
Abstract
Introduction:
The main aim of this article is to discuss and summarize the research advancements and the treatment methods for sweat gland carcinoma (SGC) based on 2 cases of SGC in our hospital and the related literature.
Case Report:
This article presents 2 patients with SGC who were treated in the China Medical University, Liaoning Provincial Key Laboratory of Oral Diseases from 2007 to 2019. We analyzed the clinical features, therapies, and prognosis of the patients and searched for related literatures.
Discussion:
Two patients underwent extended resection for local lesions with no adjuvant radiotherapy. Neither local recurrence nor distant metastasis was detected during follow-up. Reviewing previous literature, the treatment of SGC includes surgical resection, radiotherapy, and chemotherapy. We have not found an effective treatment. The prognosis of SGC occurred in head and neck is relatively good compared with another primary-site location, primary surgical excision with safe resection margins and neck dissection is recommended.
Introduction
Sweat gland carcinoma (SGC) is a rare type of malignant tumor that occurs in subcutaneous tissue, account for 6% of sweat gland tumors and less than 0.001% of all tumors. 1 Sweat gland carcinoma is more likely in to occur in patients between 50 and 70 years of age, with no race or gender preference. 2 The clinical manifestations are indistinguishable from those of many benign and malignant tumors, such tumors typically occur as solitary intradermal nodules that measure 1 to 5 cm without significant asymptomatic. It has an aggressive clinical course with a high tendency for both local lymph nodes invasions and distant metastasis. 3,4 Here, we report 2 cases of SGC that presented in our hospital with in the last 10 years based on a review of relevant literatures.
Case Report
Case 1
A 65-year-old male patient had experienced significant pain for 6 months on the right side of face due to a recurrent tumor. The surgery was performed at another hospital to remove the tumor; however, detailed information regarding the pathologic diagnosis and the type of surgery was unavailable. The patient has had psoriasis on the right side of face, which was treated with ointment for over 6 years. According to the patient’s family medical history, no one else has been diagnosed with SGC or psoriasis. An extraoral examination revealed a nodule of approximately 2 × 2 × 1 cm. The texture of the nodule was hard, and the color of the epidermis was normal. The lesion had already invaded the facial nerve and induced apparent symptoms of facial paralysis.
The local drainage lymph nodes were not significantly enlarged. Surgery was performed to remove the lesion, which included the skin on the surface of the lesion, and majority of the parotid gland, which guaranteed a surgical margin of more than 2 centimeter. Postoperative pathology observed that atrophic acinar cells in the lobules, fibrous tissue hyperplasia, and duct differentiation. Tiny cancerous tubercles were observed with enlarged nucleoli (Figure 1A-B). Immunohistochemistry results indicated: CK (+), CK7 (+), ki67 (+) 25%, GCDFP-15 (+), P63 (+), CEA (+). No recurrence or distant metastasis was observed during the follow-up of 45 months.
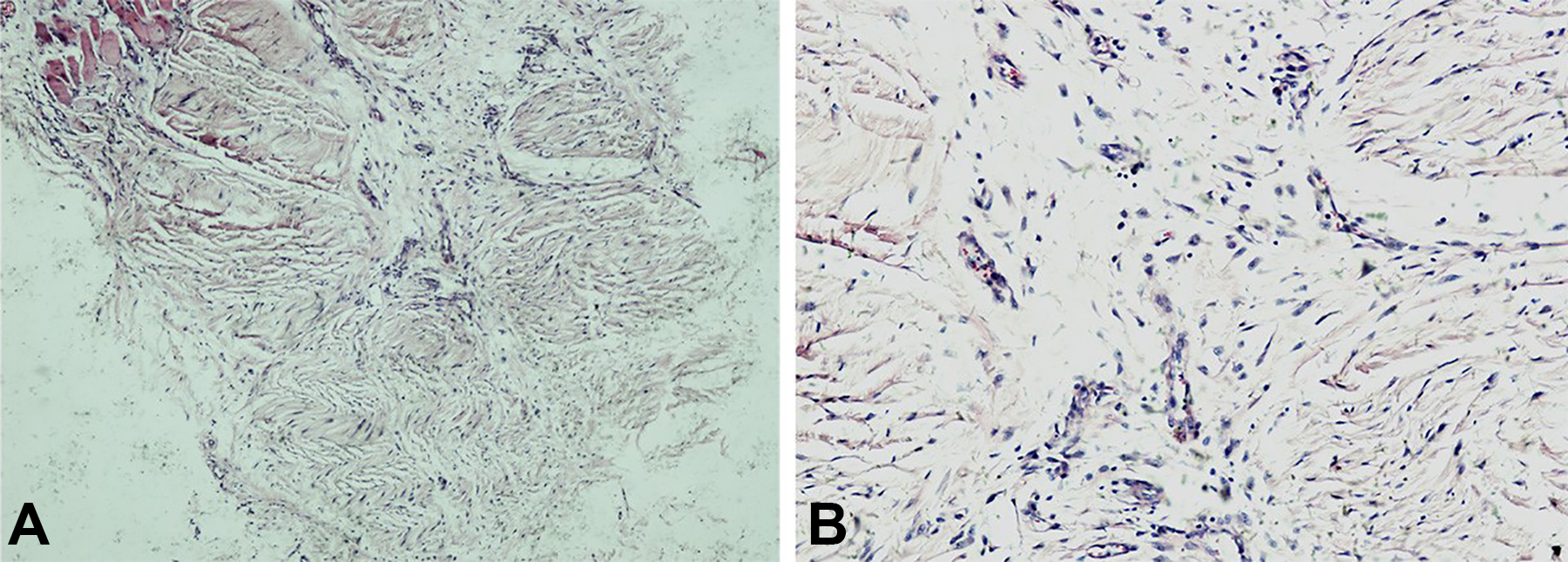
Atrophic acinar cells in lobules with, fibrous tissue hyperplasia and ductal differentiation. A tiny cancerous tubercle was observed; the tumor cell had a clear to lightly acidophilic cytoplasm and round or enlarged nuclei with distinct nucleoli (A: HE ; B: HE ). HE indicates hematoxylin and eosin stain.
Case 2
A 52-year-old male patient was admitted to our hospital because the worried about a painless, recurrent nodule on the left side of face. Recurrence occurred 6 months before admission, when the patient occasionally observed a nodule on the left side of face. An extraoral examination revealed a cutaneous lesion of approximately 2 × 1 cm in the left parotid region. The texture of the lesion was hard with an indistinct boundary, and the coloration of the surface was altered. An auxiliary examination by chest radiography and Doppler ultrasound did not indicate significant distant metastasis. Magnetic resonance imaging showed that the lesion, which had a clear boundary, was located on the outside of the left parotid gland (Figure 2).

The lesion located on the left side of the outside of the left parotid gland had a clear boundary.
During the surgery, we found that the lesion was predominantly located in subcutaneous tissue and that the boundary was indistinct. Further dissection revealed that the parotid gland capsules had been invaded by the tumor. The superficial lobe of the parotid glands and the skin on the surface were removed, and a tumor-free surgical margin was guaranteed (Figure 3). The excised specimen presented had an irregular appearance. The cross-section exhibited had fish-meat-like changes (Figure 4A-B). The patient’s pathological section exhibited epithelioid cells in nest distributed among squamous cells with acidophilic cytoplasm and nuclear fission containing small glandular configurations within (Figure 5A-B). Immunohistochemistry results indicated: CK (+), P63 (−), P40 (−), ki67(+)5%, GCDFP-15(+), CK7(+). In the 7 months after the second surgery, the patient presented lumps with painless on his left side of neck. The cervical lymph node dissection was performed and postoperative pathology was confirmed a diagnosis of recurrent SGC. No recurrence or distant metastasis was observed during the follow-up of 17months.

The incision strategy. The arrows indicate the position of the mass.
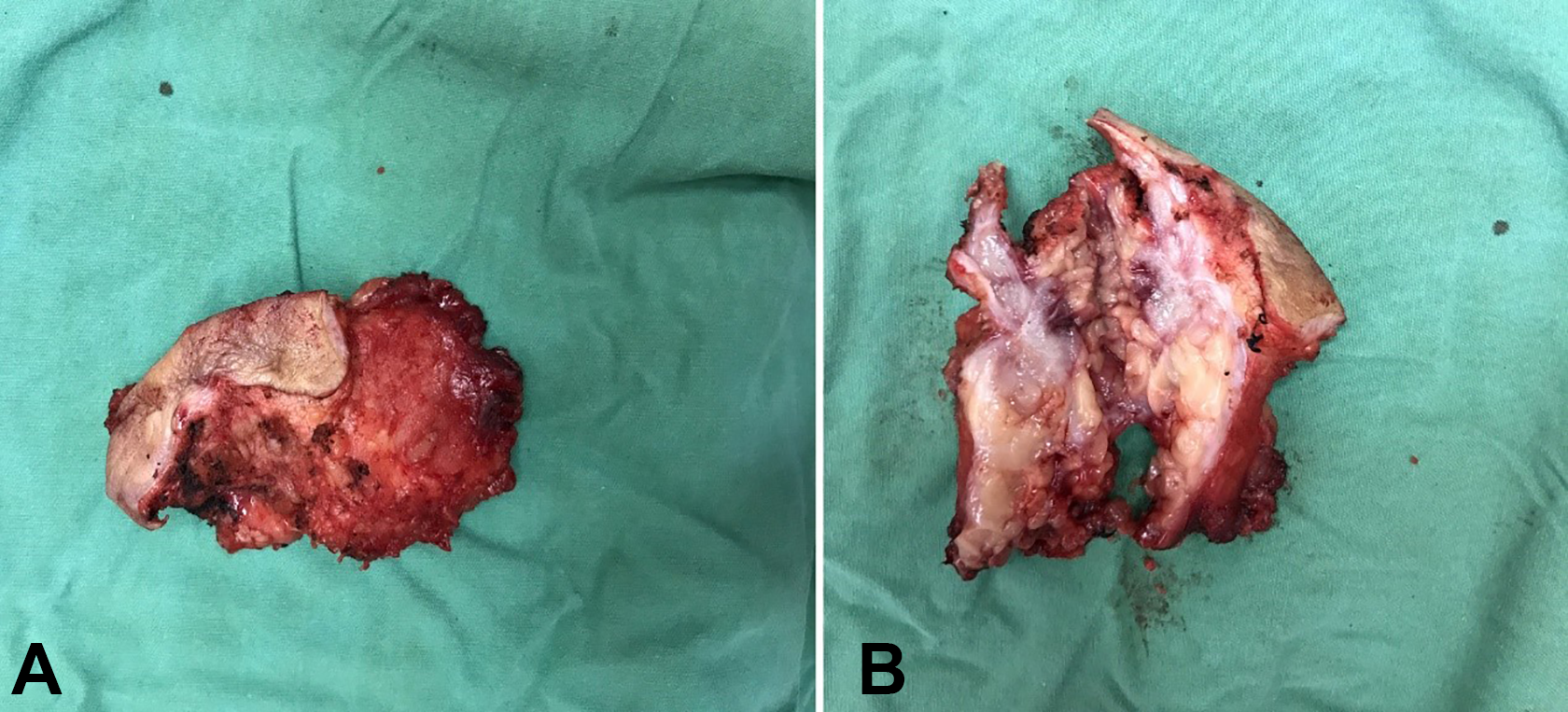
(A) Show the mass, while (B) show the cross-section, with fish-meat-like changes.
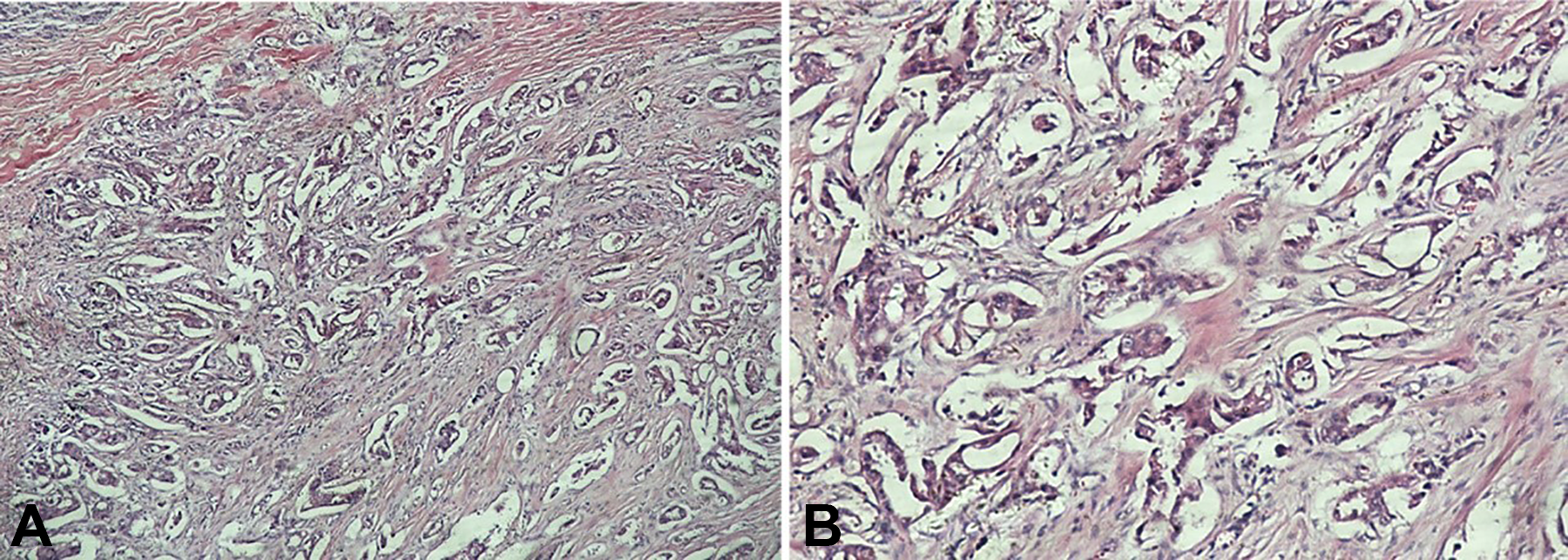
Epithelioid cells with a nest-like distribution among squamous cells, a mildly acidophilic cytoplasm, and visible nuclear fission; nests of different size, and rare, small glandular configurations were found (A, HE ×400; B, HE ×1000). HE indicates Hematoxylin and eosin stain.
Based on the standard of American Joint Committee on Cancer and tumor-node-metastasis staging, the 2 cases belong to histological grade II. Two patients underwent extended resection for local lesions with no adjuvant radiotherapy. Neither local recurrence nor distant metastasis was detected during follow-up.
Discussion
Due to the limited data available in the literature as well as the challenge in classifying this heterogeneous group of tumors, SGC’s historically have been difficult to study. There is no consensus has been established for the diagnosis histopathological features and treatment management for SGC. At the time of literature review, tissue biopsy combined with immunohistochemistry may be required for definitive diagnosis. However, in the absence of obvious histopathological features, the tumors are difficult to distinguish from their benign counterparts or other analogous malignant tumors. 5,6 Throughout the literature, the presence of multiple nomenclatures for similarly described lesions further perpetuating the lack of consensus for standardized taxonomic. Meanwhile, complex classification does not provide much assistance for clinical treatment. 7
In traditional views, sweat gland tumors were divided into eccrine and apocrine, more recent studies have shown that many of these tumors may display properties both eccrine and apocrine variant. Whereas others demonstrate more differentiated subtypes, including malignancies of sebaceous or ceruminous. Moreover, there is insufficient evidence to suggest any clinical importance for separating SGC by their eccrine or apocrine origins. 8,9
In a recent report, Cardoso’s study provides an updated review on malignant sweat gland tumors, emphasizing recently described findings with a potential impact upon the diagnosis and management of these patients. Among the entities of malignant sweat gland tumor, one type is called squamoid eccrine ductal carcinoma, which is associated with high local recurrence and deep, and diffusely infiltrative growth. Microscopic features include overt squamous differentiation in the superficial layer. In the deeper layers, the tumors cells are arranged in smaller nests, cords, and strands in a desmoplastic stroma. 1,6,10 In our report, the tumor diagnosed in the second case is most like squamoid eccrine ductal carcinoma. Squamoid eccrine ductal carcinoma has a low local recurrence (approximately 11%) and regional lymph node metastasis in fewer than 10% in Cardoso’s study. According to the histological images, the tumor diagnosed in the first case in this article is similar to spiradenocarcinoma and cylindrocarcinoma. Spiradenocarcinoma and Cylindrocarcinoma are regarded as a tumor with aggressive behavior, local recurrence and metastasis are higher than squamoid eccrine ductal carcinoma. Expression of P53, P63, and CK7 has been reported as important role of diagnosis. 4 Extended resection with a surgical margin of at least 1 to 2 centimeters is still the major treatment method for SGC. 11 Magnetic resonance imaging is necessary to confirm the tumor limits, and lymph nodes and full surgical excision with free margins, which are all critical to success. 10
In Thomas’ study, a database of more than 2600 cases of Mohs Micrographic Surgery (MMS) demonstrated that MMS is an effective approach for the management of rare cutaneous malignant tumors with cutaneous malignancies were reviewed and analyzed, which can maximally conserve tissue and significantly reduce the recurrence rate. 12,13 Study by Tolkachjov et al also demonstrate efficacy in tumor clearance, and in light of tissue preservation permitted by MMS. Through a reviewing articles published in the last 20 years on SGC treated with MMS, they found that 10 SGC patients, who underwent resection by MMS, without experience recurrence, metastasis or death, during an average postoperative follow-up of 86 months. 14 These malignancy is aggressive and usually drains to the cervical lymph node, but selective neck dissection for SGC patients without a positive lymph node is controversial. 2 Some support lymph node dissection as a first-line therapy, regardless of the high rate of recurrence and distant metastasis in this malignance. Some of the patients who underwent radical neck dissection still had a poor prognosis. A small series reported by Delgado et al demonstrated a high frequency of positive sentinel lymph nodes, which suggests that sentinel lymph node mapping and biopsy are effective tools for SGC patients. 15,16 Fortunately, immunohistochemical stains facilitate the recognition of small microscopic metastases and improve the accuracy of the pathological diagnosis. The current studies cannot answer the question of whether selective neck dissection should be performed in patients who lack obvious lymph node metastasis, and therefore requires further research. Radiotherapy is commonly used in postoperative adjuvant therapy and in the treatment of distant metastases at a dose of 50 Gy ∼ 70 Gy. 17 The therapeutic effect of chemotherapy on SGC has not been confirmed, only a few successful have been reported in single case reports. 18
According to previous literatures, the 5-year survival rate for SGC is less than 30%; the local recurrence rate is as high as 50%; and 60% of the patient exhibit metastasis within 2 years after surgery. 19,20 In the study of head and neck sweat gland adenocarcinoma (SGA), Unsal et al reported that the overall prognosis is relatively good: 5-, 10-, and 20-year disease-specific survival at 94.6%, 89.6%, and 79.8%, respectively. Primary-site location within the head and neck is a significant affecting factor. During course of 20 years, all patients possessing survival data demonstrated 100% survival in SGA of the eyelids and external ear. Sweat gland adenocarcinoma of the scalp and neck demonstrated a significantly worse prognosis in comparison, dropping to 54.3% by 20 years. Sweat gland adenocarcinoma of facial and lip primary sites, which displayed 20-year disease-specific survival of 86.2% and 80%, respectively. 7
The prognosis of SGC occurred in head and neck is relatively good than another primary-site location. Based on the articles reviewed, we suggest that effective treatment management should rely on preoperative biopsy and immunohistochemical examination to confirm the diagnosis and remove lesions by MMS. In the absence of clinical involvement of lymph nodes, a sentinel lymph node biopsy determines whether the cervical lymph nodes should be dissected at the corresponding period. Additionally, postoperative adjuvant radiation therapy is necessary, and long-term follow-up are also needed.
Footnotes
Authors’ Note
Written informed consent was obtained from all patients before the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Certificate NO: School of Stomatology, China Medical University (2017) scientific ethics review (3).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.