
Abstract
The subtype of eccrine carcinoma known as squamoid eccrine ductal carcinoma (SEDC) is rare; only 38 cases, including only 6 cases in the ear, have been documented in the literature. This may be the first case to focus on the fact that SEDC, located within the dermal and subcutaneous layers, spares the epidermis histopathologically, which can cause clinicians to confuse SEDC with acute perichondritis.
Introduction
Malignant sweat gland tumors are divided into low- and high-grade tumors based on their behaviors. High-grade cancers have substantial metastatic potential and disease-related mortality, whereas low-grade tumors are characterized by a risk of locally destructive progression, local recurrence, and very infrequent distant metastasis. Microcystic adnexal carcinoma and squamoid eccrine ductal carcinoma (SEDC) are low-grade malignant tumors, whereas aggressive digital papillary adenocarcinoma and spiradenocarcinoma are high-grade tumors. 1
SEDC is a rare subtype of eccrine carcinoma; only 38 cases, including only 6 cases in the ear, have been documented in the literature. It may present as ulcerations and papules. Because they originate in the dermis, they commonly penetrate subcutaneous tissues. With multifocal attachment to the epidermis, these tumors frequently exhibit ulceration. 1
However, this may be the first case to focus on the fact that SEDC, located within the dermal and subcutaneous layers, spares the epidermis histopathologically, which can cause clinicians to confuse SEDC with acute perichondritis.
Case Report
We present the case of an 84-year-old male patient with persistent swelling of the ear lobe with an irregular shape and reddish papulae. The lesion first appeared 10 years prior without any physical injury. The size of the lobar papules increased abruptly, with discharge at 3 months. The skin lesion extended from the ear lobe to the antitragus with an eczema-like lesion and no ulceration. He was hospitalized at another clinic for 10 days and was treated with antibiotics for suspected acute perichondritis due to diffuse swelling and auricular erythema. Initially, the symptoms showed improvement for 3 to 4 days, but the symptoms worsened, accompanied by sharp pain. The patient’s previous medical history included diabetes mellitus, hypertension, and myocardial infarction. He was an occupational soldier for several decades. Antibiotics and steroids were initially administered for perichondritis. No improvement was observed even after 10 days of antibiotic use; therefore, a punch biopsy was performed. The biopsy revealed a mixed population of smaller basaloid and larger squamoid cells, occasionally surrounding the ductal lumen. Immunohistochemistry revealed that the tumor cells were CK7 positive and that the specimen was positive for carcinoembryogenic antigen in the ductal structures. These findings are consistent with those of SEDC (Figure 1).
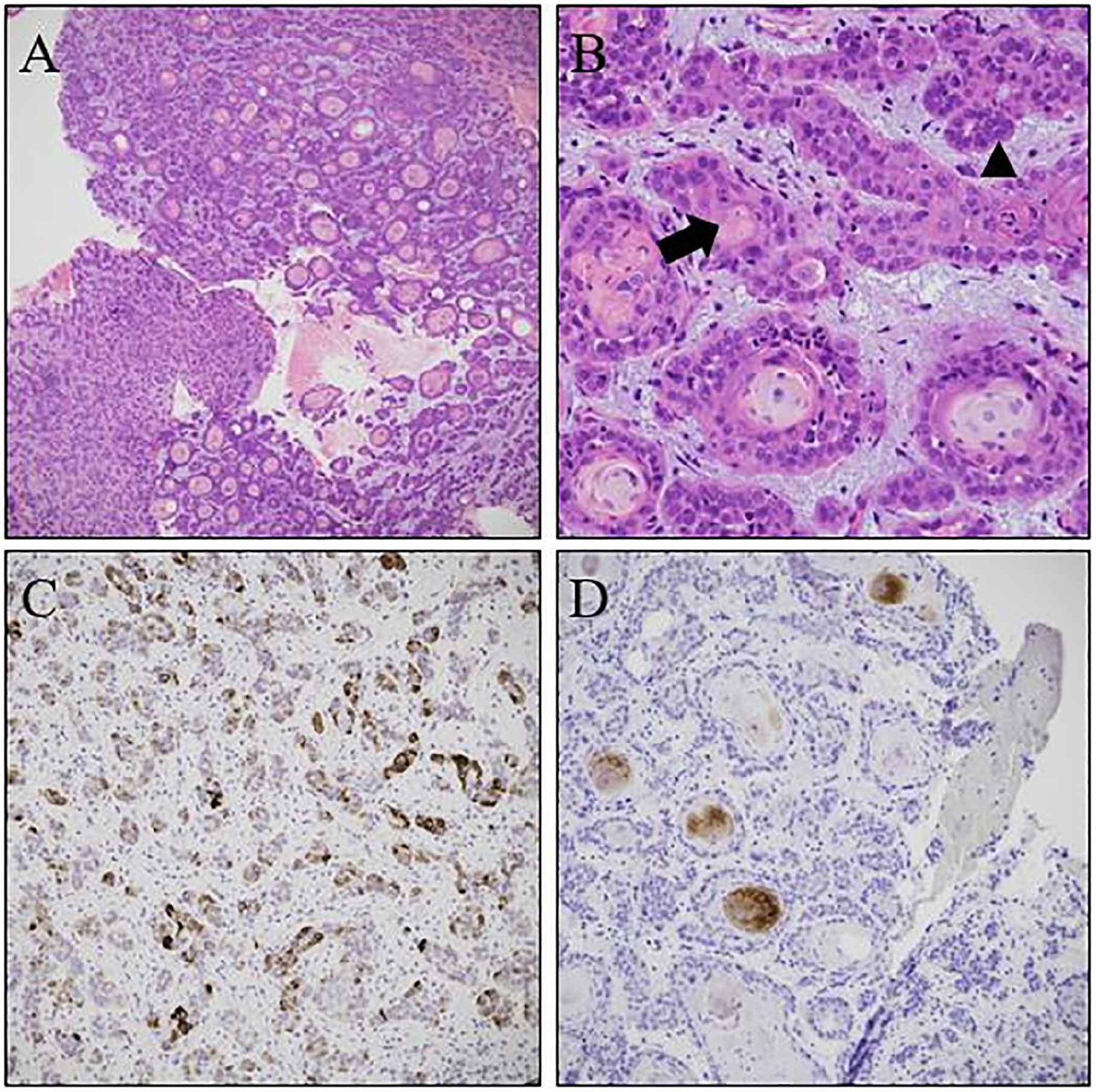
Histopathological tumor features. (A) Low-power field showing a dermal-based invasive tumor composed of cords and nests with lumina (H&E staining, original magnification: ×20). (B) High-power field showing a mixed population of smaller basaloid (arrowhead) and larger squamoid (arrow) cells occasionally surrounding the ductal lumina (H&E stain, original magnification: ×400). (C) Tumor cells positive for CK7 (original magnification: ×200). (D) Immunohistochemistry for carcinoembryogenic antigen showing positivity in the ductal structures (original magnification: ×200). H&E, hematoxylin and eosin.
Preoperative neck computed tomography (CT) scan showed no evidence of metastases or abnormal lymph node enlargements. In addition, on preoperative chest CT scan, a suspected lung cancer mass was found incidentally. Transbronchial lung biopsy was performed twice for histopathological confirmation that there were no distal metastases. The biopsy results indicated a high possibility of adenocarcinoma, but a rebiopsy was recommended. However, the patient refused to undergo a rebiopsy and requested a follow-up chest CT scan. Therefore, based on the diagnosis of SEDC without metastases, extensive tumor resection was planned.
We performed an extensive resection with a margin of 1 cm, and frozen biopsy results showed no cancer cells on the resection margins. The tumor showed squamous and glandular differentiation with increased mitotic activity and cytological atypia. The tumor was located in the dermis and exhibited diffuse infiltrative growth. There was no connection to the overlying epidermis (Figure 2). Therefore, with clinical correlation, there was no epidermal disruption; however, diffuse swelling and erythematous eczema of the auricle were observed. Therefore, the lesion was misdiagnosed as acute perichondritis.
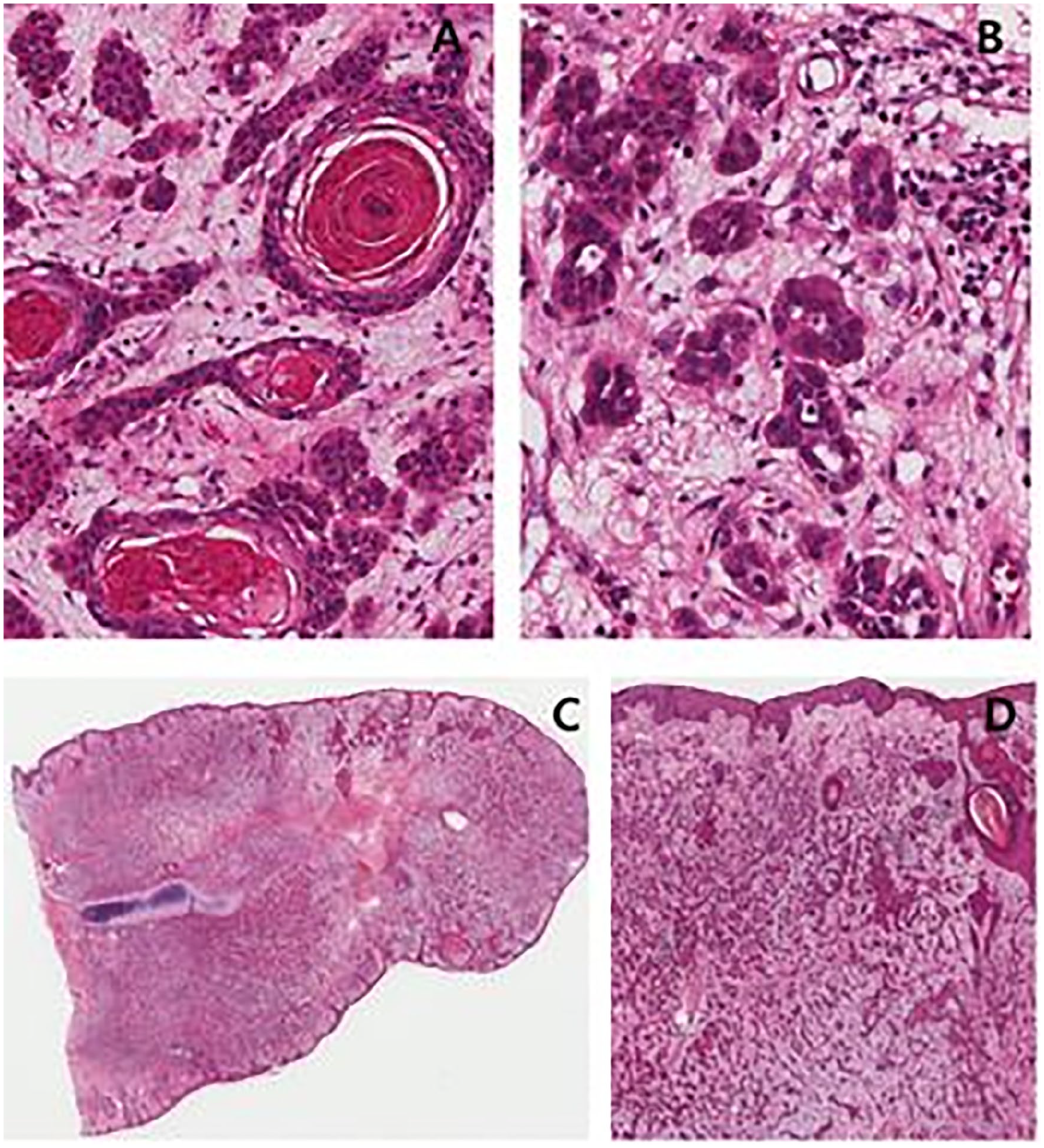
Microscopic tissue image of the left ear mass. (A, B) The tumor showed squamous and glandular differentiation. (C, D) The tumor was located in the dermis and showed diffuse infiltrative growth. There was no connection to the overlying epidermis.
After 1 month of short-term postoperative follow-up, the wound healed well (Figure 3).
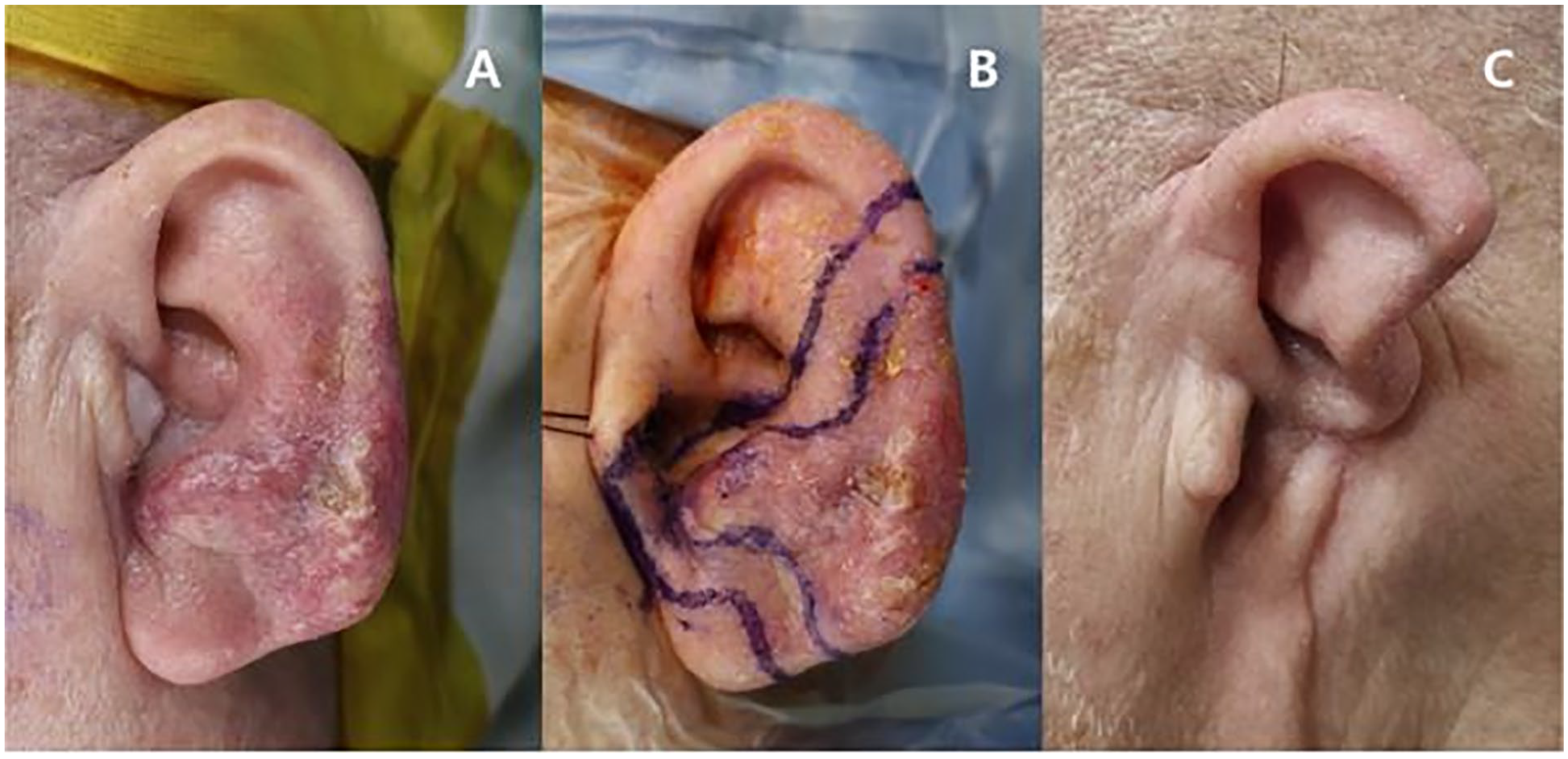
(A) Preoperative. (B) Resection margin. (C) One month postoperatively.
However, the patient had a metastatic lymph node identified in the left parotid gland area on neck CT during follow-up 3 months later. In addition, there was evident fluorodeoxyglucose uptake observed on the positron emission tomography-CT imaging (Figure 4). Consequently, a left parotidectomy and left selective neck dissection were performed. Histopathological examination revealed an SEDC metastasis in the parotid gland, with no evidence of lymph node involvement. The patient continued follow-up visits for 1 month and showed no signs of recurrence.
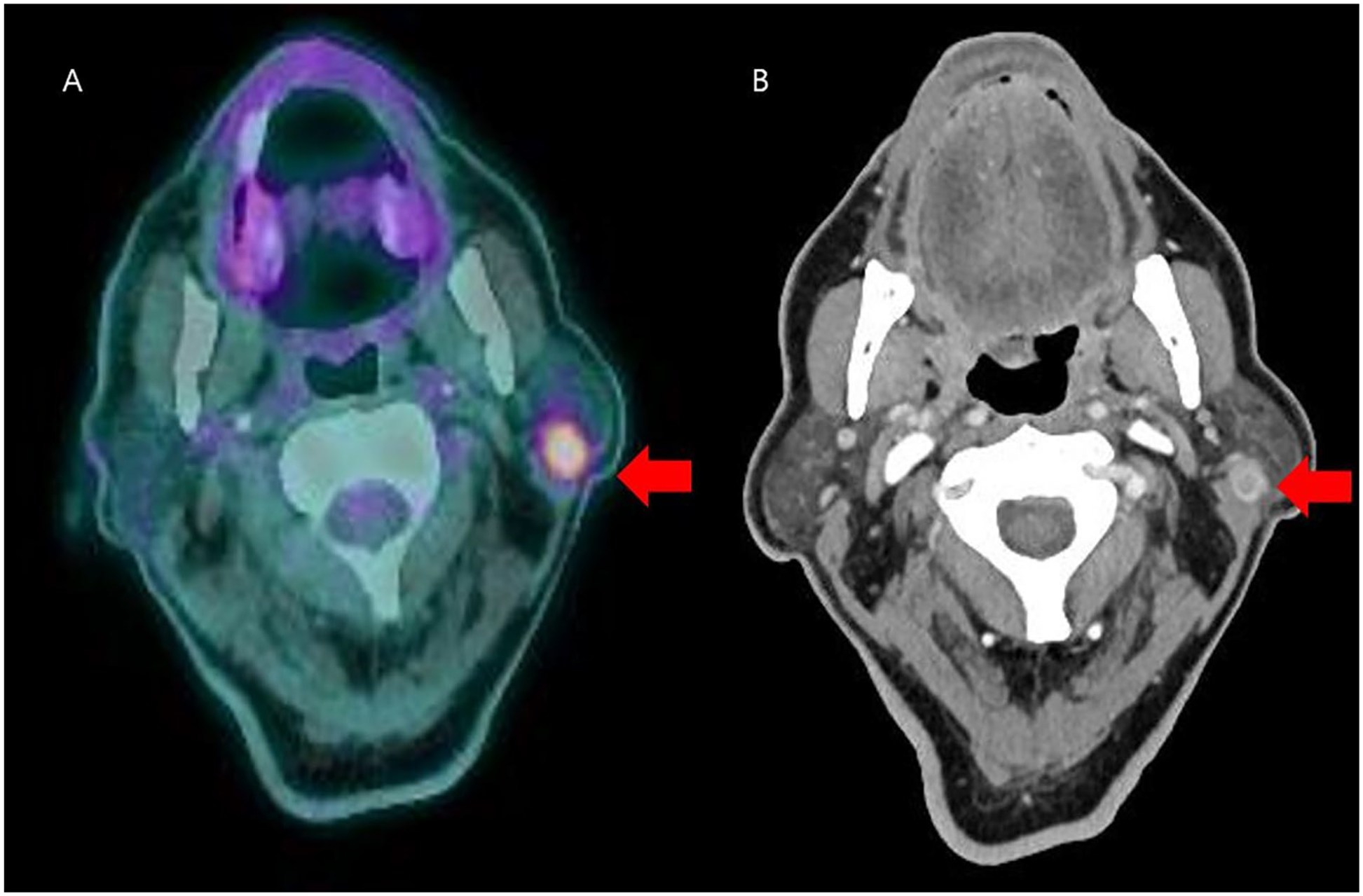
(A) Newly appearing enhancing nodule (arrow) in the left parotid space was identified (B) on a PET-CT scan, and increased FDG uptake is observed in the posterior parotid gland portion. PET-CT, positron emission tomography-computed tomography; FDG, fluorodeoxyglucose.
Discussion
Adnexal carcinoma, also known as SEDC, is rare. Since the 1997 publication of Wong’s initial description of 3 instances of SEDC, 38 cases from 2 original studies have been published. Of all these patients, only 6 were found to have SEDC in the ear 2 (Table 1).
Clinical features and follow-up.
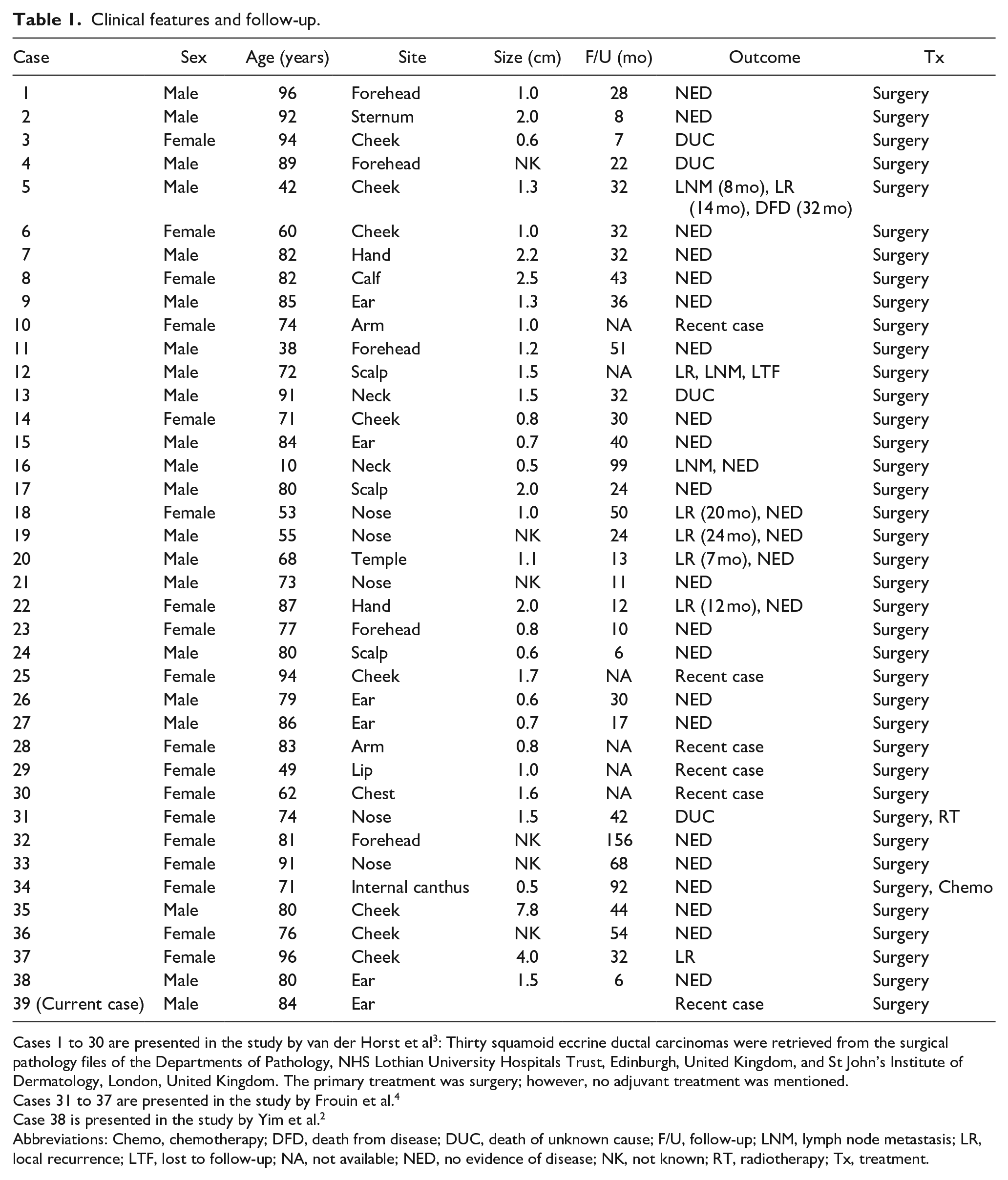
Cases 1 to 30 are presented in the study by van der Horst et al 3 : Thirty squamoid eccrine ductal carcinomas were retrieved from the surgical pathology files of the Departments of Pathology, NHS Lothian University Hospitals Trust, Edinburgh, United Kingdom, and St John’s Institute of Dermatology, London, United Kingdom. The primary treatment was surgery; however, no adjuvant treatment was mentioned.
Cases 31 to 37 are presented in the study by Frouin et al. 4
Case 38 is presented in the study by Yim et al. 2
Abbreviations: Chemo, chemotherapy; DFD, death from disease; DUC, death of unknown cause; F/U, follow-up; LNM, lymph node metastasis; LR, local recurrence; LTF, lost to follow-up; NA, not available; NED, no evidence of disease; NK, not known; RT, radiotherapy; Tx, treatment.
SEDC frequently affects older adults. According to van der Horst et al, 3 lesions developed in sun-exposed regions above the neck in 23 of 30 patients. In our case, the patient was an occupational soldier. Therefore, it can be inferred that there was considerable exposure to sunlight due to many external activities.
Clinically, SEDCs predominantly appear in the head and neck area as nodular or ulcerative skin lesions. SEDCs are asymmetrical tumors with diffuse infiltrative growth patterns and poor margins. Because they originate in the dermis, they commonly penetrate subcutaneous tissues. With multifocal attachment to the epidermis, tumors frequently exhibit ulceration. They can be confused with well-differentiated squamous cell carcinomas (SCCs) because of their superficial characteristics, where there is overt squamous differentiation. Ductal differentiation varies in deeper regions. For differential diagnosis of SCC, it is necessary to identify additional ductal differentiation in the deeper reaches of the tumor. 1
In our case, the patient presented with diffuse swelling of the ear and eczema-like dermatitis without ulceration. This has led to the misdiagnosis of perichondritis. This article introduces a case in which SEDC mimicked perichondritis because SEDC involves the dermis and frequently invades the subcutaneous tissues. We recommend that physicians consider cancerous conditions, such as sweat gland cancers, which involve the dermis and invade the subcutaneous tissues, resulting in a diffusely swollen auricle when suspecting acute perichondritis. If the lesion does not improve despite antibiotics, a deep punch biopsy is required.
SCC is frequently misdiagnosed as SEDC. Atypical squamous proliferation and duct proliferation cannot be seen simultaneously in shallow shave or punch biopsy specimens because the majority of duct-like structures in SEDC are found in the deep dermis. To distinguish SEDC from SCC, it may be necessary to recognize deep infiltrating lumina. 2
Wide tumor excision is the treatment of choice for patients with SEDC. However, owing to its rarity, the long-term effects of SEDC treatment remain unclear. 2
Independent of the excision extent, SEDCs have a high local recurrence rate. This is probably because the tumor has a deep and diffuse infiltrative growth pattern, and perineural infiltration is frequently present. In addition, the disease showed metastasis (up to 13%). Metastases are mainly to lymph nodes; however, distant metastases may also be observed. 1
In this case, metastasis to the parotid gland occurred within 3 months, and it appears that additional consideration is necessary to manage these local recurrences.
Footnotes
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the Biomedical Research Institute at Jeonbuk National University Hospital.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee.