
Abstract
Vascular leiomyoma (VL; angioleiomyoma) is an uncommon benign tumor arising from smooth muscle cells within the tunica media of blood vessels, typically presenting as solitary, firm nodules. It predominantly occurs in the lower extremities but rarely involves the head and neck region, particularly the auricle. Auricular VLs commonly appear as small, sharply-demarcated nodules that are generally asymptomatic. Nonetheless, a subset of patients may experience episodic pain, which can be elicited or intensified by environmental or mechanical factors including pressure and cold exposure, complicating clinical diagnosis. Due to the nonspecific presentation, auricular lesions are frequently misdiagnosed preoperatively. Definitive diagnosis relies on histological examination. Herein, we present a rare case involving the right auricle, accompanied by a concise review of the relevant literature to enhance clinical awareness, support early diagnosis, and guide appropriate surgical management of this rare entity.
Introduction
Vascular leiomyoma (VL), also known as angioleiomyoma, is an uncommon benign tumor derived from smooth muscle cells within the vascular walls.1,2 A comprehensive clinicopathological study by Hachisuga et al reviewing 562 cases found that VL predominantly occurs in the lower extremities (~67%), with less frequent involvement of the upper extremities (22%), head and neck region (8.5%), and trunk (2.5%). 1 Auricular VL represents an especially uncommon site, accounting for only about 2.5% of total VL cases. 1 Due to its rarity and nonspecific clinical features, auricular VL poses significant diagnostic challenges, frequently leading to misdiagnosis.2,3 The purpose of this article was to review the existing literature on auricular VL, discuss its clinical presentation, histopathological features, differential diagnosis, and optimal management strategies.
Case Presentation
A 23 year-old male presented with a 2 week history of a painless nodule over his right ear. He reported no history of trauma, ulceration, or infection recently. Physical examination revealed a soft, dome-shaped, non-tender, purple-colored mass ~1 cm in diameter, located on the crura antihelix of the right auricle (Figure 1A). The patient subsequently underwent a skin-sparing surgical excision. A well-encapsulated mass was identified within the subcutaneous tissue (Figure 1B). The excised specimen measured 0.7 × 0.5 × 0.5 cm (Figure 1C). Microscopically, the tumor consisted of encapsulated proliferations of eosinophilic smooth muscle bundles surrounding numerous small slit-like, thin-walled vascular channels, consistent with a solid-type angioleiomyoma (Figure 2A and B). Immunohistochemically, tumor cells exhibited diffuse positivity for smooth muscle actin (SMA; Figure 2C) and negative staining for S-100 protein. No recurrence or auricular deformity was observed during 1 year of follow-up.
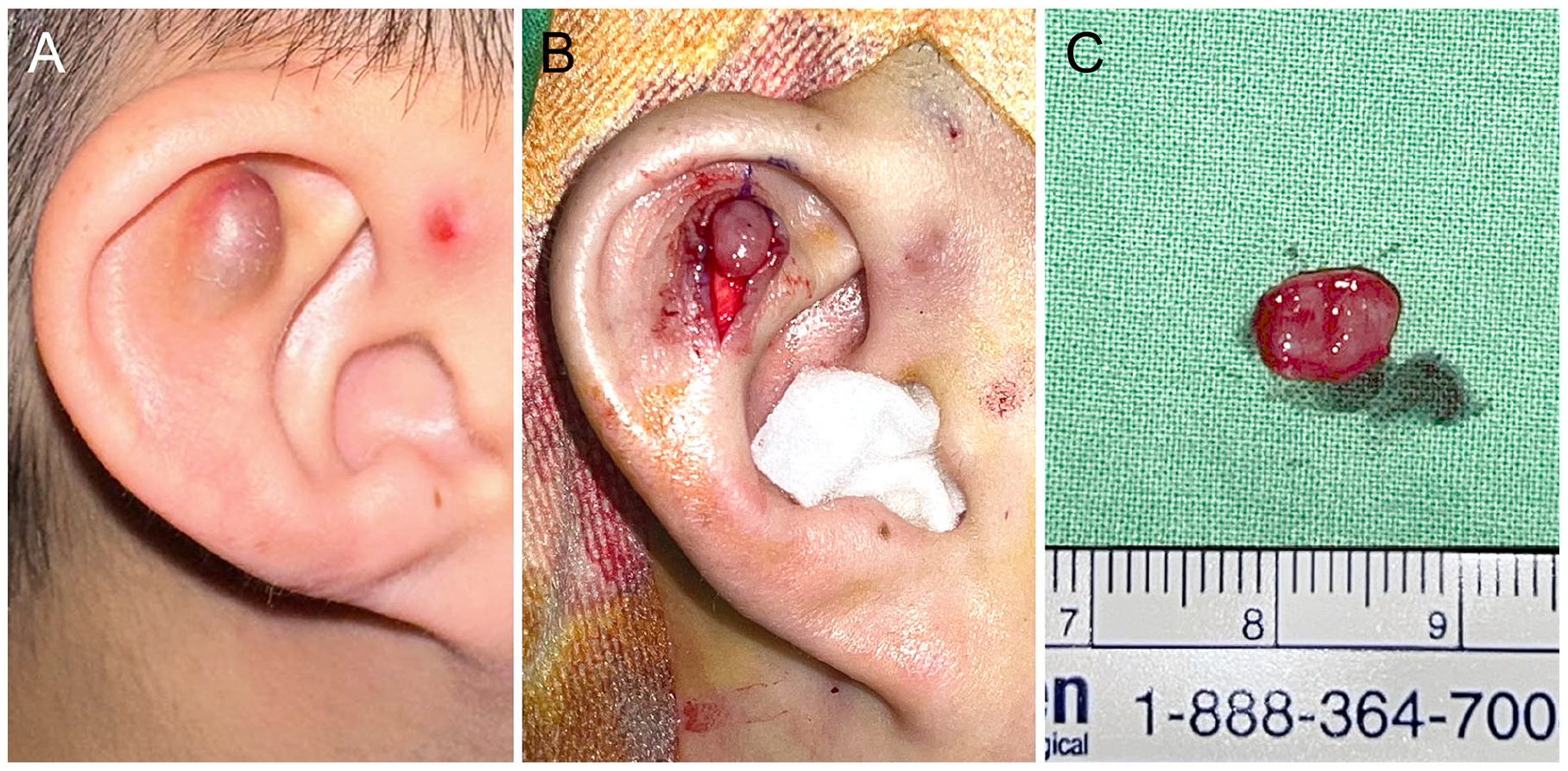
(A) Preoperative photograph of a soft-round mass in the right antihelix crura. (B) A curvilinear incision was made, and a well-encapsulated mass was identified within subcutaneous layer. (C) A specimen about 0.7 × 0.5 × 0.5 cm in size was shown.
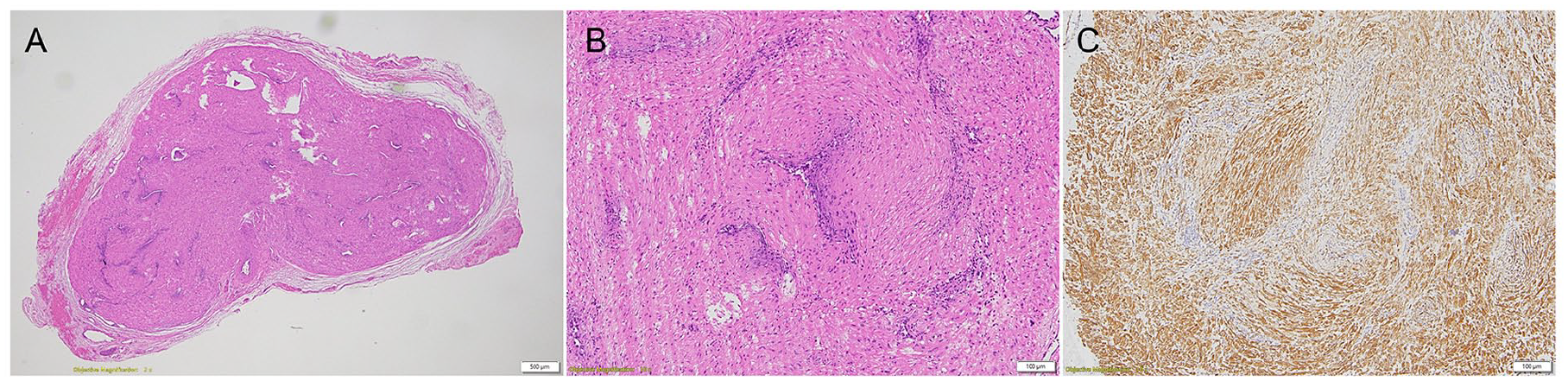
(A) A well-circumscribed nodule consisted of eosinophilic smooth muscle bundles (×20). (B) Numerous small slit-like, thin-walled vascular channels surrounded by smooth muscle bundles (×100). (C) SMA staining showed diffuse positive (×100). SMA, smooth muscle actin.
Discussion
VL is an uncommon benign tumor made up of blood vessels and smooth muscle, and it rarely occurs in the auricular region. 1 Morimoto proposed a classification system, which divided VL into solid, venous, and cavernous subtypes, providing insights into their varied clinical presentations. 2 Histologically, auricular VL predominantly manifests as solid or venous subtypes, characterized by smooth muscle bundles interlacing around variably-dilated vascular channels.2,4,5 The solid subtype, most frequent overall, consists of closely-compacted smooth muscle bundles that intersect and surround numerous small, slit-like vascular channels. The cavernous subtype consists of dilated vascular channels with relatively-smaller amounts of smooth muscle, with indistinct borders between vascular walls and surrounding bundles. In contrast, the venous subtype exhibits thick-walled vessels distinctly separated from less compacted smooth muscle bundles.1,2,6
Based on a thorough review of available literature, 22 cases of auricular VL have been reported to date (Table 1). Among these 22 cases, 17 patients (77%) were male, and 5 patients (22%) were female, indicating a male predominance. Auricular VL locations included the helix (6 cases, 27%), anterior surface of auricle (5 cases, 23%), posterior surface of auricle (5 cases, 23%), preauricular region (2 cases, 9%), antihelix (1 case, 4.5%), external auditory canal (1 case, 4.5%), and earlobe (2 cases, 9%). The tumors measured an average of 12 mm in diameter, ranging from 7 to 30 mm. Most lesions were asymptomatic (19 cases, 86%), though occasional symptoms such as intermittent pain, fullness, or hearing loss were reported in 3 cases (14%). Typically, auricular VL lesions appear as solitary, firm, well-defined nodules, usually measuring <2 cm. They are commonly asymptomatic, but intermittent pain or discomfort exacerbated by cold exposure, mechanical pressure, or stress has occasionally been reported, particularly in venous-type and carvenous-type lesions.7,8
List of Detailed Information of Auricular Leiomyoma Cases.
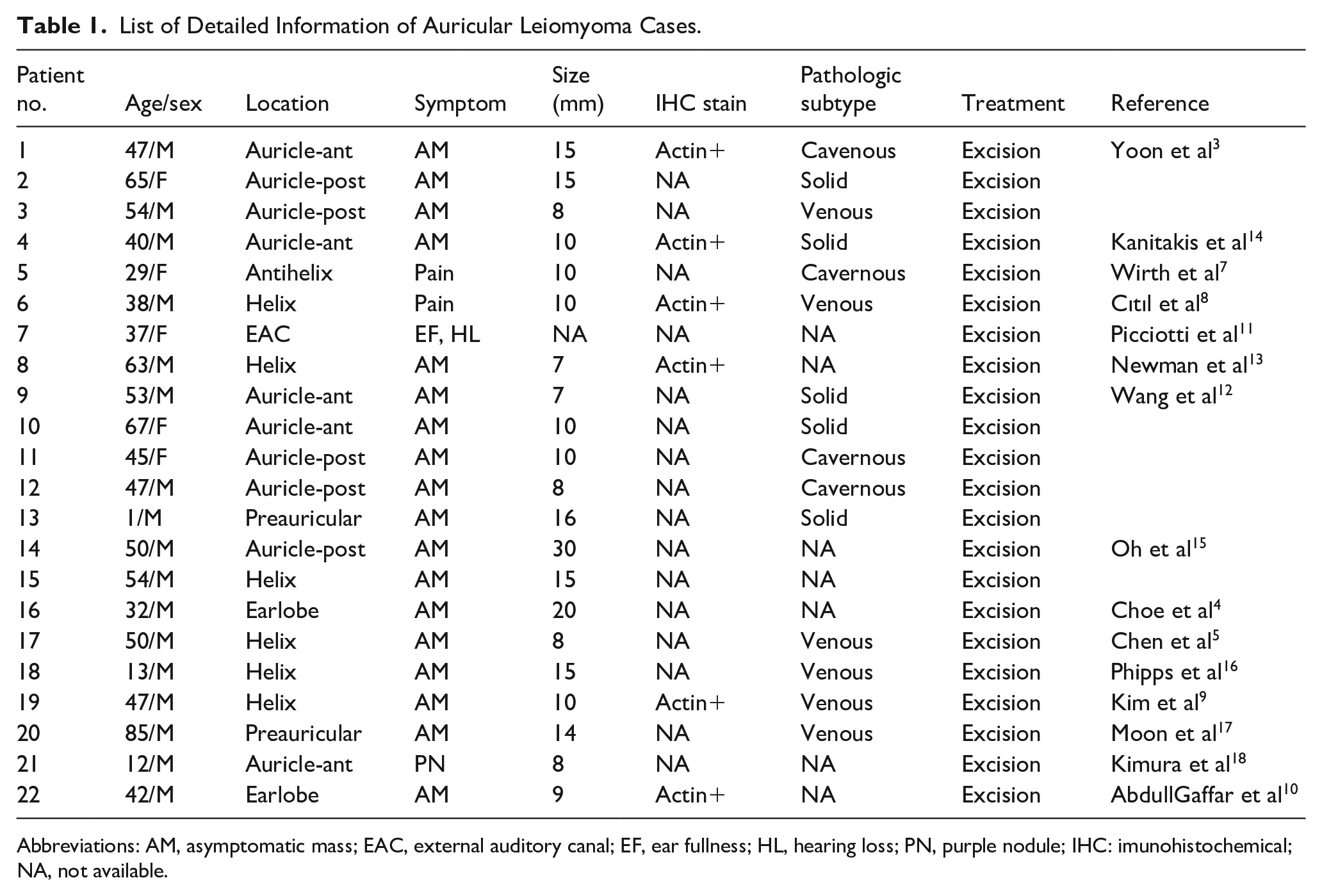
Abbreviations: AM, asymptomatic mass; EAC, external auditory canal; EF, ear fullness; HL, hearing loss; PN, purple nodule; IHC: imunohistochemical; NA, not available.
Immunohistochemical staining significantly aids in establishing a definitive diagnosis. Tumor cells consistently exhibit strong positivity for SMA and desmin, confirming smooth muscle origin.3,8-10 Additionally, endothelial cells stain positively for CD31, while S-100 protein is negative in smooth muscle cells but may highlight intratumoral nerves, aiding differentiation from schwannomas.9,10
Auricular VL is frequently misdiagnosed preoperatively due to its rarity and nonspecific clinical presentation. Clinicians should maintain a high index of suspicion when evaluating firm, well-circumscribed nodules in the auricular region. The differential diagnosis includes epidermoid cysts, hemangiomas, glomus tumors, angiolymphoid hyperplasia with eosinophilia, neurofibromas, and occasionally-malignant tumors like basal cell carcinoma and melanoma.9-11 Diagnostic imaging, including ultrasound and color Doppler, may reveal hypervascular lesions, yet definitive diagnosis primarily relies on histopathological examination of excised specimens.11,12
Complete surgical excision is the treatment of choice, with excellent prognosis and no recurrence reported in any of the 22 reviewed cases during follow-up periods ranging from 6 months to 7 years. Despite their uncommon occurrence, clinicians should maintain a high index of suspicion for auricular VL in the differential diagnosis of auricular nodular lesions to ensure accurate diagnosis and optimal management.3-6,9-13
Footnotes
Acknowledgements
This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-A-114002 to Hsin-Chien Chen).
Ethical Considerations
A written informed consent form was obtained from the patient and was approved by Tri-Service General Hospital Institutional Review Board.
Author Contributions
The specific role and contribution of each author is as follows: Cheng-Hung Lai: first author and preparation of draft. Hsin-Chien Chen: corresponding author and editing of manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-A-114002 to Hsin-Chien Chen).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.