
Abstract
Lymphomas of the larynx are a rare finding. Those with lymphoma of the larynx often present with symptoms such as vocal hoarseness, throat pain, dysphagia, and weight loss. This is a case of a 74-year-old man who presents with new onset of hoarseness and dysphagia. He has a previous history of diffuse large B-cell lymphoma (DLBCL) but was thought to be in remission at the time of presentation. On nasolaryngoscopy, there was a large, right sided, sub-mucosal mass with right vocal cord fixation. Physical exam and computed topography of the neck did not identify any adenopathy. Biopsy confirmed the recurrence of DLBCL isolated to the larynx at the time of diagnosis. The patient was treated with chemotherapy and fully recovered his vocal cord motion with resolution of his hoarseness and dysphagia. Physicians should consider lymphoma in patients presenting with laryngeal complaints especially in patients with a history of lymphoma.
Introduction
Extra-nodal lymphomas of the larynx are a rare presentation of lymphoma. The exact number of cases identified per year is unknown. Primary lymphomas of the larynx are likely less than 1% of all malignancies located in the head or neck. 1 Although not as rare as primary, secondary lymphomas of the larynx represent a minority of head and neck lymphomas. 1 There are common presenting symptoms among patients with laryngeal lymphoma. The major presenting symptoms and severity of symptoms vary based on anatomy involved. Often patients complain of hoarseness, throat pain, and dysphagia. There can also be night sweats, fever, and weight loss often referred to as “B-symptoms.” 2 In the literature, there are no mentions of a fixed vocal cord on presentation as in this case.
Case Report
The patient is a 74-year-old man who presented in the summer of 2021 to the outpatient otolaryngology clinic with complaints of hoarseness, dysphagia, and weight loss. He did not have any known risk factors for laryngeal carcinoma. He was currently healthy and not on any medications. His past medical history was significant for diffuse large B-cell lymphoma (DLBCL) diagnosed in 2013. His adenopathy was restricted to his truncal area without bone marrow involvement. At that time, he was treated with R-CHOP (rituximab, cyclophosphamide, doxorubicin hydrochloride, vincristine, and prednisolone) with a positive response to therapy and no residual disease. However, in 2018, he developed pulmonary symptoms consistent with recurrence. Lung biopsy confirmed the recurrence of DLBCL. He was treated with R-ICE (rituximab, ifosfamide, carboplatin, and etoposide phosphate) and responded well to therapy. At the time of presentation, he was believed to be in remission.
At presentation, the patient had dysphonia with a voice that was breathy in quality. A flexible fiberoptic nasolaryngoscopy revealed a mass along the right vocal cord and arytenoid. The right vocal cord motion was fixed with no motion. There was normal motion of the left vocal cord. A computed tomography (CT) of the neck confirmed the presence of a right-sided supraglottic and glottic mass (Figure 1). No lymphadenopathy was identified on physical exam or CT. A CT of the neck showing right-sided laryngeal involvement of tumor (arrow).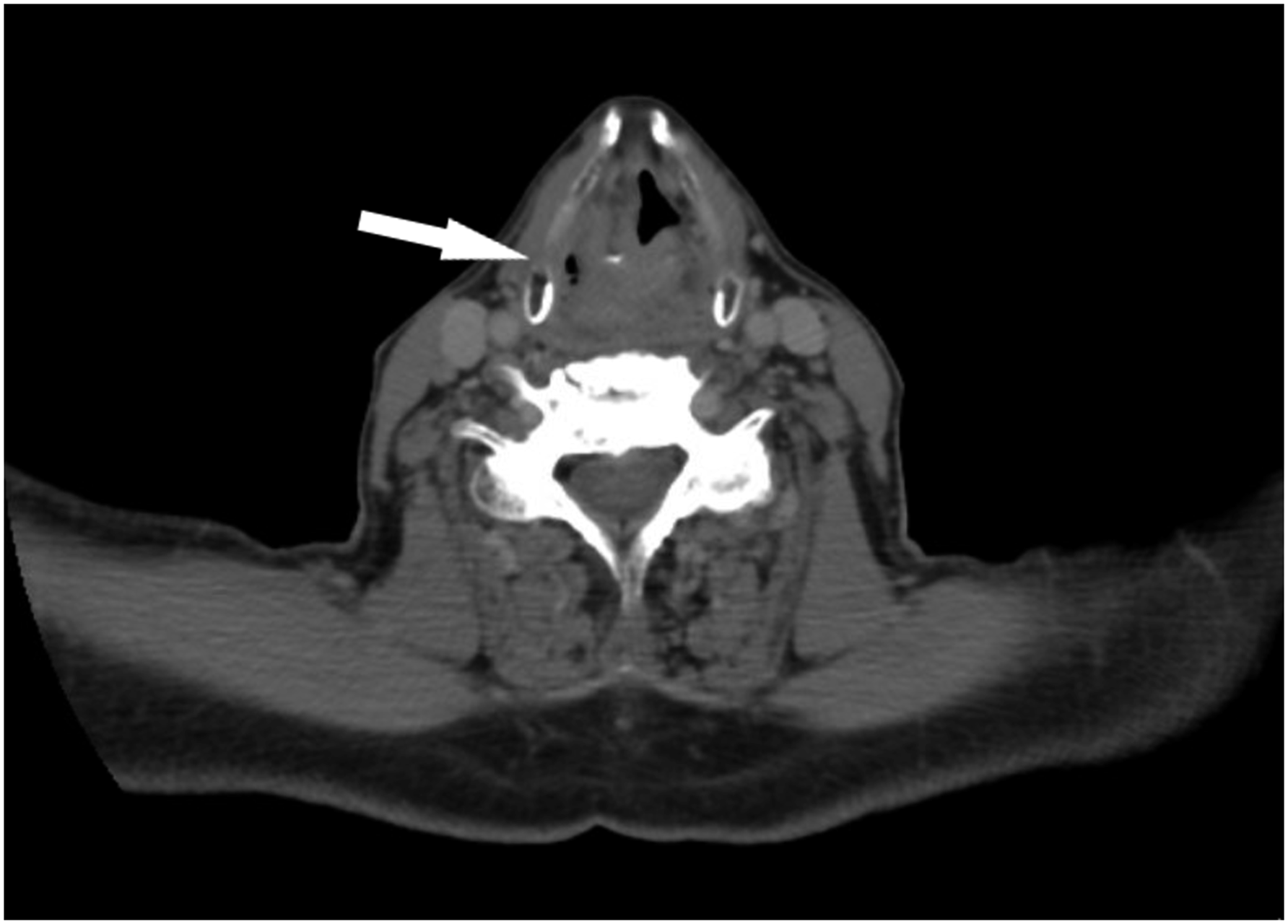
Biopsies were then obtained in the operating room via direct laryngoscopy. Tissue obtained from the right vocal cord and right arytenoid was diagnosed as high-grade B-cell lymphoma. Immunostains of tumor cells were positive for cluster of differentiation (CD)20, CD79a, CD45, and Ki-67. Staining was negative for CD3, CD10, and pankeratin. Positron emission topography (PET) scan identified an intense C-shaped area with intense activity at the right vocal cord region extending into the laryngeal space on the right side (Figure 2). A low level of intensity was identified in the left submandibular gland and right lateral neck region. Positron emission topography identifying an intense C-shaped activity at the right vocal cord region extending into the laryngeal space.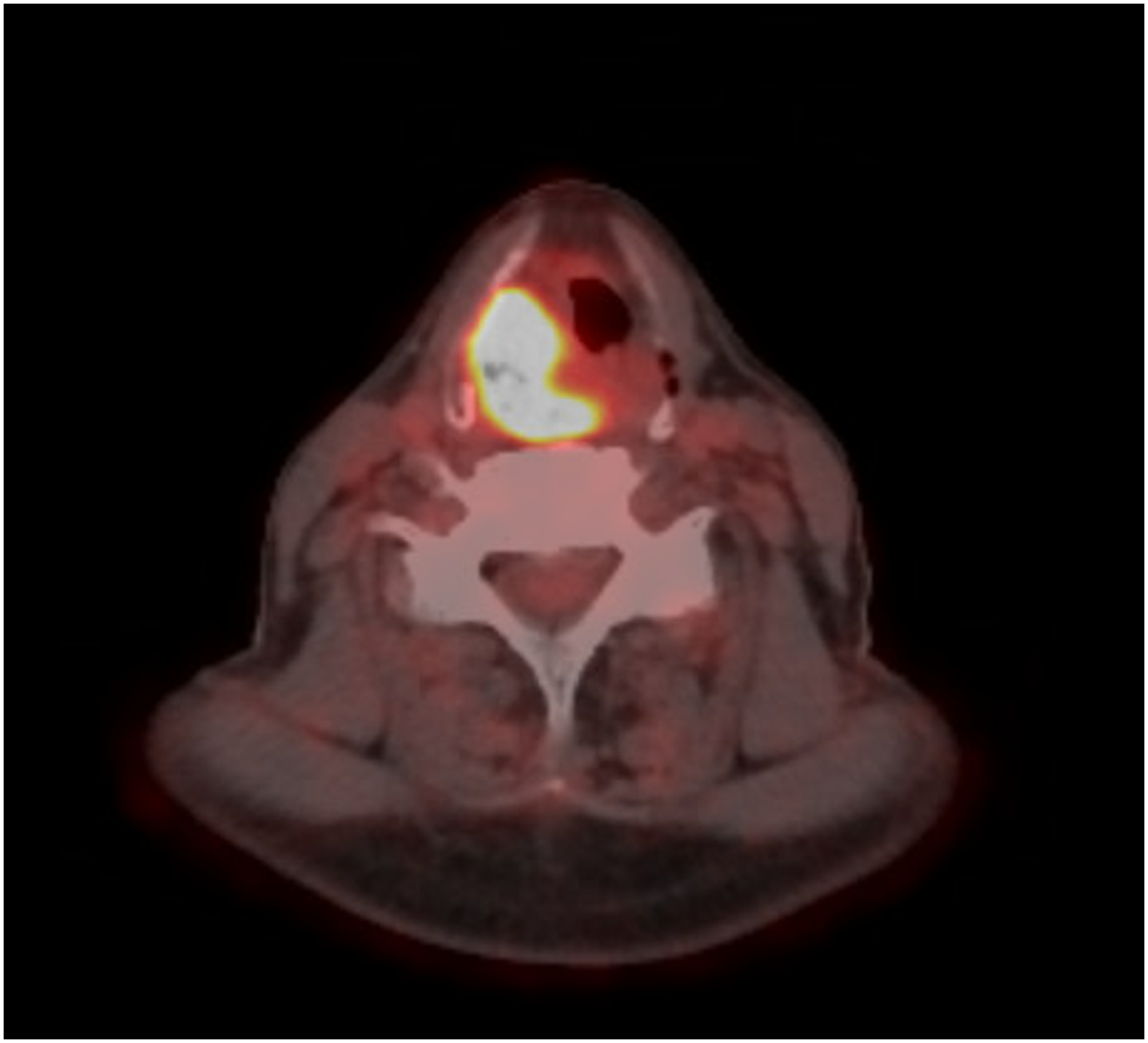
After oncologic referral and assessment, the patient was treated with definitive localized radiation. Intensity modulated radiation therapy techniques were used for a total dose of 55 Gray in 25 fractions. Additionally, immunotherapy with monoclonal antibodies to CD20 (rituximab) was used. At the 3 month follow-up, the patient was doing well and had completed radiation therapy. Flexible nasolaryngoscopy showed a normal appearing larynx and return of function to the right vocal cord with full mobility (Figure 3). The patient reports improvement of his voice with minimal dysphagia. Flexible nasolaryngoscopy showing a normal larynx with full vocal fold motion following therapy.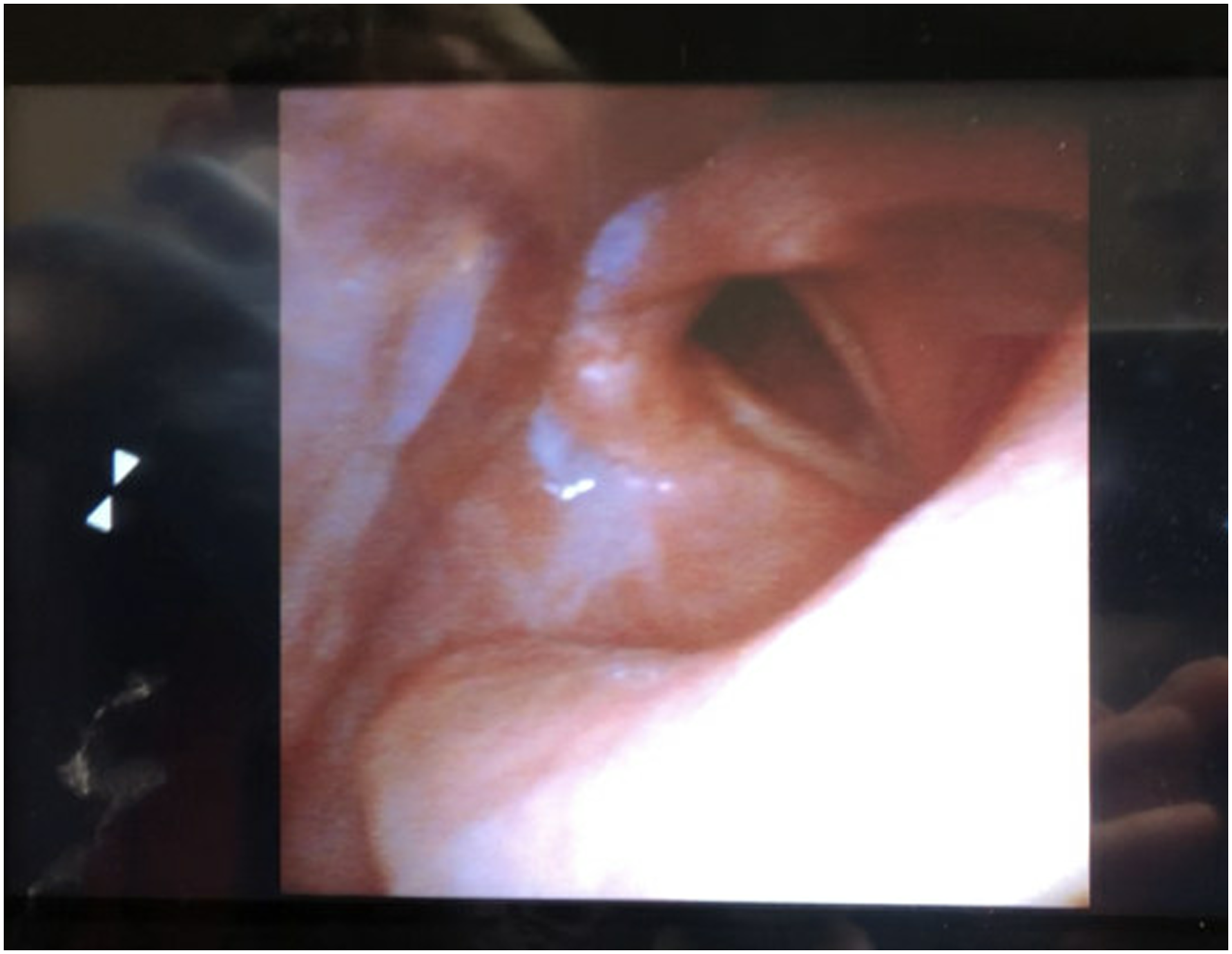
Discussion
Lymphoma of the larynx is a rare location for this pathology. Hoarseness and dysphagia are common presenting signs for laryngeal lymphomas. However, a lymphoma recurrence presenting as a fixed vocal fold has not been presented in the literature. This case demonstrates the need for a thorough work up of various laryngeal complaints.
Extra-nodal lymphomas of the larynx are a rare presentation of lymphoma.1 A large retrospective case series (n = 115) in China showed that there is a male predominance (77% males and 33% females). 3 Additionally, non-Hodgkin’s lymphoma was the exclusive pathological type. 3 A larger study with cases from the United States had similar findings. Of 200 cases, 53% were males and all cases were identified as non-Hodgkin’s lymphoma, with B-cell lymphoma as the most common (74%) type. 4
There are common presenting symptoms among patients with laryngeal lymphoma. The major presenting symptoms and severity of symptoms varied based on anatomy involved. Hoarseness was the most common presenting symptom (70.2%), followed by throat pain (26.3%) and dyspnea (17.5%). Only 12.5% of patients presented with dysphagia. B-symptoms such as night sweats, weight loss, and fever were present in 14.0% of patients. 2
Because of the rarity of laryngeal lymphoma, no treatment guidelines have been established. Typical therapy includes chemotherapy and/or radiation therapy. 5 There is rarely a role for surgical resection. As in this case, these malignancies are often responsive to treatment. Yet the recurrence rates are unknown for this location of lymphoma.
The larynx is a rare location for lymphomas. A lymphoma presenting as vocal fold fixation has not been reported elsewhere. Physicians should consider lymphoma in patients presenting with laryngeal complaints especially in patients with a history of lymphoma. Currently, there is no consensus for a standardized treatment for laryngeal lymphoma. However, chemotherapy and radiation have produced remarkable results. This case demonstrates the efficacy of therapy with a profound resolution of vocal cord fixation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
Informed consent was obtained prior to writing this report.