
Abstract
Background
Sphenoid sinus mucocele (SSM) was first reported by John Berg in 1889, accounting for 1% to 3% of all paranasal sinus mucoceles, with frontal sinus (65%), ethmoidal sinus (30%), and maxillary sinus (10%).1,2 SSM is comparatively uncommon among children than adults partly due to its slow growth feature. 3 Headache is considered the most frequent symptom of this disease, whereas some other initial symptoms, including visual disturbances or cranial nerve involvement, are nonspecific. For these reasons mentioned above, misdiagnosis often occurs.4,5 Clinically, patients tend to consult doctors first in the Neurology or Ophthalmology clinics where they might be diagnosed as SSM based on imaging data and then referred to ENT department for further treatment.
Here we presented a 9-year-old girl with sudden blindness in her right eye treated by endoscopic intranasal sphenoidotomy and optic nerve decompression, leading to a good prognosis without any postoperative complications.
Case Presentation
A 9-year-old girl, presented with acute right-sided visual loss because of strong light stimuli, was initially seen in the Ophthalmology clinic. The girl had weakly visible light perception in the temporal visual field at an early stage but quickly progressed to complete blindness after tens of minutes. She was in good general health, without any nasal, ocular, and respiratory associated symptoms, including headache, diplopia, proptosis, and movement disorders in the affected eye.
Upon physical examination, her visual acuity was hand motions at 10 cm in the right eye, whereas the pupil was dilated with 5 mm diameter and didn’t react to light and accommodation, but with positive result of relative afferent pupillary defect. Intraocular pressures were 20 or 15 mmHg in the right and left eye, respectively. Moreover, visual evoked potential examination showed that there’s no significant P2 wave amplitude difference in both eyes, with obvious P2 wave latent period delayed in the right eye as compared to the left eye. Furthermore, an orbital magnetic resonance imaging (MRI) scan revealed that an ovoid, homogenous lesion closely adjacent to the intracranial segment of the optic nerve was observed in the right sphenoid sinus and was suspected of SSM measuring a small size of 0.5 cm*1.1 cm*1.4 cm (Figure 1A1 and A2). The young patient was then transferred to our ENT department for further treatment.
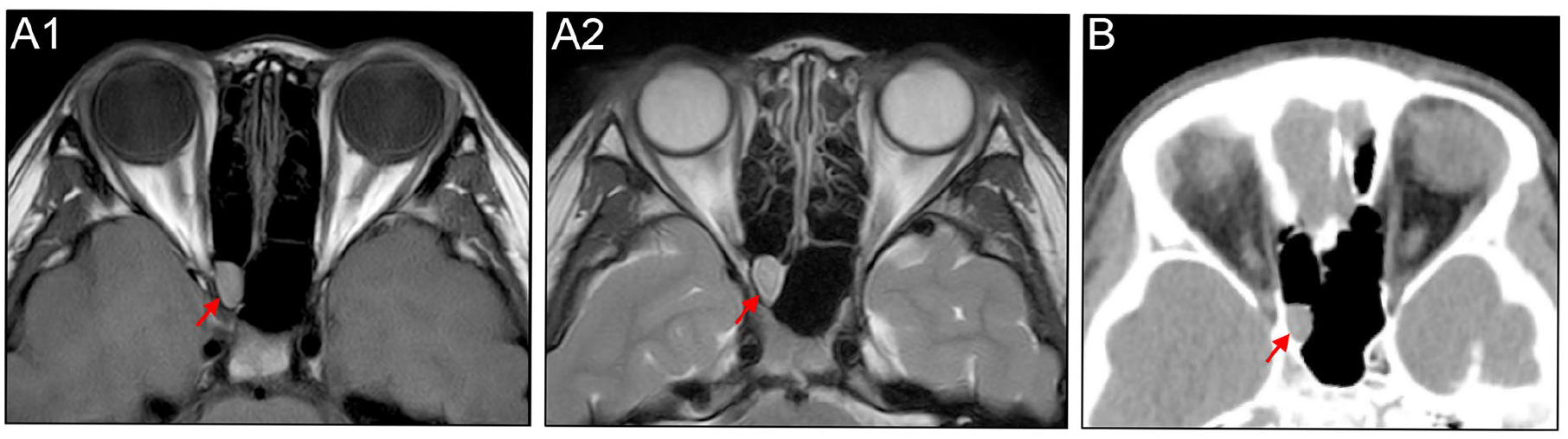
A small mucosa protrusion was found in close proximity to the intracranial segment of optic nerve in the right sphenoid sinus, with different features of hypointense, hyperintense, and homogenous opacification in the T1-weighted orbital MRI (A1), T2-weighted orbital MRI (A2), and sinus CT (B), respectively. MRI, magnetic resonance imaging; CT, computed tomography.
Computed tomography (CT) scan of the nose and paranasal sinuses showed that an isolated, small mucosa growth limited to the right sphenoid sinus in close proximity to the intracranial segment of right optic nerve, but with no evident signs of sinusitis (Figure 1B). Fundoscopy and optical coherence tomography revealed that the thickness of bilateral eye ground and optic disk nerve fiber layer was within normal range, with the right and left central foveal measuring 195 or 217 μm, respectively (Figure 2A and B). Routine blood tests were normal. Meanwhile, other blood samples, including anti-aquaporin 4 antibody, anti-myelin oligodendrocyte glycoprotein antibody, and anti-myelin basic protein antibody detection, found no abnormal results.
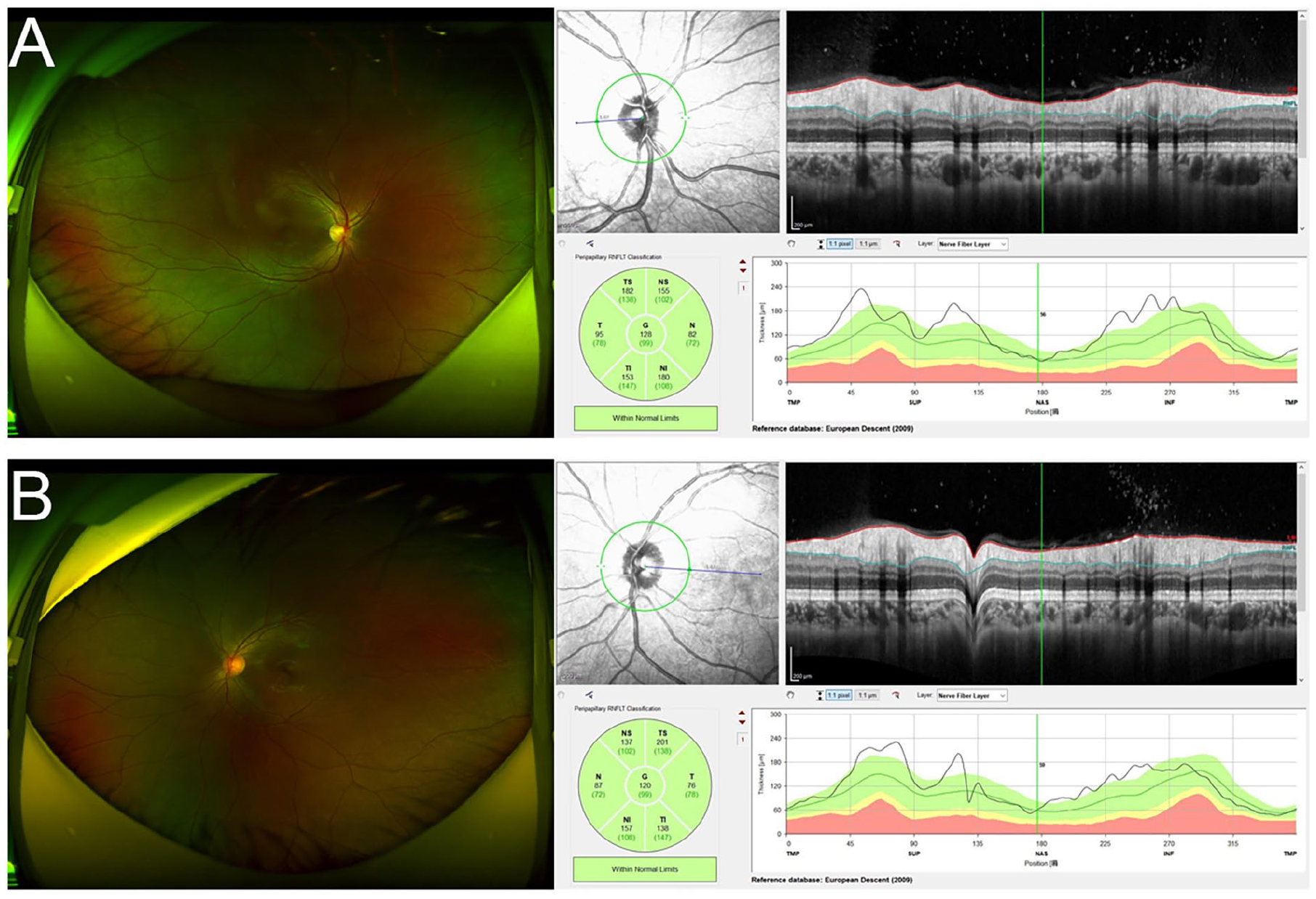
Fundoscopy and optical coherence tomography (A, B) revealed that the thickness of bilateral eye ground and optic disk nerve fiber layer were within normal range, with the right and left central foveal measuring 195 or 217 μm, respectively.
Considering that this girl experienced a 4-day right visual acuity defects after she came to our department, emergency surgery was performed to rescue her vision under general anesthesia and endotracheal intubation. The patient underwent a unilaterally endoscopic intranasal procedure accompanied by resection of the posteroinferior portion of the right middle turbinate as well as sufficient removal of the anterior and inferior walls of the right sphenoid sinus, to facilitate adequate drainage and avoid postoperative recurrences. Intraoperatively, a fibrous membrane encountered with yellow-brown fluid and measured with a total volume of about 2.0 cm*1.5 cm*1.5 cm was completely removed, followed by the right optic nerve full exposure. The clinical diagnosis of SSM was confirmed by pathology (Figure 3A).
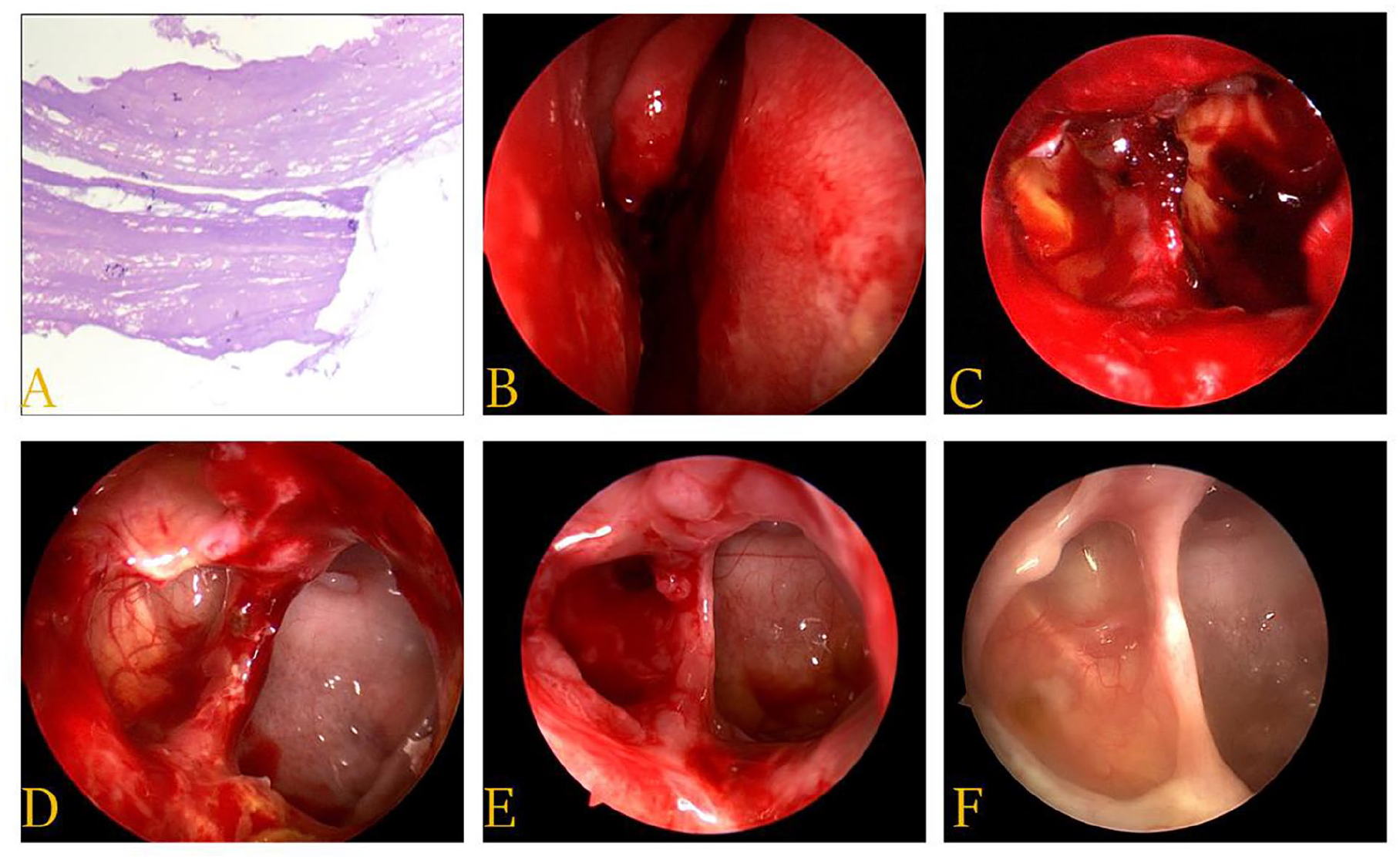
SSM was confirmed pathology (HE staining, A). Part of the right middle turbinate was resected to get a perfect exposure (B). The surgical area was observed and managed regularly postoperatively 1 week (C), 2 weeks (D), 1 month (E), and 4 months (F). HE, hematoxylin-eosin; SSM, sphenoid sinus mucocele.
Medical therapies of antibiotics combined with corticosteroids were initiated postoperatively. Intravenous ceftriaxone 0.75 g was used within 2 days to prevent infection. Methylprednisolone 200 mg was given intravenously on day 1, 2, and 3, with dosage of 100 mg daily over the next 3 days afterward, and then declined to 40 mg for another 3 days. In addition, systemic infusion of ginkgo biloba as well as local injection of Compound anisodine around right superficial temporal artery was maintained for 2 consecutive weeks so as to improve the orbital disturbances. Neither postoperative complications nor obvious bleeding was observed.
The young girl reported slight relief in her right vision immediately after surgery, with the ocular symptoms gradually improving in the next 7 days. On the visual testing, her right pupil was contracted and measured about 3.5 mm in diameter. She visited our clinic regularly at 1-month intervals for 20 months. At her first postoperative visit, the electromyogram evoked potential result showed that bilateral visual evoked potential waves were observed, but with significantly prolonged P100PL and decreased amplitude on the right side, indicating partial dysfunction of the right optic nerve. On the subsequent follow-up records, swollen mucosa tissues in the surgical area were cleared and rinsed with budesonide suspension under nasal endoscopy (Figure 3B-F). As expected, her vision showed remarkable improvement during postoperative 20-month monitor, with no complete recovery of color perception.
This study was approved by the Human Ethics Committee of the Second Hospital affiliated with Shanxi Medical University. Informed consent was obtained from this patient and her parents.
Discussion
SSM is a relatively rare entity with an incidence of 1% to 3% as compared to that commonly occurring subsites in the frontal and ethmoid sinuses. 6 According to literature, a lower incidence among pediatric cases might be assessed as 0.4% in all paranasal sinuses. 3 Since SSM usually grows very slowly, this condition typically presents between the ages of 40 to 60 and doesn’t have any gender predilection. 6 To date, the youngest patient was 8 years old and presented with exophthalmos as reported, 7 this is 1 year younger than the patient in our case.
There are various clinical manifestations including headache, visual disturbances, dizziness, nasal congestion, and facial pain involved in patients with SSM. Usually, deep-seated headache in the supraorbital or retroorbital region is the most dominating symptom, followed by the second-most common symptom of visual impairment. 4 Although SSM is benign in pathology, it may exhibit malignant potential and cause some severe complications due to the expansile opacification in the sphenoid sinus extending into the neighboring structures such as the optic nerve, dura, pituitary gland, cavernous sinus, and internal carotid artery.4,5 Clinically, some patients suffered from visual discomforts due to optic or II, III, IV cranial nerve(s) involvement and firstly consulted doctors in the Ophthalmology or Neurology clinics as such often experienced in our case. 4 Therefore, a better knowledge of SSM by ophthalmologists, neurologists, and otolaryngologists is very important for early diagnosis and proper management.
Some factors as infection, inflammation, and trauma might be attributed to SSM, but the precise mechanism remains unclear.3,8 In most cases, persistent headaches in patients might be induced directly by mechanical pressure of expanded opacification along with bone erosion on the sphenoid sinus or surrounding structures, as well as indirectly through the expression of pro-inflammatory cytokines such as IL-1, IL-6, and PGE2.2,9 Different from these reports, our patient had no headache or nasal discomforts, possibly due to the small size of mucocele without any inflammatory signs in the sphenoid sinus. However, she suffered from sudden right-sided blindness as the initial symptom, this triggered our speculation on the chance that some mechanisms might be involved in (i) congenital hypoplasia of narrow sinus ostium in right sphenoid sinus based on the intra-operative observation; (ii) an isolated, small and fibrous cyst in close proximity to the optic nerve with long-time compression of its intracranial segment based on both preoperative CT and MRI scan; (iii) compensatory function for partial eye-threatening symptoms to make the little child easily ignore unilateral visual failure, according to literature 10 ; (iv) the negative effect of excessive light on the retinal ganglion cell and irreversible damage on one’s vision, as previously described, 11 which could be partly explained by the immediate improvement in her vision after surgery, but without full recovery of color perception till now.
Differential diagnoses should be identified in relation to adolescents with acute or chronic visual impairments.8,9,12 On the basis of our patient’s present history and preoperative examinations, some common inflammatory diseases, including acute sphenoid sinusitis, retrobulbar optic neuritis, and orbit apex syndrome as well as some suspected tumors that occurred in the paranasal sinus or orbital regions could be excluded. Besides, some serum-specific antibodies were detected to rule out the possibility of neuromyelitis optica among pediatrics according to the ophthalmologist’s advice.
Most researchers believed that either CT or MRI was a useful tool to make diagnosis of SSM, whereas others argued that postoperative radiographic imaging was not recommended as a routine procedure.2,3 In our case, both orbital MRI and sinus CT were performed before surgery to determine the extent of SSM and its relationship with surrounding structures. Postoperative MRI or CT was not planned in review of the young age and radiation side-effect. Instead, nasal endoscopic examination was done during the follow-up period.
Once a patient with ocular symptoms is suspected of a diagnosis of SSM, surgical approach should be conducted in emergency. 3 However, controversies arose about the time window of surgical intervention. Studies demonstrated that endoscopic intranasal surgery should be completed within 6 days after the onset of orbital symptoms, whereas others suggested to be done within 24 to 48 hours to reduce the risk of optic atrophy and improve the disease prognosis.5,10 Although endoscopic sphenoidectomy and sinotomy are very easy, effective, and minimally invasive for patients in clinical practice, they seem a little bit difficult in children because of sinus anatomy. 12 Based on these findings, the majority of pediatric sufferers 71% to 100% with SSM-caused visual or neurological impairment tended to remit completely if timely surgical intervention was done,3,9 as was seen here in this case.
Conclusion
To our knowledge, a better understanding of SSM in pediatrics is essential for clinicians, including neurologists, ophthalmologists, and otolaryngologists to make early diagnosis and correct treatment through MRI and CT scans. In addition, prompt surgical intervention of endoscopic transnasal sphenoidectomy followed by optic nerve decompression is a very safe, effective, and minimally invasive method for patients with diagnosis of SSM, so as to guarantee currently good clinical outcomes.
Footnotes
Acknowledgements
None.
Authors Contributions
Original draft preparation and data collection, F.-L.C. and L.H.; writing, editing and literature searching, F.-L.C. and D.-N.X.; medical management of the patient, Y.-F.A., F.-Y.L., T.-T.L. and S.-Y.L.; supervision, Y.-F.A. and C.-Q.Z. The authors read and approved the final manuscript. Y.-F.A. and C.-Q.Z. contributed equally and shared co-corresponding author.
Availability of Data and Materials
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by research grants from National Natural Science Foundation of China (No. 81870707, 82171119, 82171120, 82201263), Youth project of natural science basic research program of Shanxi province (No. 20210302124306), Research Project of health commission of Shanxi province (No. 2021062).
Ethics Approval and Consent to Participate
Consent from the patient was obtained in this article.