop at the base of the tongue in the third week of gestation. The thyroid diverticulum migrates caudally in the midline, anterior to the hyoid bone and laryngeal cartilage to rest in the anterior neck at level with the C5–T1 vertebrae. During its descent, the gland is connected to the base of the tongue through the thyroglossal duct. By the tenth week of intrauterine life, the thyroglossal duct degenerates by apoptosis, leaving only the foramen cecum as a souvenir of its existence at the base of the tongue. In some cases, complete obliteration of the duct does not occur leaving remnants along its tract; the most common being the pyramidal lobe. 4
Although PL is commonly encountered in surgery and imaging, double PL is extremely rare; very few cases have been reported worldwide and none from Sri Lanka. We present the first documented case of double PL in Sri Lanka that was incidentally identified during surgery. Figure 1
Thyroid gland with the double pyramidal lobe.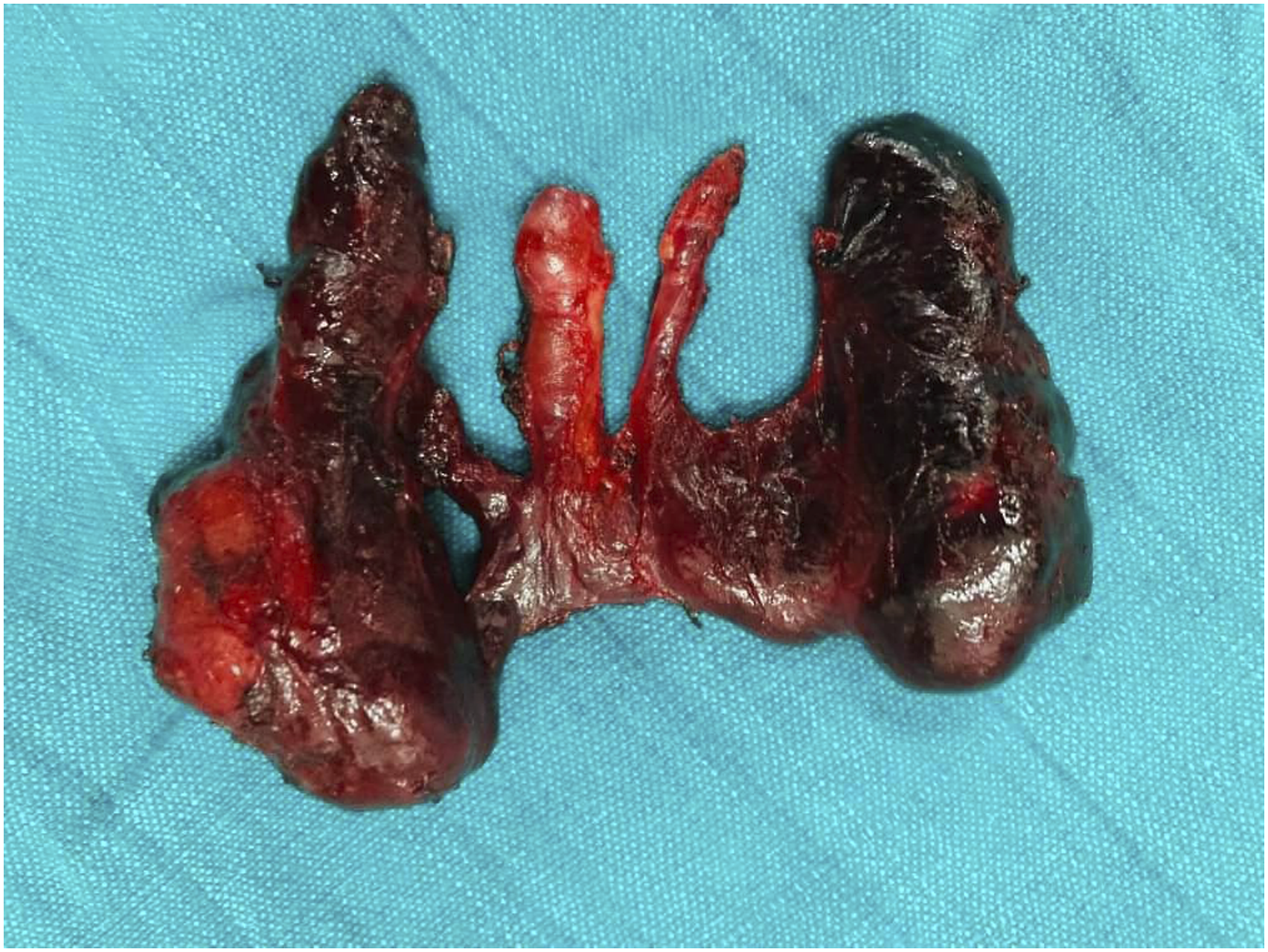
Case Report
A 40-year-old woman with a long-standing goiter underwent a clinical examination. She had a multinodular goiter (MNG) with a dominant nodule in the right lobe. There were no signs of obstruction of the upper aerodigestive tract, nor was there cervical lymphadenopathy. She was clinically and biochemically euthyroid. Ultrasonography revealed a benign MNG with background thyroiditis without anatomical anomalies of the gland. Fine needle aspiration (FNA) revealed a colloid nodule. The patient had no comorbidities and no other complaint. Considering cosmesis, she opted for a total thyroidectomy Intra operative image depicting the double pyramidal lobe.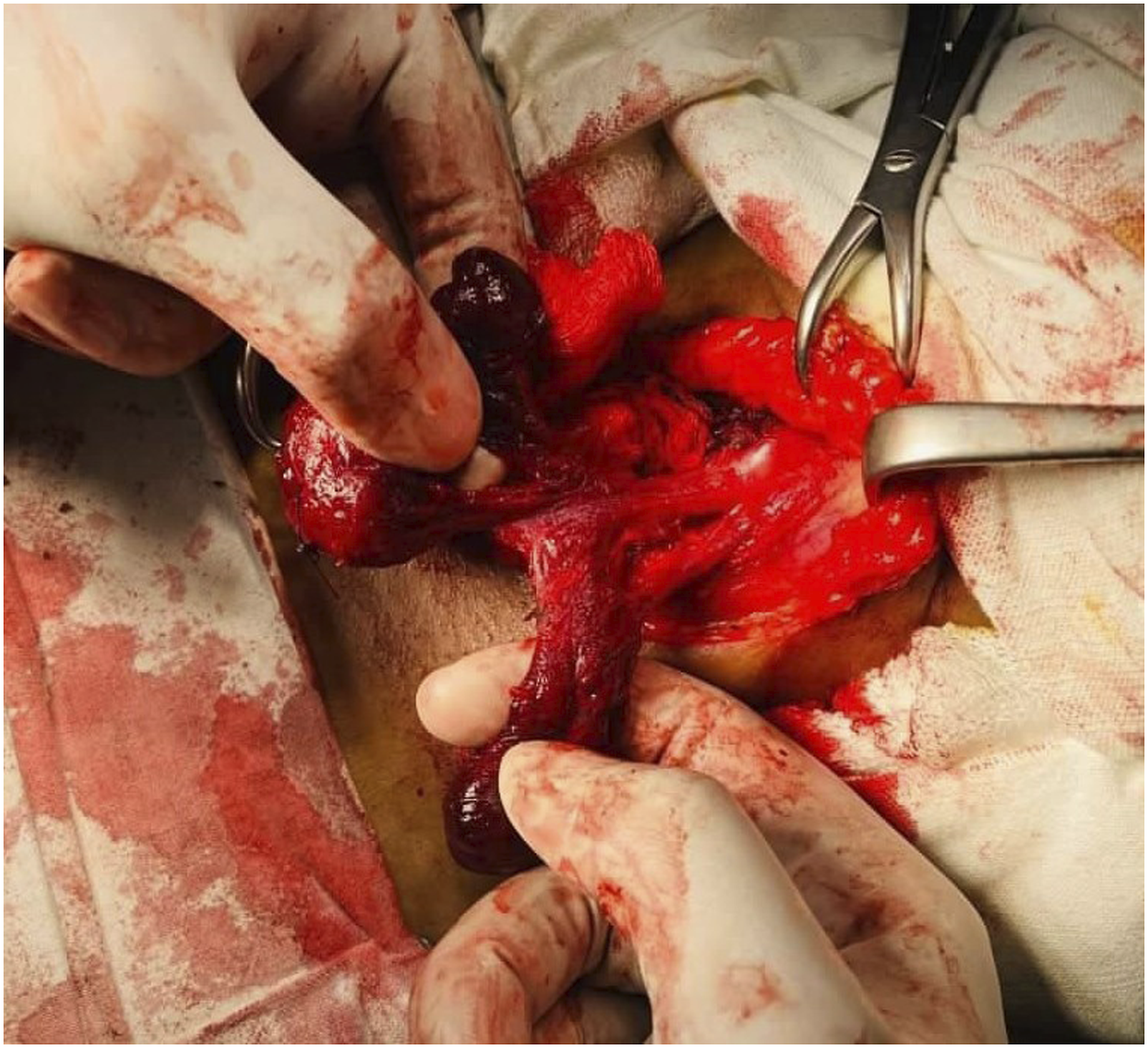
During surgery, two separate pyramidal lobes arising from the thyroid isthmus were observed, extending toward the hyoid bone on either side of the thyroid cartilage. No other anatomical variations were observed in the thyroid or parathyroid glands, nor was a thyroglossal cyst present. After mobilizing the two lobes, the isthmus along with the two pyramidal lobes was excised en bloc. Figure 2
Discussion
From an embryological point of view, PL is considered a developmental anomaly. But data collected from imaging and thyroid surgery have shown that PL is found in up to two-thirds of all individuals. On the basis of the latter, many consider it to be an anatomical component of the thyroid gland.
5
Several studies have reported various anomalies related to PL.3,6,7 Variations in position, connection to the rest of the gland, and its size have been documented.3,6,7 However, double PL has only been documented in fewer than 10 reports worldwide, and this is in fact the first such case reported from the island of Sri Lanka, emphasizing the rarity of its occurrence.2,5,7 Figure 3
Thyroid gland with the double pyramidal lobe after fixation.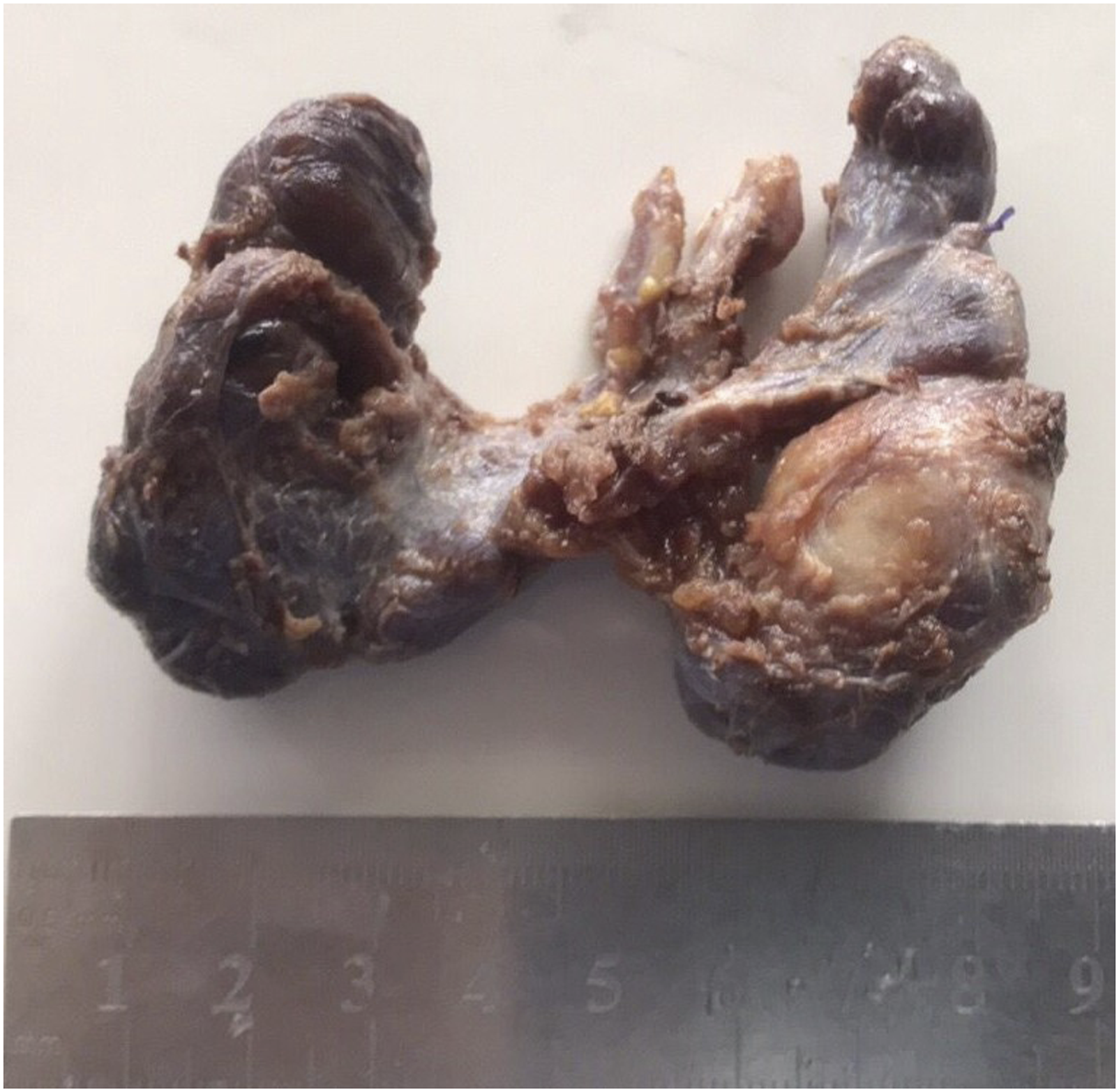
In addition to its implication in anatomy and embryology, PL has several clinical implications. PL can be the site of benign disease as well as malignancy. It is more commonly involved in diffuse than focal thyroid pathologies.2,8 Few cases of primary thyroid carcinoma and recurrent cancers involving PL have been reported.2,3,9,10 Incomplete removal of PL makes disease recurrence a probable complication.8,10 Failure to remove the PL can reduce the efficacy of postsurgical radioiodine ablation after differentiated thyroid carcinoma. Residual thyroid tissue in the PL consumes most of the radioisotope, reducing its concentration to ablate the remaining thyroid bed.2,5,8 This emphasizes the importance of actively looking for PL and its anatomical variations in all cases of thyroid surgery and complete excision when indicated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.