
Abstract
Epithelioid hemangioendothelioma (EHE) is an exceptionally rare vascular tumor with an incidence of <1/million people/year. This case report describes a patient who initially presented with progressive left-sided neck swelling and dysphagia and was found to have EHE at the confluence of the left subclavian and internal jugular veins. Diagnosis was confirmed with a core needle biopsy after an initial inconclusive fine-needle aspiration. Surgical management included direct laryngoscopy, left selective neck dissection (levels 2-4), left internal jugular vein sacrifice, and vascular reconstruction with a saphenous vein graft, followed by adjuvant radiation therapy due to positive margins. Early recognition of EHE in complex anatomical locations is essential and requires a multidisciplinary approach for optimal diagnosis and treatment.
Introduction
Epithelioid hemangioendothelioma (EHE) is a rare vascular tumor that accounts for <1% of all vascular neoplasms, with an estimated incidence of 0.23/million person-years. 1 EHE has a variable clinical picture owing to its low-grade malignancy and high-grade malignancy potential. 2 EHE most commonly affects the liver, lungs, and soft tissue, with limited cases reported in the head and neck region. 3 Presentation in the head and neck includes nonspecific symptoms of painless or progressive swelling, dysphagia, or airway obstruction. 4 Cases reported in the head and neck region involved the oral cavity, larynx, thyroid, and cervical soft tissues. However, findings within major vascular structures, such as the confluence of the left subclavian and internal jugular vein, are exceptionally rare with unique diagnostic and therapeutic challenges. 5
The etiology of EHE remains unclear and contributes to the difficulty in characterizing and diagnosing this vascular tumor. Molecular studies have suggested that the WWTR1-CAMTA1 fusion gene plays a critical role in tumorigenesis. 6 The WWTR1-CAMTA1 fusion gene is found in 90% of cases of EHE and is consequently pathognomonic for this disease.6 -8 The YAP1-TFE3 fusion gene has been associated with a novel phenotype of EHE that affects younger populations with a mean age of 30 years. 9 EHE is strongly associated with the immunohistochemical markers of CD31, CD34, ERG, D2-40, and FLI-1.10,11 The histological characteristics of EHE show nests and cords of pleomorphic epithelioid cells with intracytoplasmic vacuoles within a hyalinized or myxochondroid stroma. 12 These histological characteristics are therefore essential to the accurate diagnosis of EHE.
The optimal management of EHE remains controversial due to its variable presentation and the lack of standardized treatment guidelines. For localized EHE, complete surgical excision with clear margins is the preferred approach in the head and neck. 13 In cases that involve complex vasculature, such as the subclavian and internal jugular veins, surgical resection often requires additional vascular reconstruction. 14 Adjuvant therapy involving radiation and anti-angiogenic agents may be required for cases with positive margins, unresectable disease, or distant metastases. 15 These challenges often require a multidisciplinary team involving otolaryngologists, vascular surgeons, radiologists, pathologists, and oncologists for optimal treatment.
Herein, we present a rare instance of EHE at the confluence of the left subclavian and internal jugular veins. Highlighting the diagnostic complexities, surgical challenges, and importance of a multidisciplinary team to optimally treat this rare vascular malignancy. The objective of this report is to contribute to the growing knowledge of EHE in the head and neck region to optimize diagnostic and treatment approaches.
Case Description
This case study follows a 65-year-old female with a past medical history of hypertension, gastroesophageal reflux disease without esophagitis, and Hashimoto’s thyroiditis. Her past surgical history includes an umbilical hernia repair and dental surgery involving upper and lower implants. She reported a brief history of cigarette smoking for 1 to 2 years in her 20s but has not smoked since. She denied any history of alcohol consumption or recreational drug use.
She presented to the clinic after experiencing persistent symptoms of intermittent dysphagia and a progressive enlargement of a level II left neck mass over a 6-month period. Around the same time, she was diagnosed with Hashimoto’s thyroiditis, for which she was receiving thyroid hormone replacement therapy. A thyroid ultrasound was conducted to examine the persistent symptoms and neck mass, which detected a benign 3 mm nodule in the left lobe of her thyroid. There were no nodules in the right lobe of her thyroid. However, a prominent left supraclavicular lymph node measuring 1.8 × 1.9 × 2.5 cm was observed during the ultrasound examination and raised concerns about its potential pathologic appearance. An ultrasound-guided fine-needle aspiration (FNA) of the lymph node was subsequently conducted and indicated a normal appearing lymph node with normal flow cytometry results. An esophagogastroduodenoscopy was performed to evaluate her progressive dysphagia, which showed no esophageal masses or concerning lesions. A positron emission tomography (PET) scan was conducted and revealed a 1.5 cm hypermetabolic left supraclavicular node, further raising suspicion for malignancy. This prompted the need for a core needle biopsy of the supraclavicular lymph node due to the prior inconclusive FNA results. The core needle biopsy confirmed the diagnosis of EHE based on the histopathologic presence of pleomorphic epithelioid cells within a myxochondroid stroma, along with positive immunohistochemical markers of CD31, CD34, ERG, D2-40, and CAMTA1.
The patient’s case was reviewed by a multidisciplinary tumor board including specialists from hematology and oncology, radiation oncology, pathology, otolaryngology, and radiology. The board recommended surgical excision of the mass per National Comprehensive Cancer Network guidelines for EHE. The findings were discussed with the patient, and she elected to pursue surgical excision of the mass. A direct laryngoscopy was performed in the operating room due to PET scan activity within the left tonsillar region. However, no abnormalities were observed in the pharynx other than bilateral cryptic tonsils.
A neck dissection of levels II to IV was performed with identification and preservation of key anatomical structures. The facial vein was identified, ligated, and divided, while the hypoglossal and spinal accessory nerves were identified and preserved. Further dissection revealed a firm vascular mass intrinsic to the inferior aspect of the left internal jugular vein, with involvement of the subclavian vein and in close proximity to the vagus nerve. Careful dissection allowed tumor separation from the vagus nerve, preserving its function. The hypoglossal, spinal accessory, and vagus nerve were preserved. Multiple enlarged lymph nodes were noted within levels II through IV. The internal jugular vein with the endoluminal tumor was then clamped, divided, and resected from its junction with the subclavian vein up to its confluence with the facial vein with assistance from the vascular surgery team. Vascular reconstruction was performed by patch angioplasty with a 3-cm saphenous vein patch at the junction of the subclavian and innominate vein (Figures 1–7).
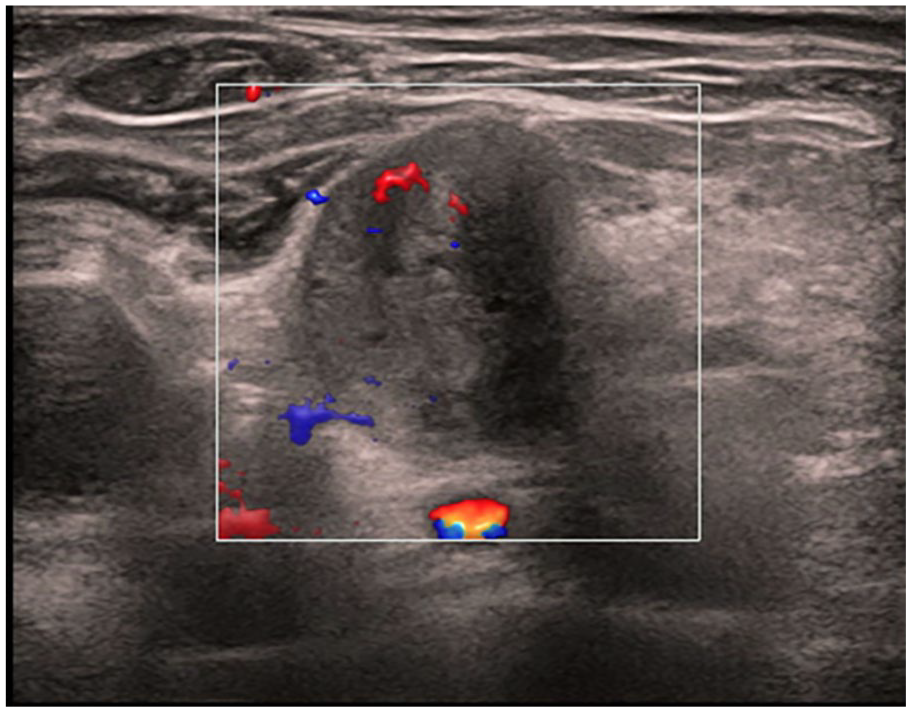
Ultrasound image of the left supraclavicular region showing an enlarged and hypoechoic lymph node. Increased vascularity is noted on Doppler imaging.
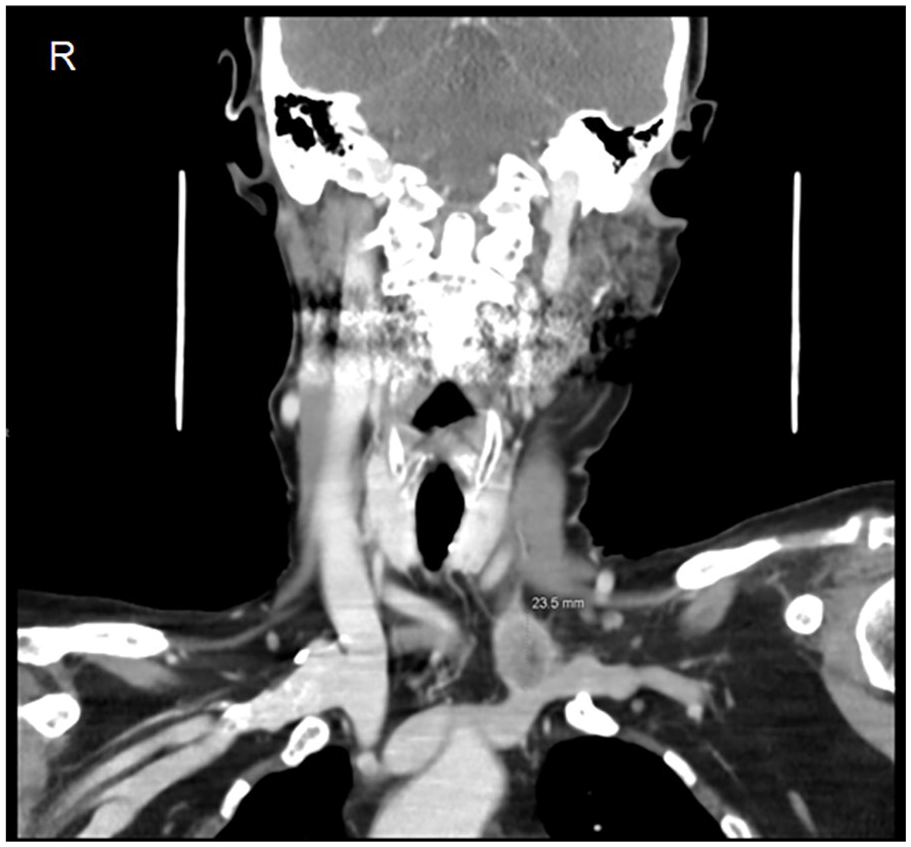
Contrast-enhanced coronal computed tomography scan of the head showing a heterogeneous enhancing mass measuring 23.5 × 21.9 × 21.3 mm at the confluence of the left internal jugular and left subclavian vein.
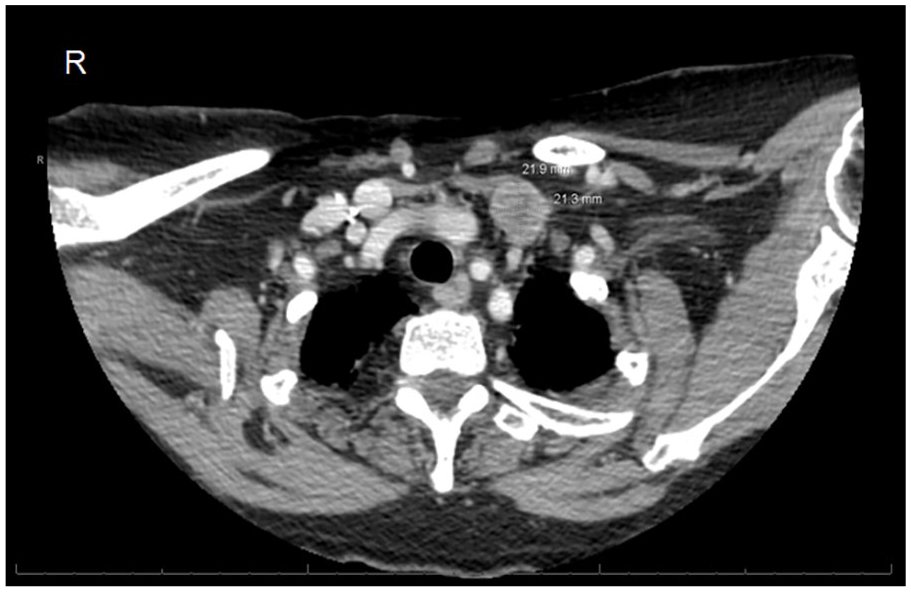
Contrast-enhanced axial computed tomography scan demonstrating the well-defined soft tissue mass measuring 23.5 × 21.9 × 21.3 mm in the left cervical region.
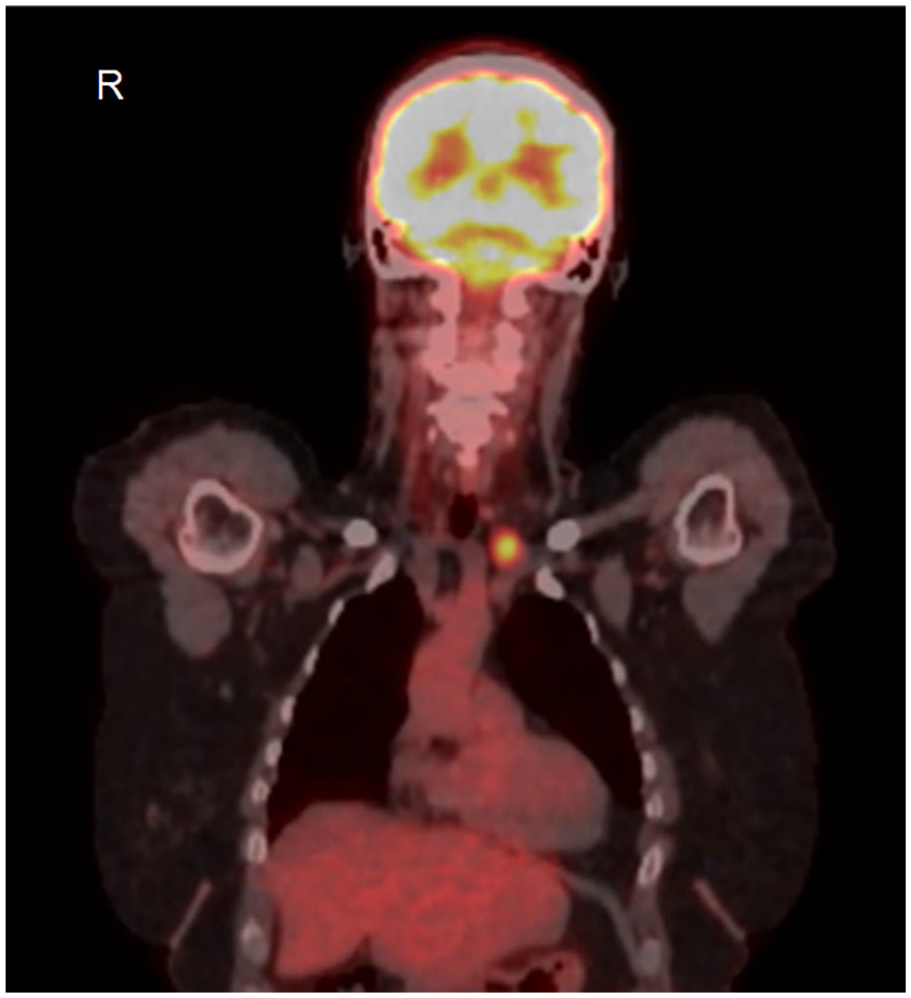
Whole body axial PET scan highlighting the hypermetabolic mass between the left internal jugular vein and left subclavian vein in the anterior mediastinum. PET, positron emission tomography.
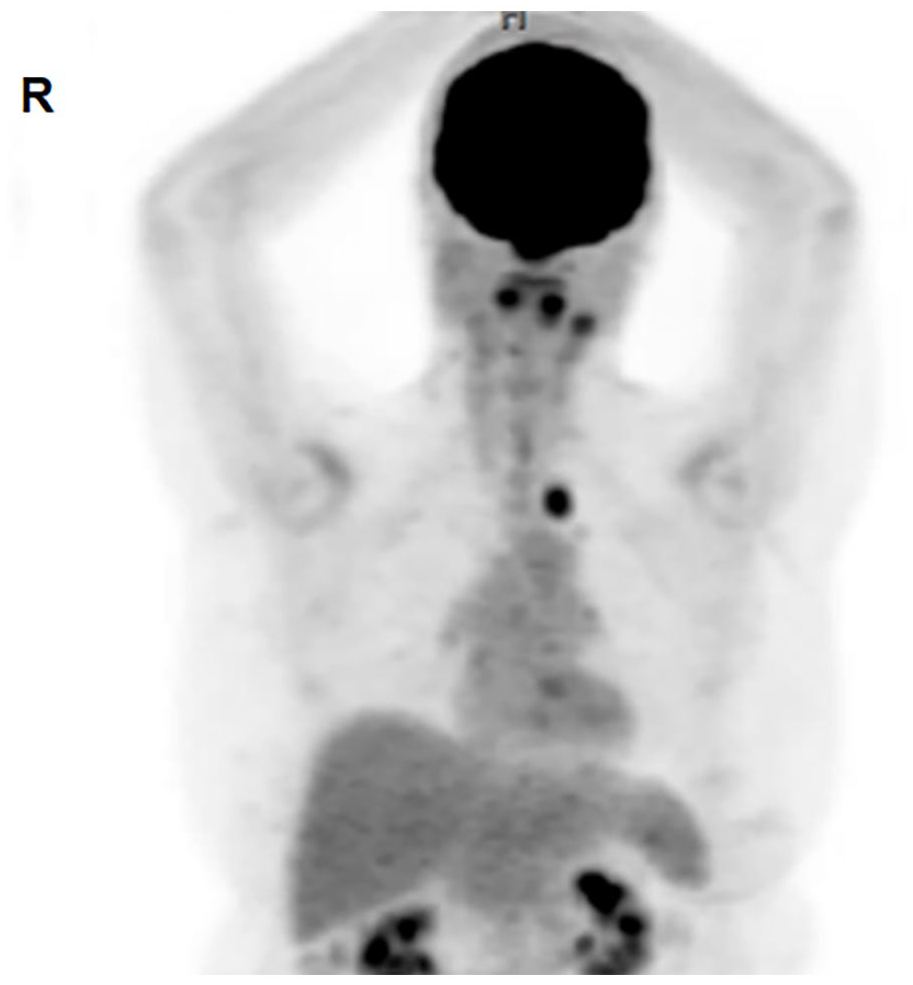
Whole body axial PET scan indicating the activity found within the left tonsillar area necessitating the direct laryngoscopy. PET, positron emission tomography.

Intraoperative image of the resected segment of the left internal jugular vein with visible endoluminal pathologic tissue.

Intraoperative image highlighting the preserved left vagus nerve attached to a red vessel loop after meticulous dissection from the adjacent tumor mass.
Postoperative pathology tissue examination of the mass confirmed EHE with positive histochemical markers of CD31, CD34, ERG, D2-40, and CAMTA1 (Figure 8). The mass, measuring at 2.4 × 2.2 × 1.4 cm, was red-tan in color and well-circumscribed within the lumen of the internal jugular vein. The 26 regional lymph nodes examined in levels II through IV were negative for tumor involvement. However, tumor involvement was present in the inferior jugular vein margin.
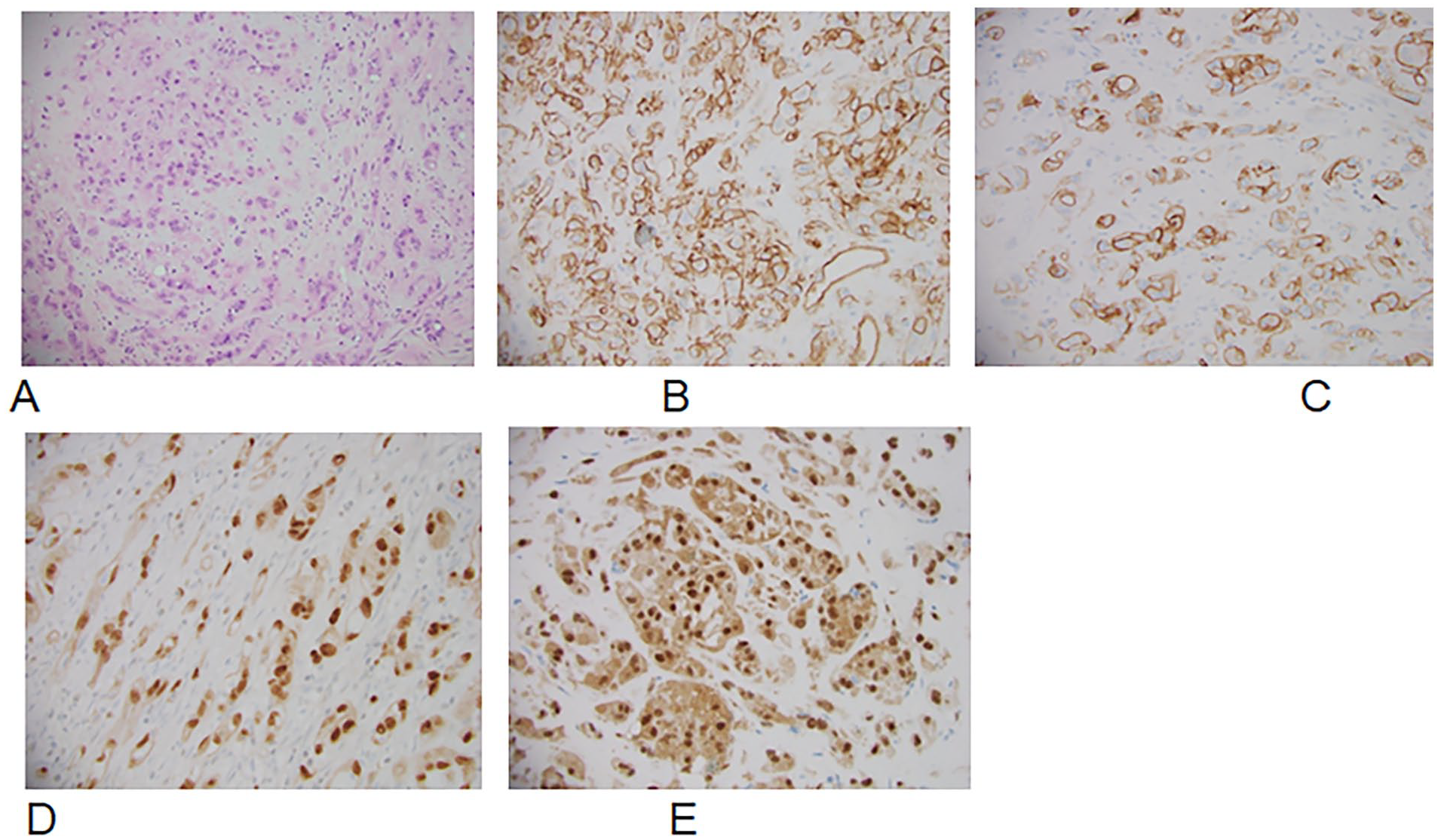
Postoperative pathologic analysis revealed epithelioid tumor cells characterized by abundant eosinophilic cytoplasm (A). These cells are arranged in cord-like structures within a myxohyaline stroma. Immunohistochemical analysis demonstrates expression of vascular markers CD31 (B), CD34 (C), and ERG (D) in the tumor cells. The diagnosis is further confirmed by CAMTA1 (E) expression.
The patient made an unremarkable postoperative recovery. Her case was presented to the multidisciplinary tumor board once again following the surgical excision of the mass, with the recommendation of adjuvant radiation treatment due to positive margins. At the time of this writing, the patient completed radiation and is disease free.
Discussion
EHE is a rare vascular tumor with intermediate-grade malignant potential that arises from endothelial cells. 16 EHE commonly presents in the liver, lungs, and soft tissue, with presentation in the head and neck region being uncommon. Its variable clinical presentation makes early diagnosis and treatment a significant challenge. Patients may present with progressive swelling, dysphasia, hoarseness, or vascular symptoms depending on the location of the tumor. In this case, the progressive swelling in the left supraclavicular region and dysphagia prompted further investigation. Initial imaging with ultrasound and PET scan was effective in our evaluation of the mass and its malignant potential. Further diagnostics with an FNA failed to provide a definitive diagnosis, likely due to the inadequate tissue sample size required for accurate histopathologic and immunocytochemical analyses. Consequently, a core needle biopsy was ultimately necessary to confirm the diagnosis. This case highlights the importance of a careful multimodal diagnostic approach in identifying EHE.
The histopathology of EHE is often characterized by epithelioid endothelial cells within a myxoid or fibrous stroma with a strong association with the immunohistochemical markers of CD31, CD34, ERG, D2-40, and FLI-1.10,11 Although initial flow cytometry results were inconclusive, this case reinforces the necessity of thorough tissue analysis, as the diagnosis was established based on repeat histopathologic and immunohistochemical findings.
For localized EHE, surgical excision remains the best treatment modality despite the lack of standardized treatment protocols. However, the vasculature involved in this case posed a considerable challenge. The tumor’s extension into the internal jugular and subclavian veins required a collaborative approach with a vascular surgery team to reconstruct the affected vasculature with a saphenous vein graft. A sternotomy was initially considered due to the location of the tumor and its possible extension, but based on preoperative imaging outlining the location of the mass, it was determined that a curvilinear incision along the left neck through levels II through IV would be sufficient for this case. The mass’s abutment to the vagus nerve was another challenge that required meticulous dissection to preserve its function.
Due to the positive surgical margins, adjuvant treatment with radiation was recommended. This is often required in cases with aggressive histopathologic features or incomplete resection of the mass. 17 Studies have shown the efficacy of antiangiogenic therapy on EHE, but these treatment strategies are more appropriate for metastatic EHE. 18 Close oncologic surveillance is still required for this case to monitor for recurrence and potential metastases.
Conclusion
This case highlights the diagnostic and treatment complexities of EHE in the head and neck region. Early recognition, multidisciplinary collaboration, and careful surgical planning were crucial for optimal treatment of our patient. Given the rarity of head and neck EHE, further studies are needed to establish a standardized treatment protocol and evaluate the usage of emerging systemic therapies for local and metastatic diseases.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Informed written consent was obtained from the patient for their anonymized information to be published in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.