
Abstract
Dysphonia and dysphagia are often observed among patients presenting to the otolaryngology clinic. One of the more common etiologies includes iatrogenic injury to the recurrent laryngeal nerve (RLN) as a known complication of head and neck surgeries such as thyroidectomy or anterior approaches to the cervical spine. Most often, RLN injury occurs in this context due to traction or transection of the nerve. No reports on delayed presentation of RLN injury from the extrusion of cervical spine hardware (screw) could be found in the peer-reviewed literature. We present a case of a 63-year-old woman who presented to the otolaryngology office with a 3-month history of hoarseness and difficulty swallowing. The patient’s past medical history was significant for a motor vehicle accident (MVA) 6 years prior resulting in right arm radiculopathy and subsequent anterior cervical discectomy with spinal decompression and fusion (ACDF) at C5-C6 and C6-C7 approximately 3 months after the MVA. Strobovideolaryngoscopy revealed right vocal fold immobility. Computed tomography scan revealed that a screw from the right side of the ACDF hardware migrated approximately 2 cm with compression of the RLN. The patient underwent neck exploration with removal of the extruded hardware and microdirect laryngoscopy with right vocal fold injection laryngoplasty. Intraoperatively, the extruded screw was found embedded within the RLN fibers. This case represents the first report to our knowledge of extrusion of cervical spine hardware screw resulting in delayed RLN injury and vocal fold paralysis.
Introduction
Hoarseness and difficulty swallowing are common chief complaints of patients who present to the otolaryngologist. Approximately 30% and 13% of the population will be affected by dysphonia and dysphagia, respectively, at some point in their life. 1 The differential diagnosis is quite broad, whereby infectious, inflammatory, neoplastic, neurologic, iatrogenic, or even multifactorial etiologies are considered. 2 The recurrent laryngeal nerve (RLN), a branch of the vagus nerve, is an important contributor to the muscles involved in voice and swallowing. Common procedures associated with iatrogenic injury of the RLN include thyroidectomy and anterior approaches to the cervical spine. We describe a case of delayed onset dysphagia and dysphonia following anterior cervical discectomy and fusion (ACDF) due to an extruded hardware screw resulting in injury to the right RLN.
Case Report
A 63-year-old woman presented to the otolaryngology office with worsening hoarseness and difficulty swallowing. Her past medical history was notable for a motor vehicle accident (MVA) 6 years prior and ACDF surgery at levels C5-C7 3 months after the MVA. Strobovideolaryngoscopy revealed an immobile right true vocal fold with vocal fold atrophy and bowing (Figure 1). A neck computed tomography (CT) scan was obtained, which revealed that the right C7 hardware screw had migrated nearly 2 cm, embedding into the posterior aspect of the thyroid gland along the right tracheoesophageal groove (Figure 1). The patient underwent right neck exploration with removal of the extruded screw and microdirect laryngoscopy with injection laryngoplasty of the right vocal fold. The right RLN was found to be adherent to the head of the extruded screw with splaying of the nerve fibers (Figure 2). The nerve remained intact after the screw was carefully dissected from the nerve. Nerve stimulation testing remained absent before and after the dissection. A vocal fold injection laryngoplasty was performed at the time of hardware removal. Postoperatively, the patient experienced satisfactory improvement in her voice and swallow without the need for any additional procedures. On her most recent follow-up, strobovideolaryngoscopy revealed improved atrophy of the right vocal fold, suggesting either partial recovery of the nerve function or that the injection provided a long-lasting effect.
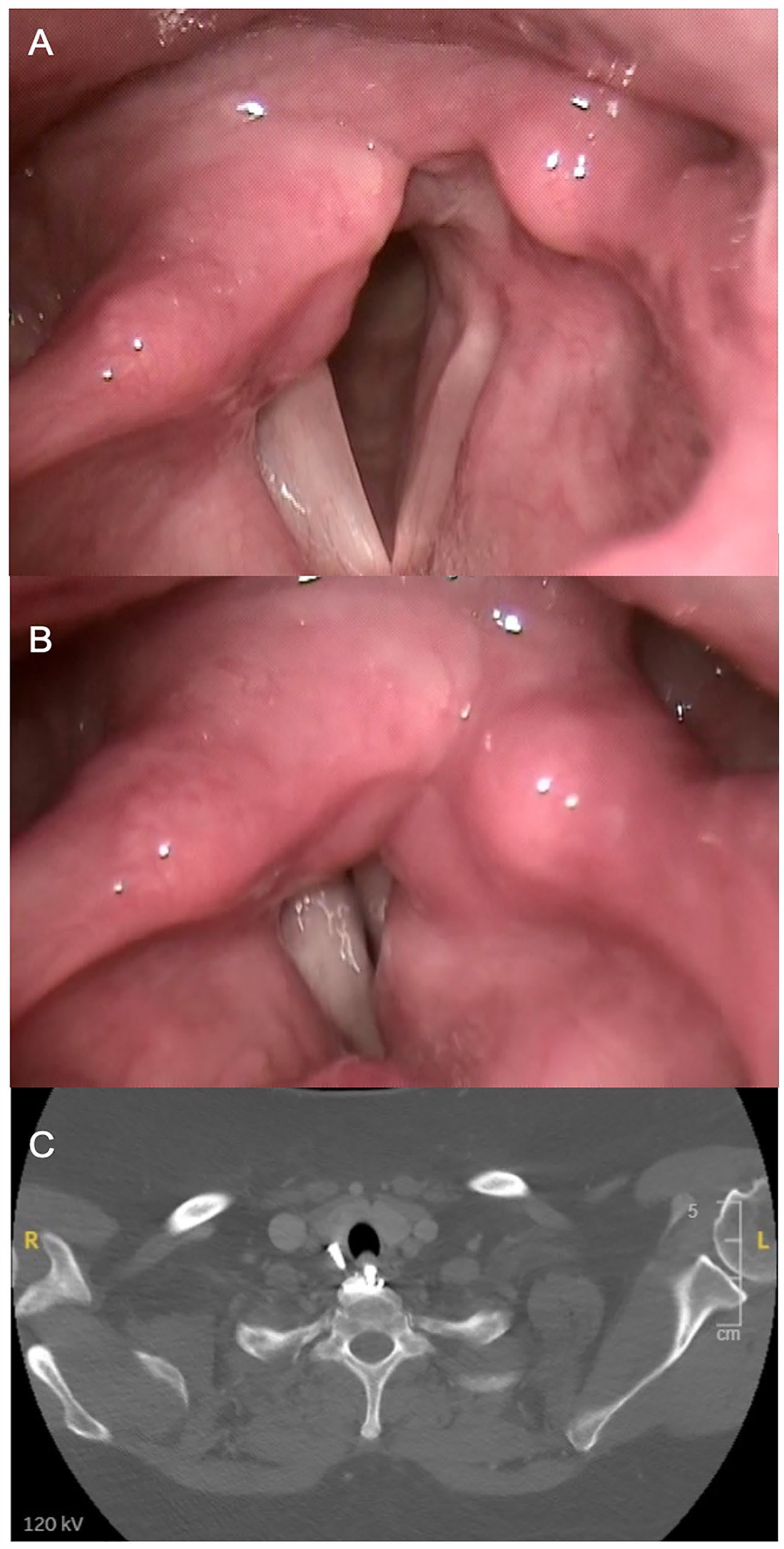
Pre-operative findings. Flexible strobovideolaryngoscopy findings reveal a right paralyzed vocal fold as evidenced by the vocal folds in abduction (Panel A) and adduction (Panel B). Panel C reveals axial-enhanced CT scan at the level of C7 showing a screw had migrated into the posterior aspect of the thyroid gland.
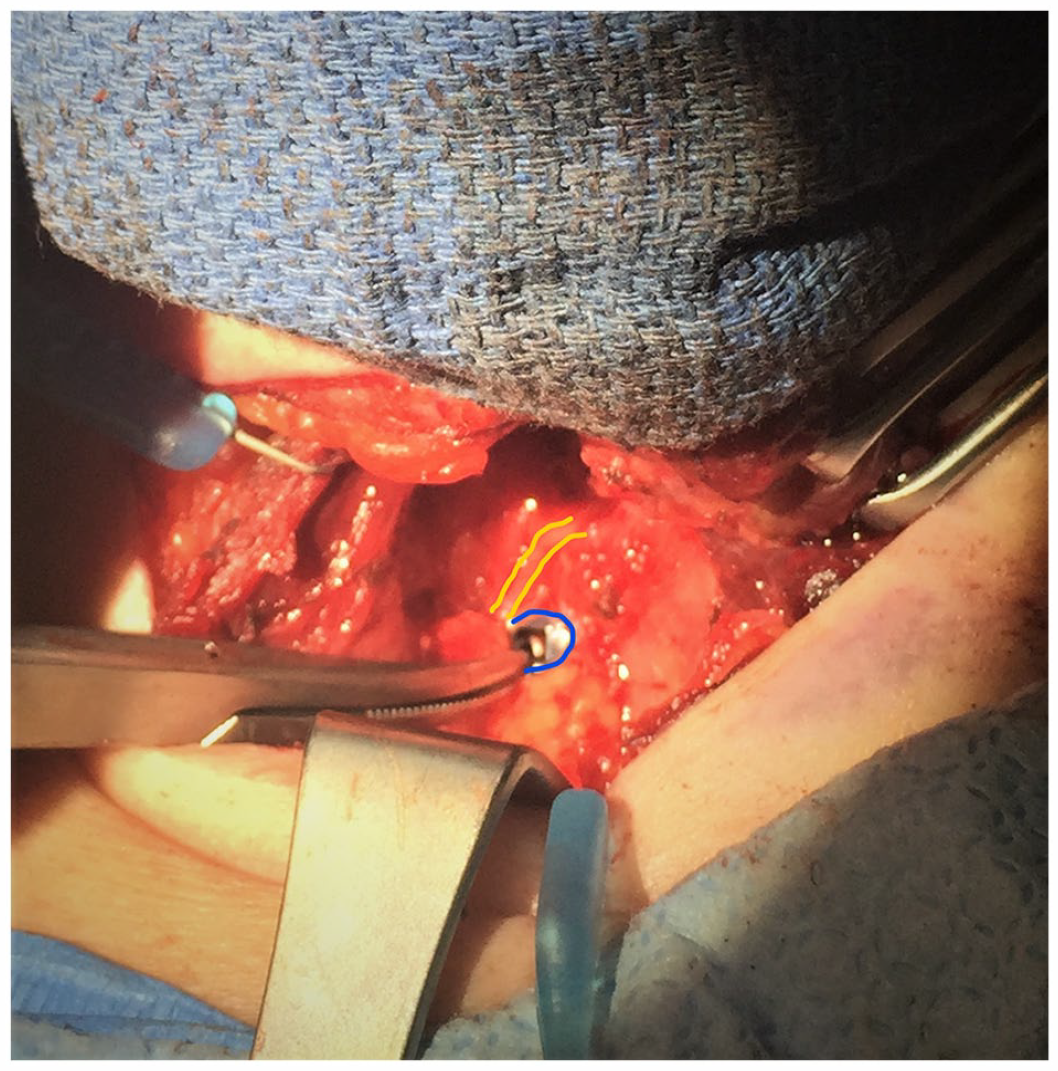
Intraoperative photograph displaying the relationship of the extruded screw (at the tip of the hemostat) medial and the RLN more lateral. The head of the screw is outlined in blue and the RLN is outlined in yellow.
Discussion
In the case presented, the time between symptom onset and the original surgery was approximately 6 years. Investigating the symptoms of hoarseness and difficulty swallowing begins with a complete history and physical examination of the head and neck, including strobovideolaryngoscopy. When vocal fold paralysis has been identified, diagnostic workup involves obtaining cross-sectional imaging from the skull base to the mediastinum for full evaluation of the ipsilateral vagus nerve. Despite the time delay to the development of symptoms in this case, attention to the past surgical history in conjunction with the CT findings was helpful in determining the cause.
Although injury to the RLN during ACDF is a reported complication, it is typically due to a traction injury or nerve transection. Rates of dysphonia after ACDF vary widely in the literature from 1% up to 60%.2,3 Additionally, the reported rate of dysphagia after ACDF can be as high as 70% in the immediate postoperative period. 3 The rates of both dysphagia and dysphonia have been found to decrease as the postoperative period progresses, suggesting return of baseline nerve function or compensatory innervations. 3
Few reports have been published regarding extruded cervical spine hardware leading to laryngopharyngeal manifestations and complications.4,5 Pharyngoesophageal complications from extruded hardware include pharyngoesophageal erosion or perforation. 5 These complications are rare and can be delayed by many years after the initial surgery. 5
Laryngeal manifestations from extruded hardware screws are even rarer. 4 The closest report involved an extruded screw from the odontoid that had migrated into the pharynx abutting the arytenoid, with effects on voice and swallowing. 4 In these rare events, hardware removal may become necessary to improve function and to avoid further injury.4,5 Our case is unique, given that the extruded screw from cervical spine hardware caused RLN injury and vocal fold paralysis.
Conclusion
Iatrogenic injury to the RLN from an extruded cervical spine hardware screw is extremely rare. To our knowledge, this is the first case reported in the literature. Adherence to recommended diagnostic workup protocols to include imaging of the vagus nerve when vocal fold paralysis is identified led to appropriate diagnosis and management for this patient. The possibility of extruded cervical spine hardware causing RLN injury remains in the differential diagnosis for vocal fold paralysis, even when symptom onset occurs many years after the surgery.
Footnotes
Acknowledgements
None.
Authors’ Note
This was presented at the ALA Annual Meeting 2023 held in Boston, Massachusetts on May 5-7, 2023 (Submission Entry ID#23-0116).
Author Contributions
Each author participated in developing the original concept for the article as well as chart review, data analysis, drafting the article, revisions, and final acceptance.
Data Availability Statement
Data are available through the patient’s electronic medical record and can be accessed through the patient’s providers only.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
St. Luke’s University Health Network IRB does not require ethical approval for reporting individual cases or case series of less than 5 patients.
Informed Consent
Informed consent was verbally obtained.
Trial Registration Number/Date
None.
Grant Number
None.