
Abstract
In this article, we explore the disease spectrum and clinical characteristics of and the diagnosis and endoscopic approach to treating isolated sphenoid sinus disease (ISSD) in children. To these ends, we review a case series of 19 patients (mean age: 8.1 ± 4.9 years, range: 1.1-15 years, median age: 6.7 years, 13 males, 6 females) who underwent surgical treatment at our hospital for ISSD during the 4 years between 2012 and 2016. The symptoms of pediatric sphenoid sinus disease tend to be variable and nonspecific and include atypical headache, nasal congestion, epistaxis, postnasal drip, snoring, and impaired vision. Headache is the presenting symptom in 42% of patients, but headaches occurred in no specific or typical location. Ten patients underwent preoperative endoscopic examination, and abnormalities in the sphenoethmoidal recess were found in 6 (60%) of these 10 patients. All 19 patients underwent ultra-low-dose paranasal sinus computed tomography (CT) imaging, and 9 patients with suspected tumors or sphenoid mucoceles were further examined by magnetic resonance imaging (MRI). The endoscopic transostial approach was performed in all 19 patients: 16 patients received excision of inflammatory sphenoid sinus disorders and benign tumors, including sphenoid sinusitis, sphenoid sinus mucocele, sphenoid sinus polyp, and ossifying fibroma; 3 patients with suspected tumors received biopsies to detect rhabdomyosarcoma, Langerhans cell histiocytosis, and juvenile xanthogranuloma. No intraoperative or immediate postoperative complications were observed. Children with opacified sphenoid sinus identified by radiographic imaging presented a variety of pathologies. The most common lesions were associated with inflammatory disease. Because the symptoms of pediatric sphenoid sinus disease tend to be variable and nonspecific, CT remains the standard for evaluating sphenoid sinus disease, and ultra-low-dose paranasal sinus CT imaging is recommended and can provide images of equal or better quality compared with those obtained by standard dose CT. In addition, MRI is an essential adjunct in the diagnosis and selection of treatment for suspected tumors of the sphenoid sinus. The endoscopic transostial approach was especially suitable for the management of pediatric benign isolated sphenoid sinus lesions.
Introduction
Isolated sphenoid sinus disease (ISSD) implies complete opacification of one or both sphenoid sinuses as determined by imaging studies and may be caused by a variety of pathologies. 1 Sphenoid sinus disease usually is not present in early childhood and typically is not seen until the patient is at least 3 years old. In clinical practice, ISSD in children is more rare than in adults. The symptoms of pediatric sphenoid sinus disease tend to be variable and nonspecific. Because the sphenoid sinus is located at the base of the skull, is located in a concealed position among important adjacent structures, and, especially in children, the nasal cavity is narrow, sphenoid sinus surgery in children is difficult. An appropriate endoscopic approach to open the sphenoid sinus is an effective, safe, and direct surgical method for the treatment of isolated sphenoid sinus lesions. The authors report the results of their endoscopic treatment in 19 children with isolated sphenoid disease.
Patients and Methods
Nineteen patients underwent surgery for the treatment of ISSD in the Department of Otorhinolaryngology of the Beijing Children’s Hospital between 2012 and 2016. All patients were evaluated using routine otorhinolaryngology, ophthalmology, and nervous system examinations. The preoperative examination included computed tomography (CT) scan, magnetic resonance imaging (MRI) study, and endoscopic examination. Notably, all the patients underwent the ultra-low-dose paranasal sinus CT scan, and scan data were reconstructed using a full model–based iterative reconstruction algorithm. 2
Endoscopic sphenoidotomy was performed in all 19 patients. STORZ 2.7 mm (Tuttlingen, Germany), 0° rigid endoscopes were used, along with a monitoring system and the Medtronic3000 power system, and treatment of 2 patients was assisted by use of the Medtronic FUSION electromagnetic navigation system (Louisville, USA). We decongested nasal mucosa using a 1:10000 solution of adrenaline. All 19 patients were treated via an endoscopic intranasal approach. In general, the surgeon used one of 2 ways to locate the ostium of the sphenoid sinus: The first approach is to locate the ostium of the sphenoid sinus with a superior turbinate because the natural ostium usually is present at the posterior end of the superior turbinate. 3 The other is via the posterior choana; the natural ostium typically is located approximately 1.2 to 1.5 cm superior to the roof of the posterior choana. Sixteen patients received excision of inflammatory sphenoid sinus disorders and benign tumor, including sphenoid sinusitis, sphenoid sinus mucocele, sphenoid sinus polyp, and ossifying fibroma; 3 patients with suspected tumors received biopsy to detect rhabdomyosarcoma, Langerhans cell histiocytosis, and juvenile xanthogranuloma. The technique of transostial sphenoidotomy provided direct access to the sphenoethmoidal recess without opening the posterior ethmoid sinus. The surgical approach comprised partial middle turbinectomy in 10 patients and middle turbinate lateralization in other 9 patients. After locating the ostium, the surgeon enlarged it using Kerrison forceps or a power system so that the resulting width was not less than 1 cm.
Antibiotics were given postoperatively and nasal packing was removed 2 days later. Nasal irrigation was used, nasal endoscopy was reviewed regularly, and the duration of follow-up was more than 6 months.
Results
The mean age of children with ISSD who underwent endoscopic sinus surgery was 8.1 ± 4.9 years (range: 1.1-15 years), and there were 13 boys and 6 girls. Sphenoid sinus involvement was unilateral in 16 (84.2%) patients and bilateral in 3 (10.5%) patients.
The clinical presentation of the symptoms of pediatric sphenoid sinus disease was variable and nonspecific, including atypical headache in 8 (42%) cases, all of which occurred among the patients with inflammatory sphenoid sinus disease cases, nasal congestion in 8 (42%) cases, snoring in 4 (21%) cases, postnasal drip in 4 (21%) cases, and epistaxis, decreased vision, intermittent fever, and vomiting each occurred in 1 case or 5% of the group (Table 1).
Patient Characteristics and Outcomes.
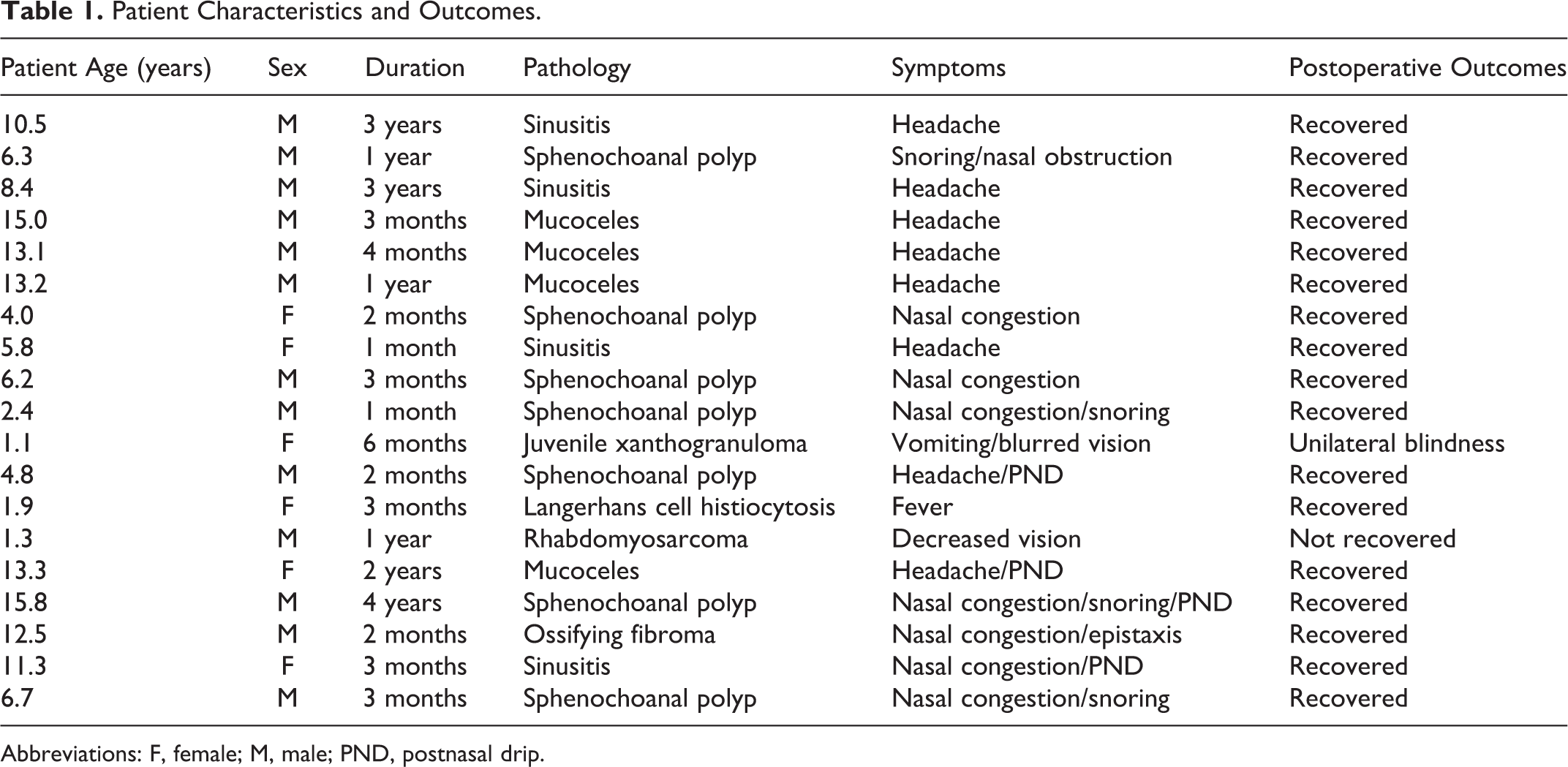
Abbreviations: F, female; M, male; PND, postnasal drip.
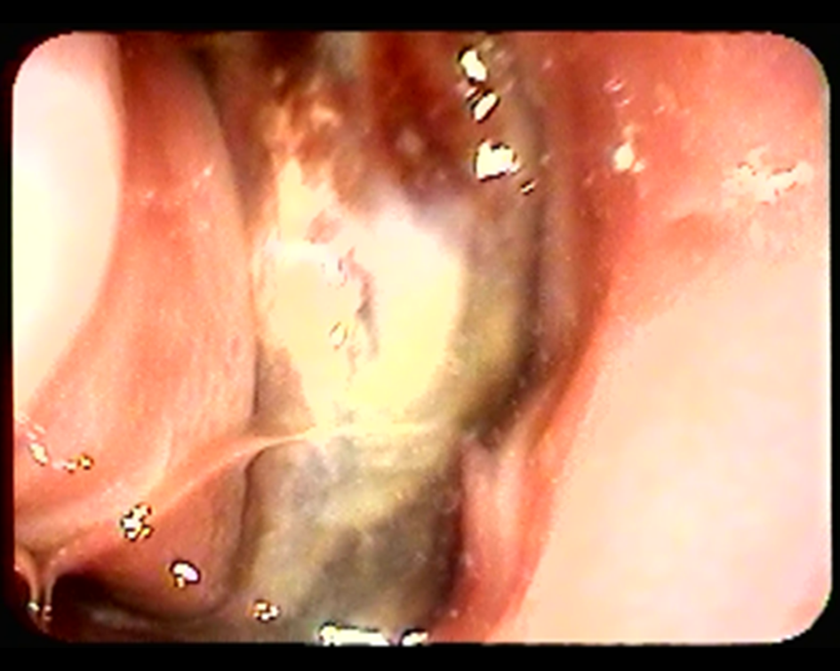
Only 10 patients underwent preoperative endoscopic examination, and the sphenoethmoidal recess showed an abnormality in 6 (60%) patients. Endoscopic examination findings included nasal polyps (Figure 1) in 5 patients and hemorrhagic crusts in 1 patient with ossifying fibroma (Figure 2). All the patients underwent ultra-low-dose paranasal sinus CT imaging, and 9 patients with suspected tumors or sphenoid mucoceles received MRI examinations. Computed tomography was the first radiologic test ordered in 16 patients who had the diagnosis of ISSD, but MRI was necessary to exclude the possibility of a malignant tumor.

Preoperative endoscopic examination showed a nasal polyp in the phenoethmoidal recess.
Preoperative endoscopic examination showed hemorrhagic crusts in the phenoethmoidal recess.
Inflammatory Sphenoid Sinus Disease
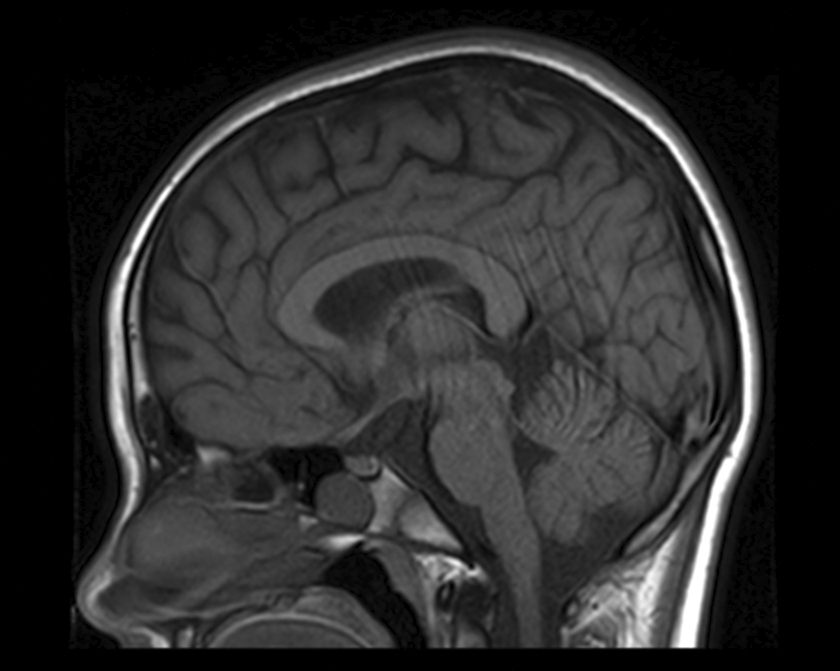
Among the 15 patients who had the diagnosis of ISSD, 4 had sphenoid sinusitis, 4 had sphenoid sinus mucocele, and 7 had sphenochoanal polyps. Table 1 summarizes the presenting symptoms and signs. There were 4 out of 8 with mucoceles, 3 out of 8 with sphenoid sinusitis, and 1 out of 8 with sphenochoanal polyp, presented with headache in various locations, including the whole head (2) and frontal (1), vertex (2), retro-orbital (1), and diffuse (2) regions of the head. The duration of the headaches ranged from 2 to 36 months (mean: 16.6 ± 15.3 months). Nasal congestion or discharge was present in 6 children who had a sphenochoanal polyp and in 1 child with sphenoid sinusitis. Postnasal drip was present in 2 children who had sphenochoanal polyp, 1 child with sphenoid sinusitis, and 1 child with mucocele. Snoring was present in only 4 children with a sphenochoanal polyp. There were no intracranial or intraocular symptoms or vision problems. The CT scan revealed a homogenous sphenoid mass without surrounding bone erosion, whereas the MRI showed a hypointense mass surrounded by diffuse hypersignal in the left sphenoid sinus with slight compression of adjacent skull bone (Figures 3 and 4). All the patients underwent endoscopic transnasal sphenoidotomy. One-year follow-up nasal endoscopy showed no evidence of relapse.

Sagittal CT of sphenoid mucocele demonstrating total opacification of the left sphenoid. No bony erosion was identified. CT indicates computed tomography.
T1-weighted MRI with gadolinium shows a hypointense mass surrounded by a diffuse hypersignal in the left sphenoid sinus with slight compression of adjacent skull bone. MRI indicates magnetic resonance imaging.
Suspected Tumors
Three patients with suspected tumors underwent biopsy: a 1-year-old boy had rhabdomyosarcoma, a 1-year-old girl had Langerhans cell histiocytosis, and a 1-year-old girl had juvenile xanthogranuloma. Two former patients received postoperative chemotherapy. Because the disease is self-limited with age, the girl who had juvenile xanthogranuloma was not given postoperative chemotherapy; this patient’s intracranial complications resolved and a 3-year follow-up MRI showed that the tumor disappeared, but intraocular complications progressed to unilateral blindness. In a 12-year-old boy with ossifying fibroma, the tumor was removed by transostial sphenoidotomy without middle turbinectomy. Postoperative imaging studies in this patient confirmed that the sphenoid sinuses had cleared and that tumor did not recur within 2 years. (Figure 5A-C.)
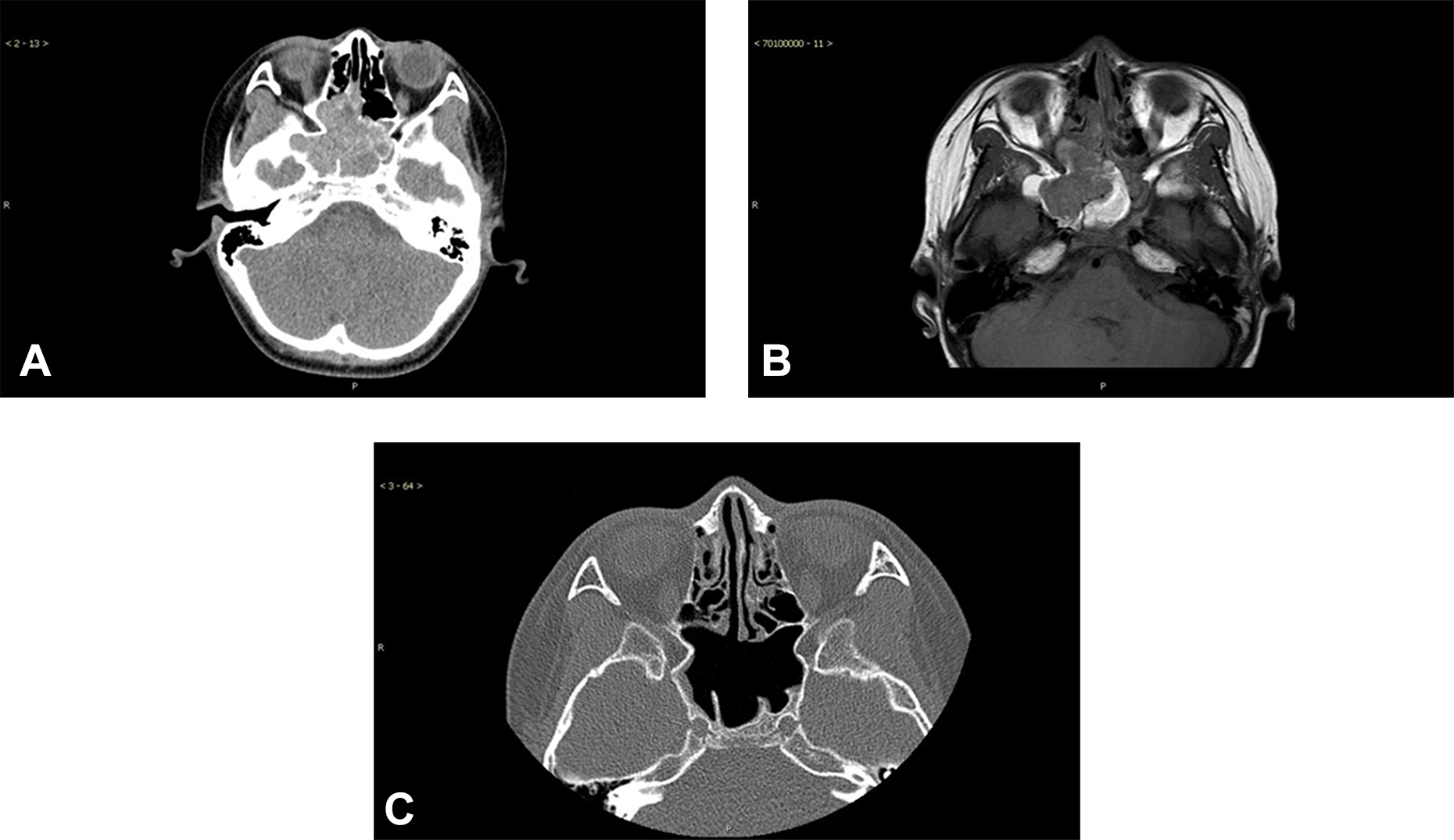
A, Axial sinus CT demonstrating total opacification of right and left sphenoid; no bony erosion was identified. B, Axial MRI showed cystiform structures and bleeding inside the opacification. C, A 6-month postoperative CT demonstrated that both sides of the sphenoid sinuses had cleared. CT indicates computed tomography; MRI, magnetic resonance imaging.
For children with suspected tumors, a bony erosion adjacent to or involving the sphenoid bone was present on all preoperative CTs. Both CT and MRI were ordered in each case, and in each of these patients, postoperative imaging studies confirmed that the sphenoid sinuses had cleared and that tumors did not recur (follow-up ranged from 2 months to 3 years).
Discussion
Classification of Sphenoid Sinus Disease in Children
Isolated sphenoid sinus disease can be broadly divided into the inflammatory, neoplastic, and miscellaneous categories. In studies of adults, infection/inflammation was the most common pathology (75%), tumors were found in 18.9%, and malignant tumors were found in 7.0%. 4 Rarely, the sphenoid sinus may be the site of metastatic lesions. 5 Castelnuovo et al found that fungal sinusitis is the most common inflammatory sphenoid sinus lesion. 6 Benign tumors included inverting papilloma, meningioma, osteoma, hemangioma, chordoma, giant cell tumor, and many other less common types. 5 Fibrous dysplasia was found to be as common as all other neoplasms according to a study by Kim et al. 7
Like adults, children who presented to our surgical service with opacified sphenoid sinus imaging on radiographs had a variety of pathologies. The most common lesion was associated with inflammatory disease, including polyps (37%), chronic sinusitis (21%), and mucoceles (21%), but there were no fungal infections in the patients studied. Among our study children, primary tumors of the sphenoid sinuses included Langerhans cell histiocytosis, rhabdomyosarcoma, juvenile xanthogranuloma, and ossifying fibroma but no metastatic lesions. These characteristics were different from those in adults who have sphenoid sinus tumors. Sphenoid sinus tumors mainly are benign and self-limited.
Clinical Signs and Symptoms of ISSD in Children
In our study, the symptoms of pediatric sphenoid sinus disease tended to be variable and nonspecific, including atypical headache, nasal congestion, epistaxis, postnasal drip, snoring, and decreased vision. There is always a particular risk that these symptoms may be ignored either by the patient or by the doctor, particularly because the various pathologic processes that affect the sphenoid sinus share many of the same characteristics. For example, headache was the most common symptom in all studies, including those in adults and children. 1,4 Localization of headaches related to sphenoid sinus disease is quite variable: The vertex, frontal, temporal, periorbital, and occipital regions are common sites. This is explained by sensory innervation of the sphenoid sinus by the fifth cranial nerve and afferent fibers from the sphenopalatine ganglion. 8 In our study, headache was the presenting symptom in 42% of cases. Headaches occurred in the whole head and vertex, as well as the retro-orbital and diffuse regions. The incidence of headache was similar among these patients, and there was no specific or typical location. Our patients experienced headaches during the 2 to 36 months (mean 16.6 ± 15.3 months) before diagnosis.
Nasal obstruction is the second most common presenting symptom of sphenoid sinus disease, according to most current literature. 6,7,9 We found nasal obstruction as well as nasal discharge and snoring were the second most common presenting symptoms in our study. In 7 patients with sphenoid sinus polyps, 6 patients had snoring symptoms, which suggested that snoring was the main complaint associated with sphenoid sinus polyps in children. Other symptoms included ocular disruptions and nosebleed. In this study, 1 case of juvenile yellow granuloma was first diagnosed on the basis of the patient’s vomiting symptoms.
Evaluation of Sinus Disease
Regarding the evaluation of sinus disease, endoscopy is a very useful tool. Rigid endoscopy of the sphenoethmoidal recess under local anesthetic has been advocated to assist diagnosis, but among adult patients, endoscopic examination detected no abnormalities in 31.2% of instances of sphenoid sinus disease. 10 Among children, rigid endoscopy generally is not well tolerated. In our series, only 10 patients underwent endoscopic examination, and the sphenoethmoidal recess included an abnormality in 6 (60%) of these patients, despite the presence of subjective symptoms. Thus, the normal appearance of the sphenoethmoidal recess does not exclude sphenoid pathology.
Hence, the initial diagnosis of sphenoid sinus pathology is usually based on imaging studies. Computed tomography remains the standard for evaluating sphenoid sinus disease because it is the most accurate way of diagnosing sphenoid sinus disease and its complications. 5 In children with sphenoid sinus disease, CT was the most common initial study, but it failed to demonstrate that disease had spread to the cavernous sinus or to the optic canal. 1 Magnetic resonance imaging is an essential adjunct in the diagnosis and selection of treatment for many lesions of the sphenoid sinus because it provides detailed images of soft tissues and plays an important role in the diagnosis of intracranial lesions.
Lawson and Reino proposed an algorithm for using CT and MRI in the diagnosis of ISSD. 11 This elegant scheme classifies the various radiologic findings noted on CT scan to better determine the correct diagnosis or to identify the need for further imaging. The purpose of this algorithm is to optimize the diagnostic value of the imaging techniques while minimizing unnecessary studies. 11 In our series, all the patients received CT scans, and 9 patients with suspected tumors and sphenoid mucoceles underwent MRI study. However, the scanning region overlaps both the sinus and the eye, and the potential damage to the vitreous body of the eye during sinus imaging is always a concern. 12 -16 In our series, all the patients underwent ultra-low-dose paranasal sinus CT imaging, and scan data were reconstructed using a full model–based iterative reconstruction algorithm. Ultra-low-dose CT imaging provided image quality that was equal to or better than that obtained with standard dose CT. 2
Endoscopic Treatment of Isolated Pediatric Sphenoid Sinus Lesions
Endoscopic transnasal sphenoid sinus surgery was first proposed at the end of the 1990s. 17 The intranasal approach to the sphenoid sinus currently comprises transostial (or sphenoethmoidal recess), transethmoidal, transseptal, and transpterygoid approaches. 18
We used the endoscopic transostial approach in all 19 patients. During the past 20 years, the transostial approach has progressively become the first-line approach for the diagnosis and treatment of ISSDs. This approach is especially suitable for the management of pediatric benign ISSD. This simple, direct approach does not violate other structures and is safe because it deals with the medial nasal part of the anterior sphenoid wall, thus avoiding injury to the optic nerve and carotid artery. Although this direct approach provides good exposure of the sphenoethmoidal recess, a partial middle turbinectomy or lateralization would be performed first, as the children’s nasal cavities are narrower than those of adults. In our series, 10 (52%) patients received a partial middle turbinectomy. In the other 9 patients, middle turbinate lateralization alone was sufficient to expose the sphenoid ostium. Theoretically, lateralization of the middle turbinate could lead to fractures of the basal lamella and ethmoid cells. These potential fractures of the skull base could induce leaks of cerebrospinal fluid, and for this reason, it should be performed only by especially skilled surgeons. However, we did not encounter such adverse events during our follow-up of the patients.
Conclusion
Children who presented with opacified sphenoid sinus identified by radiographs had a variety of pathologies, and the most common lesion was associated with inflammatory disease. The symptoms of pediatric sphenoid sinus disease tend to be variable and nonspecific. Computed tomography remains the standard for evaluating sphenoid sinus disease, and ultra-low-dose paranasal sinus CT imaging is recommended. We further demonstrated that ultra-low-dose CT imaging can provide equal or better image quality compared with standard dose CT. Magnetic resonance imaging is an essential adjunct in the diagnosis and selection of treatment for suspected tumors of the sphenoid sinus. The endoscopic transostial approach is especially suitable for the management of pediatric isolated sphenoid sinus lesions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Paediatric Clinical Technology Innovation Project of the Beijing Municipal Administration of Hospitals (Grant Number XTZD201801) and the Special Paediatric Project of the AY Foundation (Grant Number AYEK201805).