
Abstract
Malignant melanoma originating from the sphenoid sinus is an extremely rare but aggressive tumor of the head and neck. A 57-year-old man had a 1 month history of headache, right trigeminal paresthesias, and upper lid ptosis. Magnetic resonance imaging showed a large mass in the right sphenoid sinus and an invasion of the right cavernous sinus and clivus. The patient underwent endoscopic endonasal transsphenoidal surgery, and pathologically revealed malignant melanoma. One month after the operation, the patient was treated with radiation therapy. Unfortunately, the patient died of distant metastasis 2 years later. Due to its rarity, there is still no effective treatment strategy and no way to assess the progression of malignant melanoma.
Introduction
Melanocytes are neural crest cells derived from the embryonic period, which are normally found in human skin, mucosa, and uvea. 1 Melanocytes are the source of malignant melanomas, and approximately 20% of melanomas (skin and mucosa) originate in the head and neck, and only 1% arise from the sinonasal tract, and it is extremely rare to originate from the sphenoid sinus. 2 The commonly affected areas include the nasal cavity, maxillary sinus, ethmoid sinus, and frontal sinus. 3 As we all know, most malignant melanomas of the sphenoid sinus are diagnosed at a late stage due to the lack of clinical symptoms in the early stages. The common clinical symptoms are nasal obstruction and epistaxis. 4 The treatment of melanoma is mainly surgical and usually supplemented by radiotherapy or immunotherapy.5,6 Malignant melanoma originating from sphenoid sinus is extremely rare and only a few reports have been reported previously.7-11 Therefore, we report a case of primary malignant melanoma arising from the sphenoid sinus.
Case Report
A 57-year-old man presented to the neurosurgery department of Chongqing General Hospital (Chongqing, China). He had a 1 month history of headache, right trigeminal paresthesias, and upper lid ptosis. He denied nasal obstruction and epistaxis. There was no previous history of melanoma of the skin or mucosa in other parts of the body. Chest computed tomography (CT) and abdominal ultrasonography revealed no abnormal findings. Cranial magnetic resonance imaging (MRI) showed a large mass in the right sphenoid sinus and an invasion of the right cavernous sinus and clivus (Figure 1). Further workup, there was no palpable cervical lymphadenopathy. Routine laboratory tests, including routine blood tests, and evaluation of blood coagulation function, liver, and kidney, were within the normal range. The lactate dehydrogenase (LDH) was 117 U/L (normal range 100-245 U/L). The preoperative diagnosis may be pituitary adenoma, craniopharyngioma, or chordoma. Due to the reduction of quality of life, the patient underwent endoscopic endonasal transsphenoidal surgery. Informed consent was written from the patient.
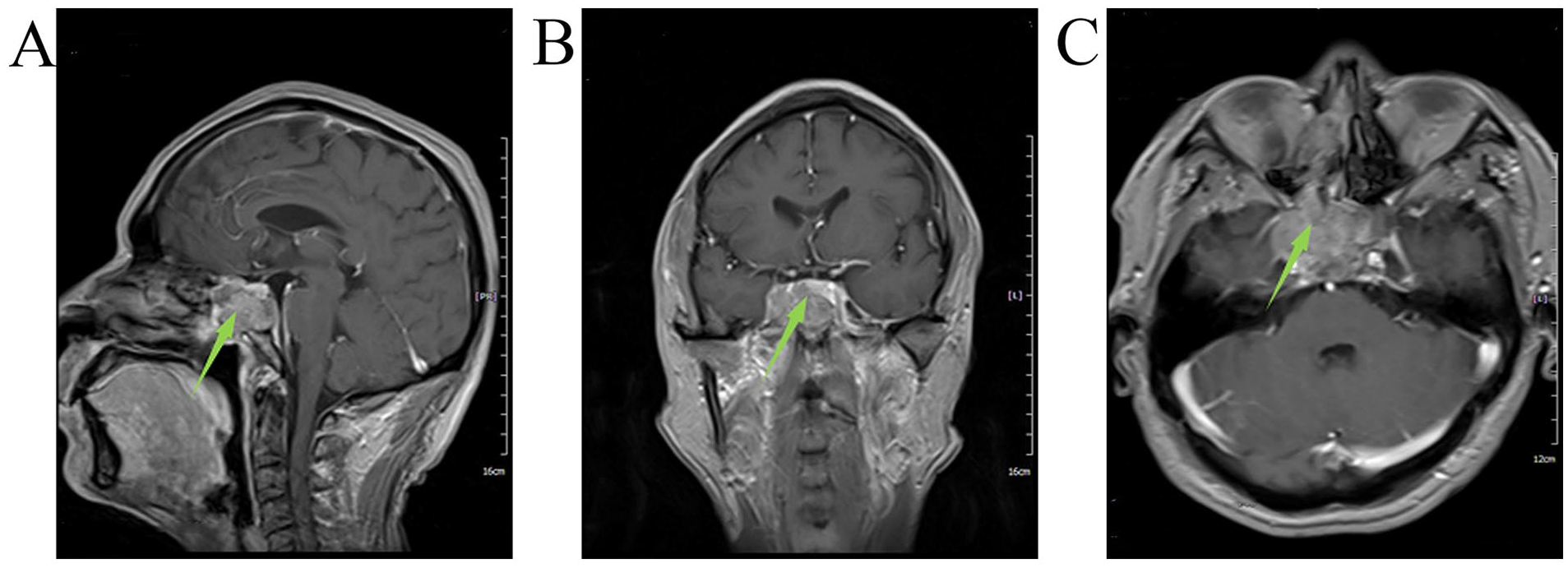
Preoperative (A) sagittal, (B) coronal, and (C) horizontal MRI. Green arrow indicates preoperative tumor. It revealed a large mass in the right sphenoid sinus and an invasion of the right cavernous sinus and clivus. MRI, magnetic resonance imaging.
After general anesthesia, the patient was placed supine position with his head slightly tilted to the right. Subsequently, an endoscope was placed along the right nasal cavity and found the opening of the right sphenoid sinus. Granulation tissue was found at the opening of the sphenoid sinus, cut the mucosa above the sphenoid sinus, and invasion of the outer wall of the sphenoid sinus. After exposing the tumor, it varied from grayish-white to dark red in color, with a rich blood supply. Removed the tumor with a curette and tumor forceps, and the deep part of the tumor invaded the clivus and sellar floor. Considering that complete resection of the tumor may lead to cerebrospinal fluid leakage, a small amount of tumor was retained at the sellar floor and achieved subtotal resection of the tumor. Finally, to prevent cerebrospinal fluid leakage, closure was achieved by a gelatin sponge and double-layered artificial meninges.
After surgery, his vital signs were stable, the headache was relieved, and right trigeminal paresthesias and upper lid ptosis still existed. According to the American Joint Committee on Cancer (AJCC) Staging Manual, the tumor’s stage belonged to stage II. On the second day after the operation, cranial MRI showed that the tumor was subtotal resection and there was no secondary intracranial hemorrhage. Routine blood tests, and evaluation of the liver, and kidney, were also within the normal range. The LDH was 109 U/L (normal range 100-245 U/L). Based on pathological examination findings, malignant melanoma was diagnosed (Figure 2). Gene mutational testing and immunotherapy were not performed due to the patient’s reluctance and financial issues. One month after the operation, the patient was treated with 60 Gy of radiation therapy in 30 fractions to the tumor bed in the oncology department. After radiation therapy, the headache disappeared and the patient was discharged. However, the patient did not attend his follow-up examinations at 3, 6, and 12 months postoperatively as required. Two years later, he returned to our department with headaches and bloating, and his abdominal CT scan showed distant metastases in his liver. As there were already multiple metastases in the liver, he had lost the opportunity for surgical treatment. In addition, the patient and his family were unwilling to actively seek treatment, and only palliative care was provided and he soon died.
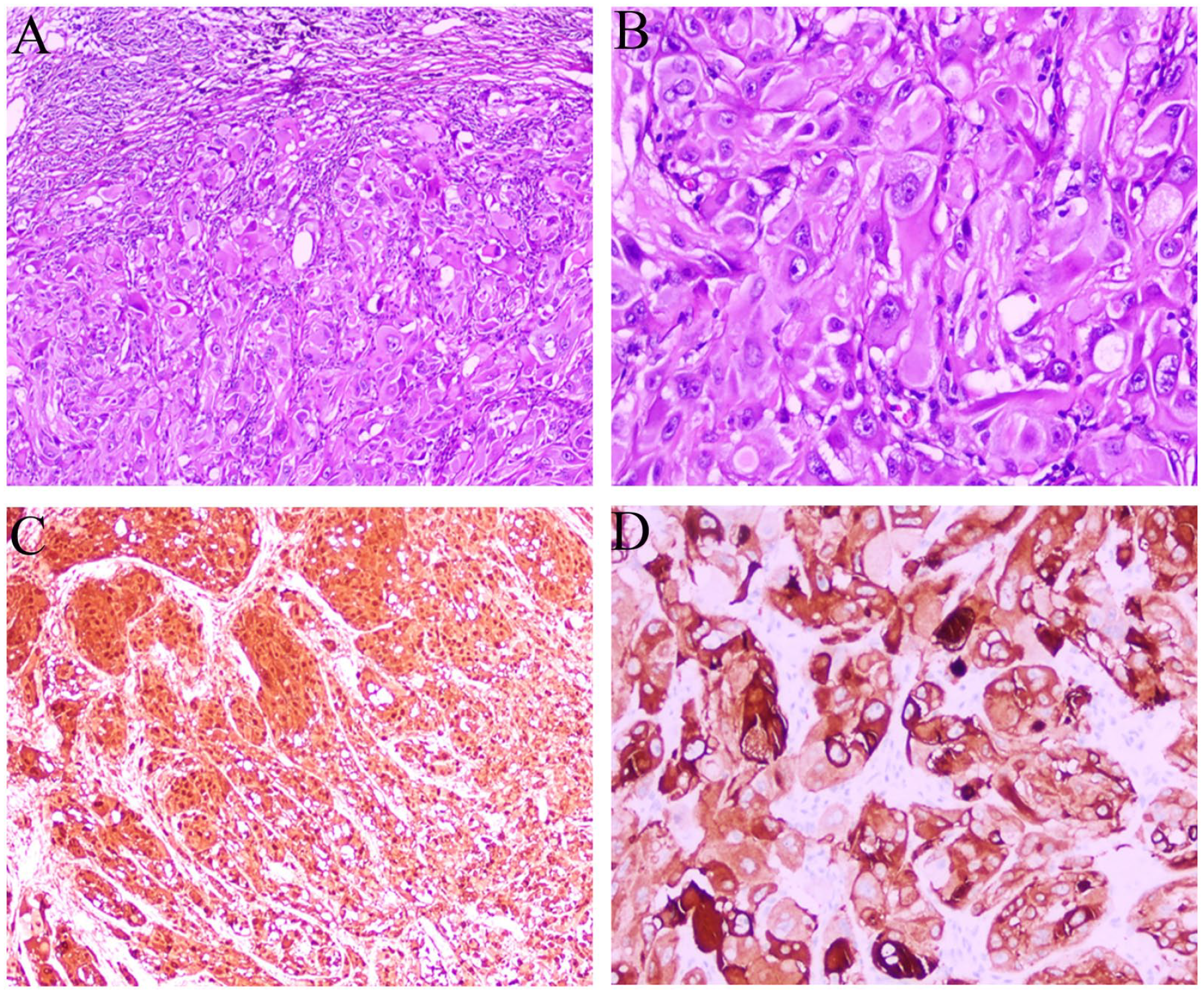
Pathological findings. (A, B) Shows HE staining, (C, D) Shows IHC staining. The pathological diagnosis was of a malignant melanoma. HE, hematoxylin-eosin; IHC, immunohistochemical.
Discussion
Melanoma remains rare in most African and Asian countries, with incidence rates commonly less than 1 case per 100,000 person-years. 12 Batsakis et al 2 reported that 0.5% to 1.5% of all melanomas originate in the nasal cavity and paranasal sinuses, and none of the 194 patients with sinonasal melanomas originated in the sphenoid sinus. Yamasaki et al 13 reported a case of malignant melanoma metastatic to the sphenoid bone. Therefore, primary malignant melanoma originating from the sphenoid sinus has rarely been reported.
Surgical resection is the treatment of choice for melanoma. Radiotherapy or immunotherapy is used as an adjuvant treatment for melanoma, there are literatures demonstrating an effect on survival and local control.14,15 Manolidis and Donald 16 reported that of the 14 cases, 10 cases received surgical treatment, 3 cases received radiotherapy, and 1 case did not receive treatment. Breik et al 17 reported that of the 8 cases, 6 cases received surgical treatment and 3 cases received radiotherapy. Tahiri et al 11 reported a 63-year-old woman who received surgical resection and adjuvant radiotherapy.
The prognosis of patients with melanoma is related to the extent of the primary tumor, the completeness of surgical resection, and the occurrence of distant metastases. Compared with skin melanoma, patients with sphenoid sinus melanoma often tend to be a worse prognosis because the tumor is usually found in the late stage. 18 It is reported the 5 year survival rate ranges from 14% to 45% for patients with head or neck mucosal melanoma,4,14,16,19,20 while the 5 year survival rate was 0% for patients with sphenoid sinus melanoma.7,10,21 In our case, the endoscopic surgical plan is guided by the extent of the disease, and radiotherapy helps prolong the survival time of patients.
In conclusion, primary malignant melanoma arising from the sphenoid sinus, due to its rarity, the treatment plans are similar to melanoma of the head and neck.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
J.L., P.W., J.W., H.J., G.Z., X.T., and N.W. participated in the conception, design and data acquisition of the article. J.L. drafted the manuscript. J.L., P.W., and J.W. revised the manuscript. NW critically revised the article. N.W. ensured that questions related to the integrity of any part of the work were appropriately investigated and resolved. J.L., H.J., G.Z., and X.T. confirm the authenticity of all the raw data. All authors read and approved the final version of the manuscript.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The Ethics Committee of Chongqing General Hospital (Chongqing, China) waived the requirement for additional ethical review, as this report is retrospective and not based on any specific patient priorities, experiences, or preferences. Informed consent for participation in the study or use of the medical data was obtained from the patient.
Patient Consent for Publication
Written informed consent was obtained from the patient for the publication of anonymized data and any accompanying images.