
Abstract
Myositis ossificans (MO) is a benign, self-limiting, and nonneoplastic lesion involving the skeletal muscle or soft tissue, rarely occurring in the head and neck. It is relatively rare in clinical practice, and it is difficult to distinguish specific cases from musculoskeletal conditions, which poses unique challenges for clinical diagnosis and treatment. We reported that a 9-year-old boy suffered from local and nontraumatic MO of the trapezius muscle. Given the rarity of this case, the present article detailed the diagnosis and treatment of this rare case and reviewed the relevant literature on MO, focusing on the clinical, pathological, and radiographic characteristics of MO. Notably, these investigations aimed to enhance clinicians’ understanding of the disease and improve diagnostic accuracy.
Introduction
Myositis ossificans (MO) is a benign and nonneoplastic lesion characterized by the proliferation of fibrous tissue with extensive new bone or cartilage formation. 1 Notably, this can occur throughout the body but is more common in the skeletal muscle groups of the extremities (eg, lower extremity quadriceps, medial abdominis, or upper arm muscles) or in the soft tissues surrounding the joints (eg, fibrous tissue, subcutaneous tissue, ligaments, and even blood vessel walls). 2 However, the etiology and pathogenesis of the disease remain unclear. 3,4 Based on the clinical manifestations, MO is divided into MO progressive (MOP), MO circumscripta (MOC), and nontraumatic MO. 5,6 Because the clinical symptoms of MO are mostly atypical and the imaging diagnosis of the lesion in the early stage is limited, this disease is often confused with benign and malignant lesions such as musculoskeletal infections, soft tissue sarcoma, and osteosarcoma, resulting in missed diagnosis and misdiagnosis. 2 Importantly, a pathological biopsy is a gold standard for diagnosing MO. As the lesion matures, computerized tomography (CT) imaging will reveal typical features. 4 Unfortunately, if left untreated, MO will seriously affect the patients’ physical health and increase the economic burden on the family and society. 6 Therefore, clinical awareness and attention to this disease are needed. In this article, we presented the case of a 9-year-old boy with nontraumatic MO of the trapezius muscle and reviewed the relevant literature.
Case Presentation
General Information
A 9-year-old boy was admitted to the Department of Otolaryngology, Head and Neck Surgery at our hospital with intermittent low-grade fever for 1 month and a mass in the left-sided neck for 3 weeks. The patient had no history of head and neck trauma, neuromuscular disease, burns, or other systemic conditions. Physical examination revealed a painful mass on the left-sided neck with an approximate range of 10 cm × 8 cm × 9 cm. In addition, the superficial skin was red, swollen, and ruptured. Furthermore, the local skin temperature was slightly high, the texture was medium, the boundaries were still clear, the pressure pain was positive, and the neck activity was limited.
The laboratory tests showed that the C-reactive protein, white blood cell counts, and erythrocyte sedimentation rate were above normal. Albumin was below normal. T-cell test for tuberculosis infection and lymphocyte culture was negative. Galactomannan and fungal D-glucan tests, anti-streptolysin O and mycoplasma pneumonia antibodies, anti-nuclear antibody and anti-double-stranded DNA titers, carcinoembryonic antigen, alpha-fetoprotein, and neuron-specific enolase were normal.
Imaging Examination
During hospitalization, the patient completed the CT and cervical orthopantomogram. CT showed an inflammatory and occupying lesion involving the soft tissue of the left-sided neck, mainly in the trapezius muscle. The superficial skin was ruptured, and irregular calcification and ossification shadows were observed in the soft tissue. The lesion range was 9.7 cm × 7.8 cm × 8.9 cm, which was closely related to the occipital condyle and the transverse process of the atlas (Figure 1). In addition, the cervical orthopantomogram showed the lesion was located within the soft tissue of the left-sided neck and showed an irregular mass-like dense shadow with multiple calcified and ossified components in the soft tissue and thickening of the surrounding soft tissue (Figure 2).
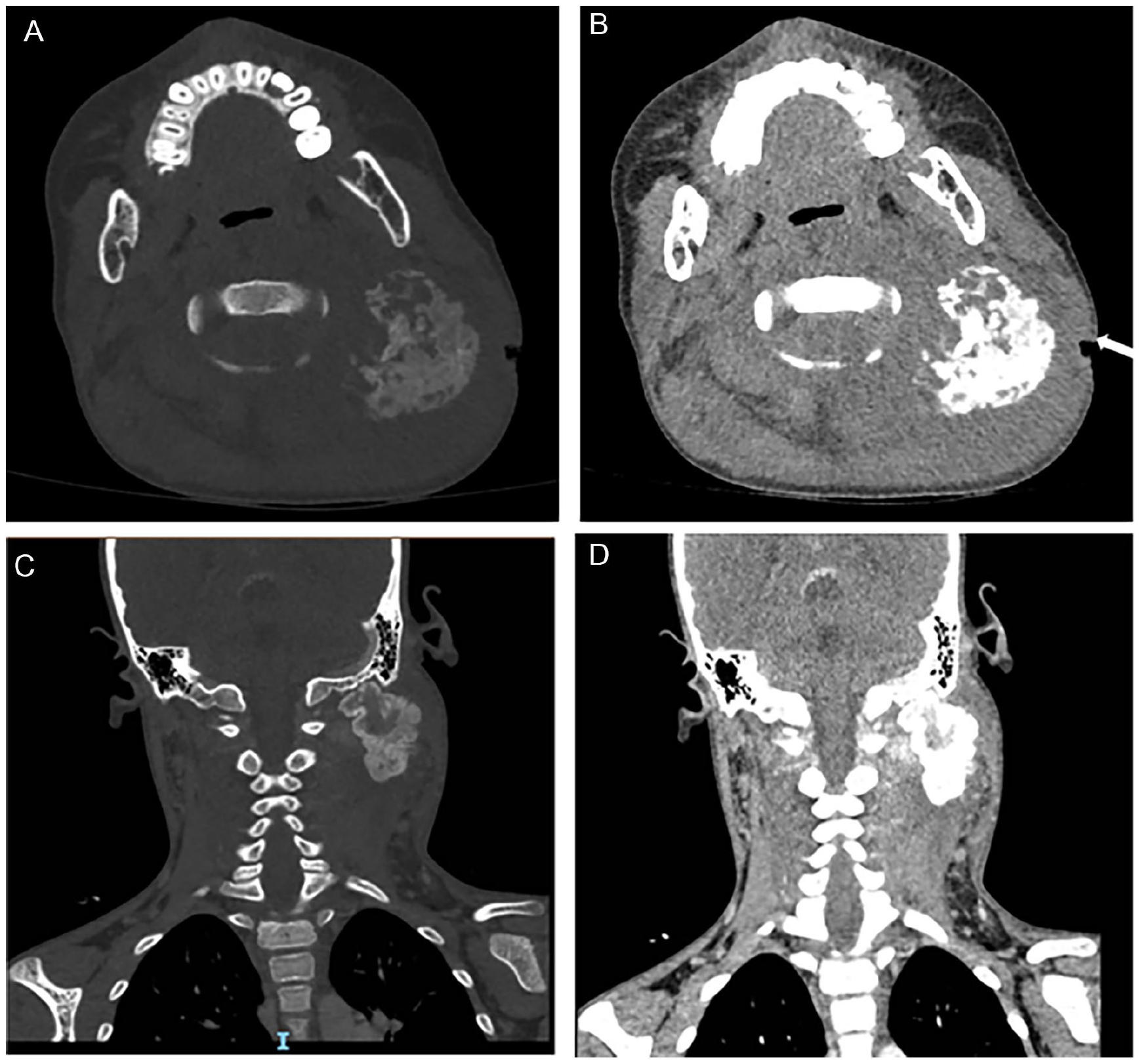
CT images showed the superficial skin was ruptured (indicated by the white arrow). CT, computerized tomography.

The cervical orthopantomogram showed an irregular mass-like dense shadow with multiple calcified and ossified components.
Treatment and Follow-Up
Following admission, the patient was treated with anti-inflammatory therapy. At the same time, a tissue biopsy of the mass in the left-sided neck was performed to clarify the lesion’s nature. Notably, the pathological examination showed MO (Figure 3). After consultation with the immunology department, the child was given oral diclofenac sodium enteric solution (25 mg/dose, bis in die), sulfamethoxazole tablets, and oral detoxification agents (Chinese medicine) for comprehensive treatment. Subsequently, the child’s body temperature gradually returned to normal, and his inflammatory indicators improved significantly. The mass in the left-sided neck was significantly smaller than before, and the superficial skin gradually healed. Subsequently, the child was discharged from the hospital, continued taking oral medication (ie, diclofenac sodium enteric solution, sulfamethoxazole tablets, and oral detoxification agents), and was regularly reviewed at the outpatient clinic. After 5 months of oral medication, the lesion in the left-sided neck was significantly reduced, and the medication was discontinued. Ultrasound of cervical soft tissue was performed 1 month after discontinuation of the drug, showing a well-defined lesion in the left-sided neck with boundaries surrounded by calcified and ossified components resembling “eggshell-like” changes at the edges (Figure 4). Furthermore, magnetic resonance imaging (MRI) showed a significant reduction of the lesion (Figure 5). The outpatient clinic recommended continued follow-up and observation. The child has been off the medication for 13 months, and during this follow-up period, the mass gradually reduced, and no recurrence was detected.
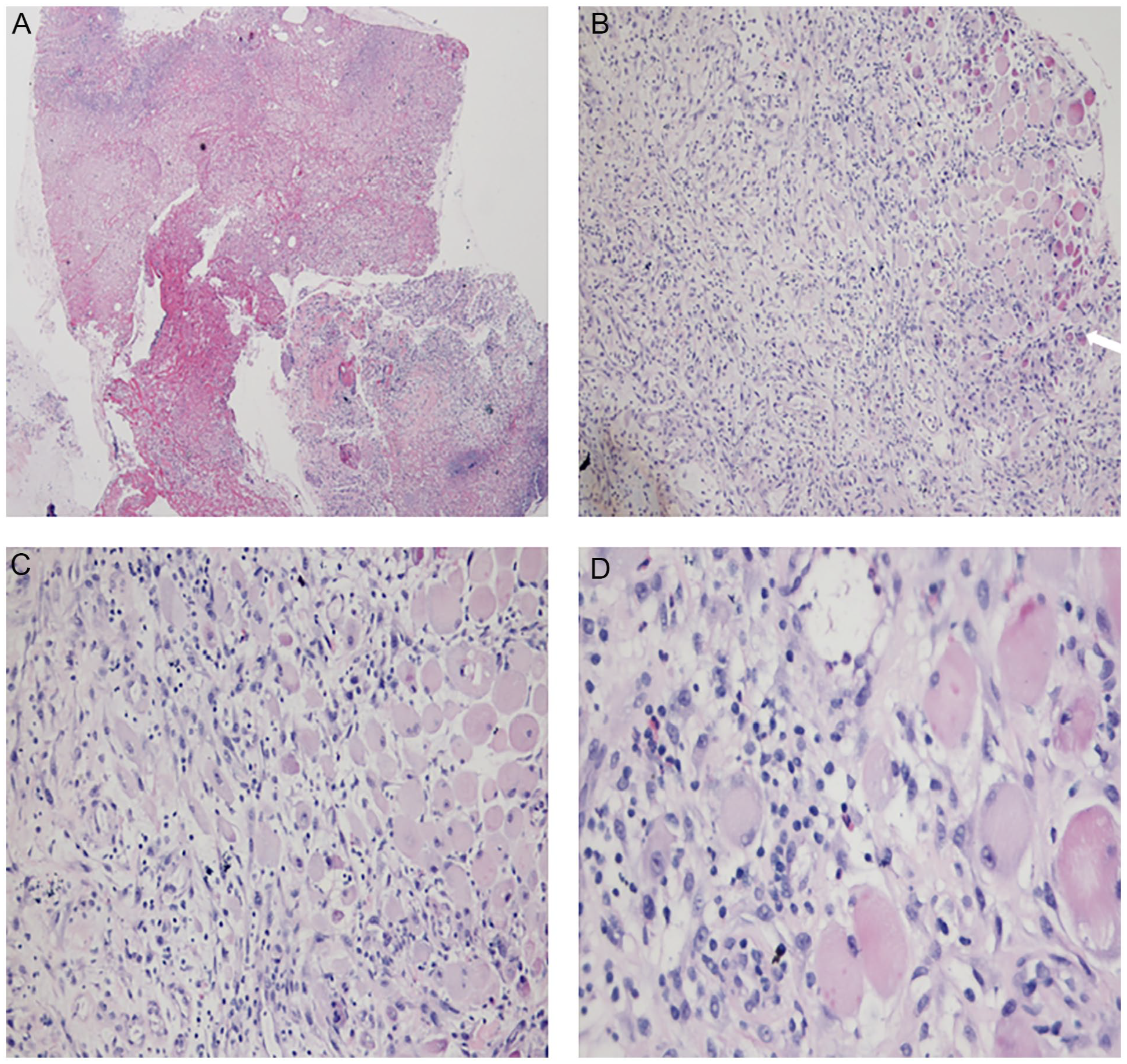
The pathological examination of the mass in the left-sided neck.
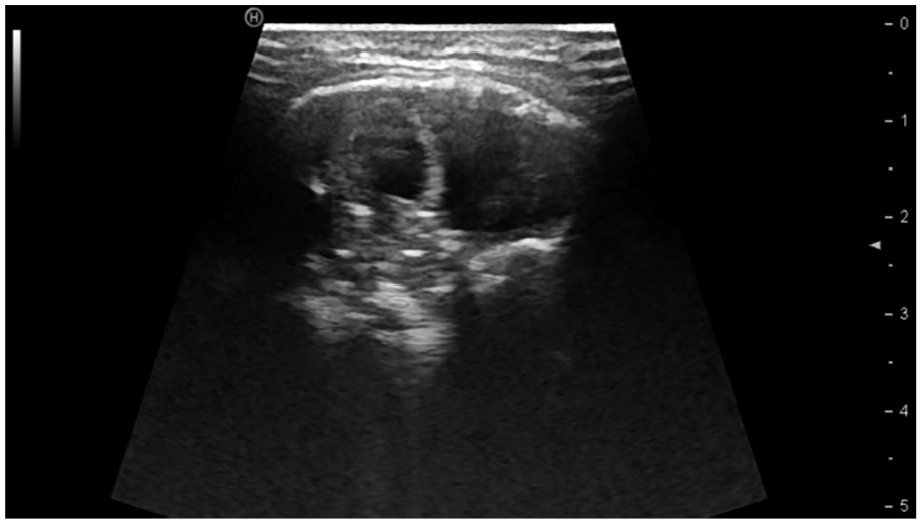
Ultrasound of cervical soft tissue showed “eggshell-like” changes at the edges.
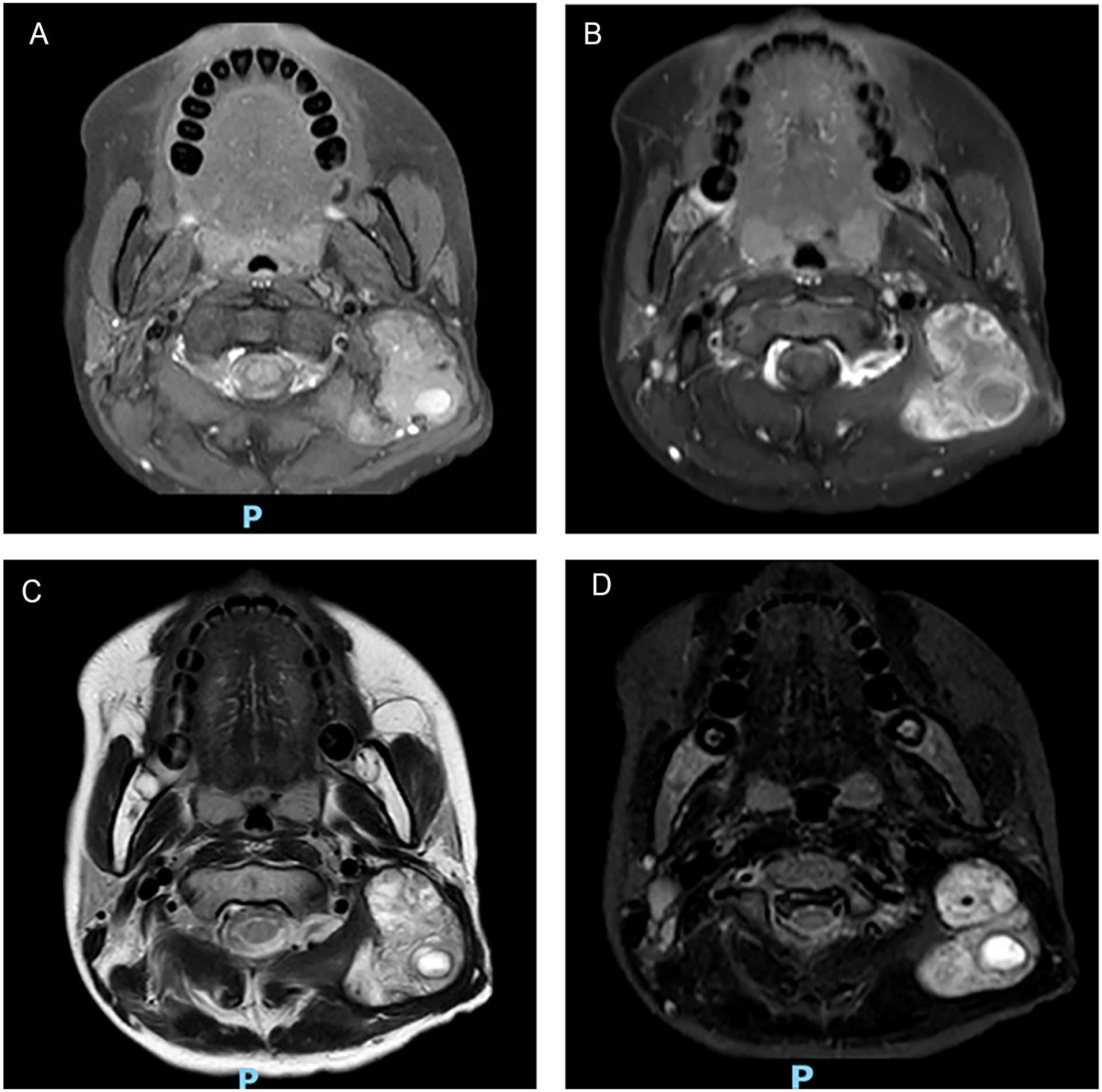
MRI showed a significant reduction of the lesion following discontinuation of the comprehensive drug treatment. MRI, magnetic resonance imaging.
Discussion
MO, known as osteogenic fibrous dysplasia or osteogenic fibrous hyperplasia, is a benign, self-limiting, and nonneoplastic lesion characterized by the proliferation of fibrous tissue with extensive new bone or cartilage formation. 2 The course of MO is as short as a few weeks and as long as several years. 3,4 Generally, according to the clinical manifestations, MO can be classified into three categories: MOP, MOC, and nontraumatic MO. 5,6 MOP is mainly caused by mutations in the gene encoding activin A receptor type I (ACVR1)/activin-like kinase 2 (ALK2) and is an autosomal dominant disorder. 7 The lesions are generalized, diffuse, sometimes familial, and often develop in the first few years of life, with progressive ossification of extraskeletal muscles or connective tissues associated with pain or disability. 8 In addition, both nontraumatic MO and MOC present with local, nonprogressive lesions, 6 which are primarily seen in adolescent or young adult males and involve not only skeletal muscles of the extremities or their surrounding soft tissues 8,9 and involve other parts of the body such as medial pterygoid muscle, 10 temporal muscle, 11 abdominal rectus muscle, 12 paraspinal muscle, 13 and masseter muscle. 14 MOC is associated with localized violence or repeated trauma, with a prevalence of 60% to 75%. 15 In contrast, nontraumatic MO is associated with neuromuscular disease, burns, chronic infections, some systemic diseases, and so on. 3,13 Likewise, some patients with MO may combine with joint fracture or dislocation. 7 The lesion may occur at any age but is rare in children under 10. 9,16 This article reports the case of a 9-year-old boy with nontraumatic MO, mainly involving the trapezius muscle. It is rarely reported at home or abroad. Thus, we focused on this case and reviewed the relevant literature to enhance the understanding of nontraumatic MO and improve the accuracy of clinical diagnosis.
The clinical manifestations of nontraumatic MO are atypical and are divided into three stages based on the progression of the lesion, including early, intermediate, and mature. 2 The early stage occurs in the first 4 weeks after injury and presents as a distinctly swollen, painful, and soft mass characterized by an inflammatory cascade; thus, ossification is usually not evident during this period. 5 After 4 to 8 weeks following the progression to the intermediate stage of the disease, the lesion gradually reduced and hardened, and prominent calcification was observed via imaging. This is followed by the maturation phase, characterized by marked peripheral bone formation. 5 Over the next few months, the lesion becomes self-limiting, eventually consolidating or regressing. However, lesions of nontraumatic MO presented at different times cannot be easily distinguished from benign and malignant conditions such as musculoskeletal infections, soft tissue sarcoma, and osteosarcoma. 17,18 Particularly when a lesion occurs around the joints, it is easily confused with inflammatory arthritis. 6 Diagnosing nontraumatic MO directly based on a simple history and physical examination is challenging in clinical settings. 13 Therefore, multiple imaging means and pathological examinations are needed to clarify the diagnosis and make a differential diagnosis to avoid missed and misdiagnosis.
In addition to clinical manifestations, pathological and radiographic examinations are complementary and have specific characteristics at different stages of the nontraumatic MO. 5,6,19 Specifically, in the early stage, the pathology shows abundant and immature mesenchymal cells and fibroblasts. Due to a lack of calcification and ossification, MRI and ultrasound can assist in assessing early lesions. 5,20 T1-weighted imaging (T1WI) and T2-weighted imaging (T2WI) images may show iso- or high-signal heterogeneous mass with unclear boundaries, and the signal intensity was similar to that of bone tissue. 20 In the intermediate stage, the lesion is gradually calcified and ossified from the periphery to the center. Notably, the pathology shows a progressive distribution, characterized by immature cells enriched in the central zone, immature bone formation in the intermediate zone, and mature lamellar bone in the peripheral zone. 21 This specific distribution has an important reference for the diagnosis of MO. 22 During this period, CT, orthopantomogram, and ultrasound are better than MRI in showing the lesion, which can show high-density shadows with different degrees of circular calcification. The lesion gradually matured and completed ossification when the condition progressed to the mature stage. Furthermore, the pathology shows a lesion surrounded by mature lamellar bone. CT, orthopantomogram, and ultrasound may also show irregular high-density masses. Moreso, MRI shows equal or slightly longer signals on T1WI and T2WI images with clear boundaries. In short, clinical manifestations, pathological examinations, and radiographic examinations have their advantages in showing the characteristics of MO in different stages, and they should be evaluated and applied comprehensively.
The primary treatment for nontraumatic MO is to develop an individualized plan according to the lesion’s size, location, and nature. 5 Due to the self-limiting nature of nontraumatic MO, some patients with small lesions and no functional impairment can be temporarily followed up, and the lesions may mature or even regress during this period. As for those with larger lesions, conservative and surgical treatments can be chosen. Usually, conservative treatment includes general treatment, symptomatic medication, physical therapy, and so on. 23 General treatment (eg, icing and braking) should be applied as early as possible after the onset of nontraumatic MO, and nonsteroidal anti-inflammatory drugs can be used to relieve pain. 24,25 Previous studies have also reported that local low-dose laser irradiation physiotherapy and electrohydraulic shock wave therapy may slow down the progression of this condition. 25 –27 Furthermore, a recent meta-analysis confirmed the efficacy of combining Chinese and Western medicine in treating MO. 28 Thus, clinicians should choose different treatments depending on the patient’s situation. However, conservative treatment is ineffective when severe pain occurs and the joint movement is limited, severely affecting somatic activities. Moreso, the nature of the lesion cannot be clarified, or malignancy is considered. Thus, surgical resection is generally better when surgery is chosen at a mature stage of the lesion to reduce disease recurrence, 19,26 and postoperative attention to pathology and follow-up is still required, with the aid of comprehensive treatment with conservative measures if necessary.
The present article reported a 9-year-old boy who presented first with a low-grade fever and then a left-sided neck mass without a history of neck trauma. A pathological biopsy confirmed a nontraumatic MO and did not exclude infectious factors. CT and cervical orthopantomogram were completed early in the disease, showing an irregular soft tissue mass with multiple calcified and ossified components. After conservative anti-inflammatory treatment and combining Chinese with Western medicine, the lesion gradually reduced and formed “eggshell-like” changes at the edges. At present, the drug has been discontinued for more than 13 months, and the left-sided neck mass has been self-limiting significantly, indicating that the lesion is in the mature stage. However, regular follow-up monitoring is still required.
Conclusion
Nontraumatic MO is usually associated with neuromuscular disease, burns, chronic infections, or other systemic diseases and is relatively rare in children under 10. The article reported a 9-year-old boy with nontraumatic MO, a rare clinical case. CT, orthopantomogram, and ultrasound may be generally used as the first examination of choice in the disease’s different stages and in the lesion’s progression. MRI should be used as adjunctive imaging as calcification may not be well represented on MRI. After diagnosing nontraumatic MO is confirmed by pathological biopsy, conservative treatment can be effective. When the lesion is significantly smaller than before and has reached maturity, regular monitoring is still needed to allow clinicians to choose the right time to intervene.
Footnotes
Acknowledgements
Author Contributions
Prof Xin Ni, Prof Shengcai Wang, and Prof Jie Zhang designed the case study and revised the manuscript; Dr Yanzhen Li, Dr Xuexi Zhang, and Dr Qiaoyin Liu collected the clinical data and completed the follow-up period examinations of this case; Dr Nian Sun, Dr Zhiyong Liu, Dr Xiaodan Li, and Dr Yuwei Liu searched for relevant literatures sources; Mr Ge Zhang and Dr Tingting Ji composed the original manuscript.
Data Availability Statements
The information and images for this article are available online and completely open to the public.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Beijing Science and Technology Commission Capital Clinical Treatment Technology Research and Translation Application Project (Z201100005520077) and the National Natural Science Foundation of China (82271184).
Ethics Statement
This study was approved by the Medical Ethics Committee of Beijing Children’s Hospital. A piece of written informed consent was obtained from the parents of the child for publication of this case report and any accompanying images.