
Abstract
Introduction
Supernumerary teeth, with a prevalence of 1% to 3%, are more common than other oral surgical conditions. They occur frequently in the maxillary anterior region,1-6 although they have also been reported in the nasal cavity. 6 However, intranasal supernumerary teeth are rarely encountered in daily clinical practice and therefore are currently not diagnosed or treated systematically.
In addition to presenting a case with an intranasal supernumerary tooth, which we treated, we analyzed the relevant literature and conducted a clinical examination to establish systematic methods for diagnosing and treating intranasal supernumerary teeth.
Patients and Methods
We searched the PubMed database for literature on intranasal supernumerary teeth, published from 1990 to 2019. We identified 308 cases in 237 papers. We were able to obtain the relevant data for 131 cases (103 papers). Combined with a case that we experienced and report here, we included 132 cases in our analysis (Figure 1). We included only cases in which there were no jaw deformities (cleft lip and palate, etc.) and in which only supernumerary teeth were impacted. This study was approved by the institutional review board of Saitama Yorii Hospital (approval number: Y-211123.0). All participants provided written informed consent.
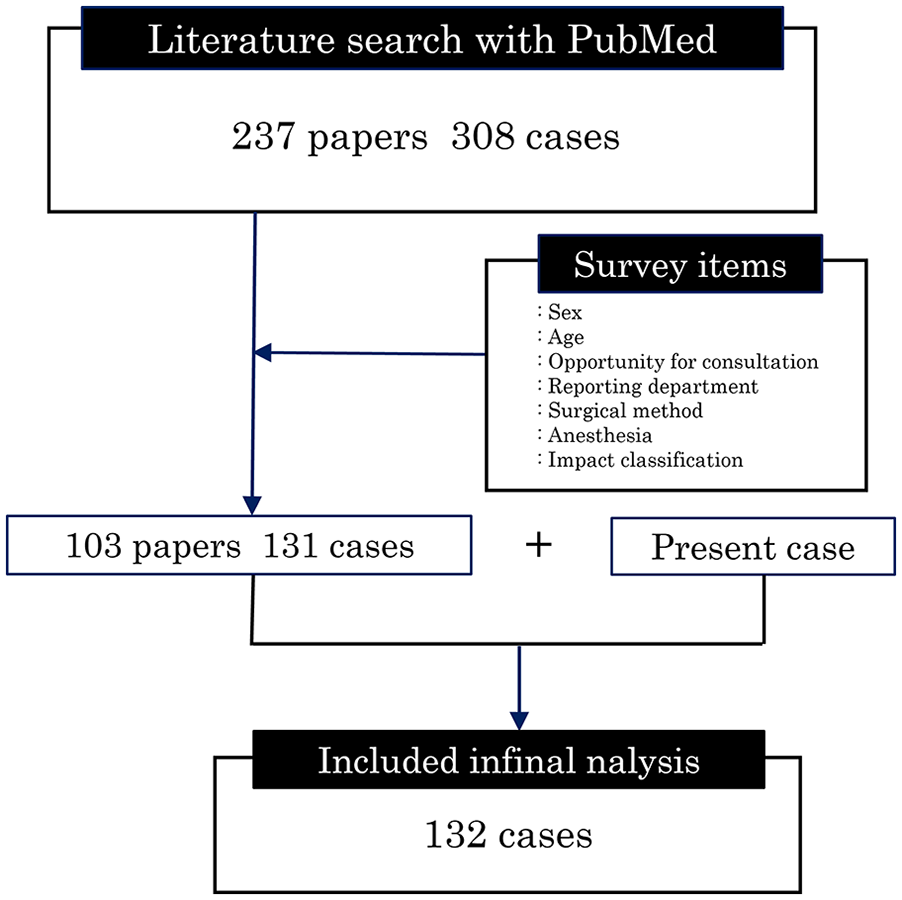
PubMed literature search.
We recorded the following data items: sex, age, reason for consultation (chief complaint), reporting department, supernumerary tooth impact classification (left, right, center), surgical approach used for its removal (nasal, oral vestibular, palatal) and its relationship with impaction position, and anesthesia (general or local) and its relationships with the surgical approach and impaction position.
Based on diagnostic imaging, we classified intranasal supernumerary teeth according to their vertical and anterior-posterior positions relative to the maxilla (Figure 2). The vertical position was classified as follows, with the axis of the alveolar bone as the central axis: bone impact with one-third or less of the total supernumerary tooth length or intramucosal impact was defined as Class I; bone impact with one-third to two-thirds of the total tooth length was defined as Class II; and bone impact with two-thirds or more of the total tooth length was defined as Class III (Figure 2). The anterior-posterior position was classified as follows, based on a straight line between the anterior nasal spine and posterior nasal spine (bottom of the nasal cavity) as the central axis: impact in the anterior-third of the bottom of the nasal cavity or impact from the anterior nasal spine to the canine was defined as Class A; impact in the middle-third of the bottom of the nasal cavity or impact from the canine to the first molar was defined as Class B; and bone impact in the posterior-third of the bottom of the nasal cavity or impact from the first molar to the posterior nasal spine was defined as Class C (Figure 2).
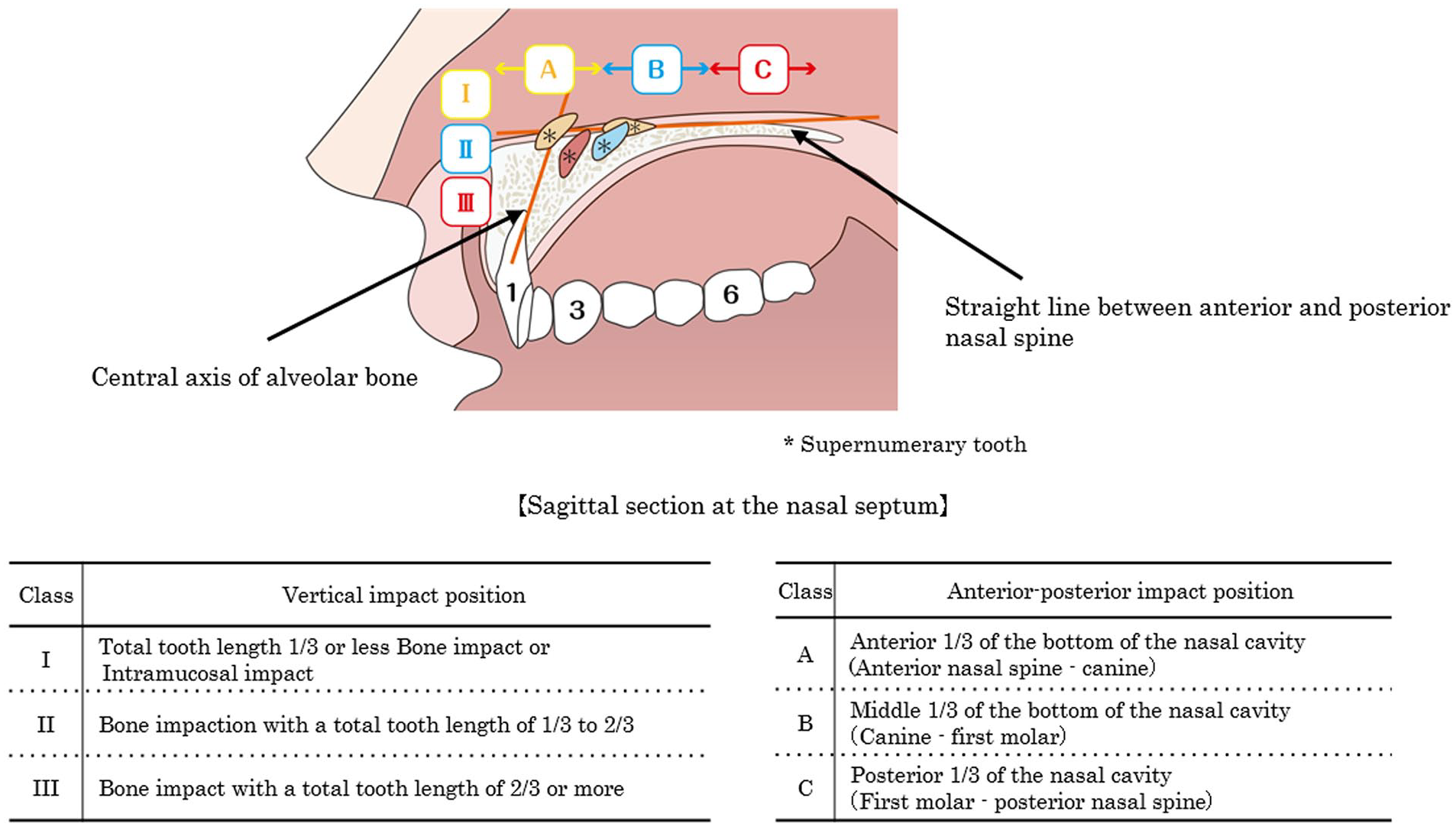
Classification of intranasal supernumerary tooth impaction positions.
Results
Sex and Age
Males outnumbered females (male-to-female ratio of 1.9:1; Table 1). As shown by a median age of 10 years, the majority of patients were young (Table 1). These trends were observed in all decades of the study period.
Cases by Sex and Age in Each Period.
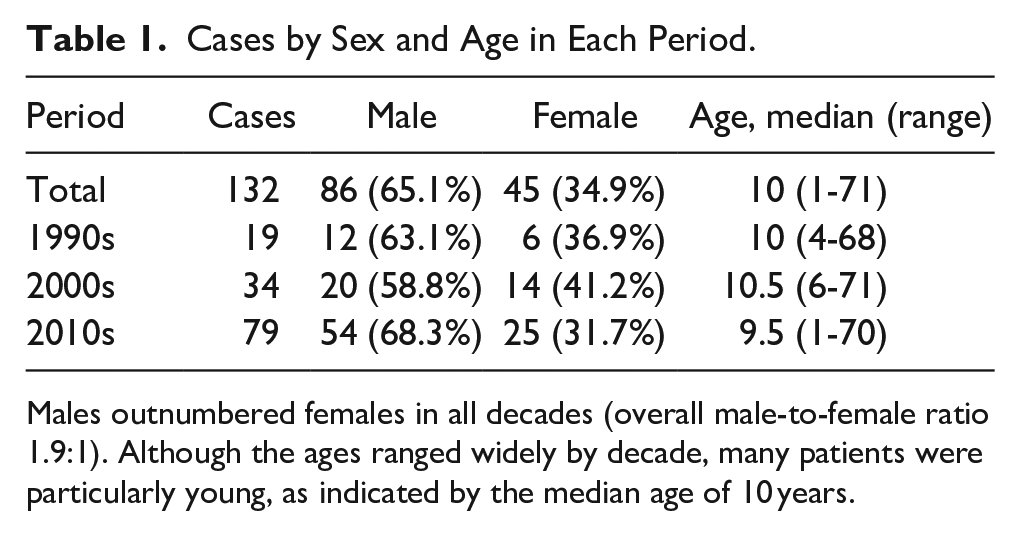
Males outnumbered females in all decades (overall male-to-female ratio 1.9:1). Although the ages ranged widely by decade, many patients were particularly young, as indicated by the median age of 10 years.
Reasons for Consultation
Reasons for consultation consisted of the following: indications observed in diagnostic imaging in 55 cases total; school examinations in 18 cases; discovered by chance in examination for other symptoms, in the absence of nasal symptoms, in 34 cases; and nasal symptoms in 106 cases.
Analysis by decade yielded the following results. In the 1990s, the most common reason for consultation at a healthcare facility was a chief complaint of nasal symptoms, which accounted for 29 of 34 cases (85.3%). From the year 2000 onward, an increasing number of patients underwent consultation due to indications found in diagnostic imaging, despite the absence of symptoms. In the 2010s, the most common reason for consultation was diagnostic imaging indications, which accounted for 46 of 110 cases (41.8%), followed by nasal symptoms, which accounted for 43 of 110 cases (39.1%) (Figure 3). The category of “other symptoms” consisted of cases in which earache, earwax removal, or sore throat prompted consultation at a healthcare facility in which intranasal supernumerary teeth were discovered by chance in a nasal examination; a small number of such cases were observed in each decade.
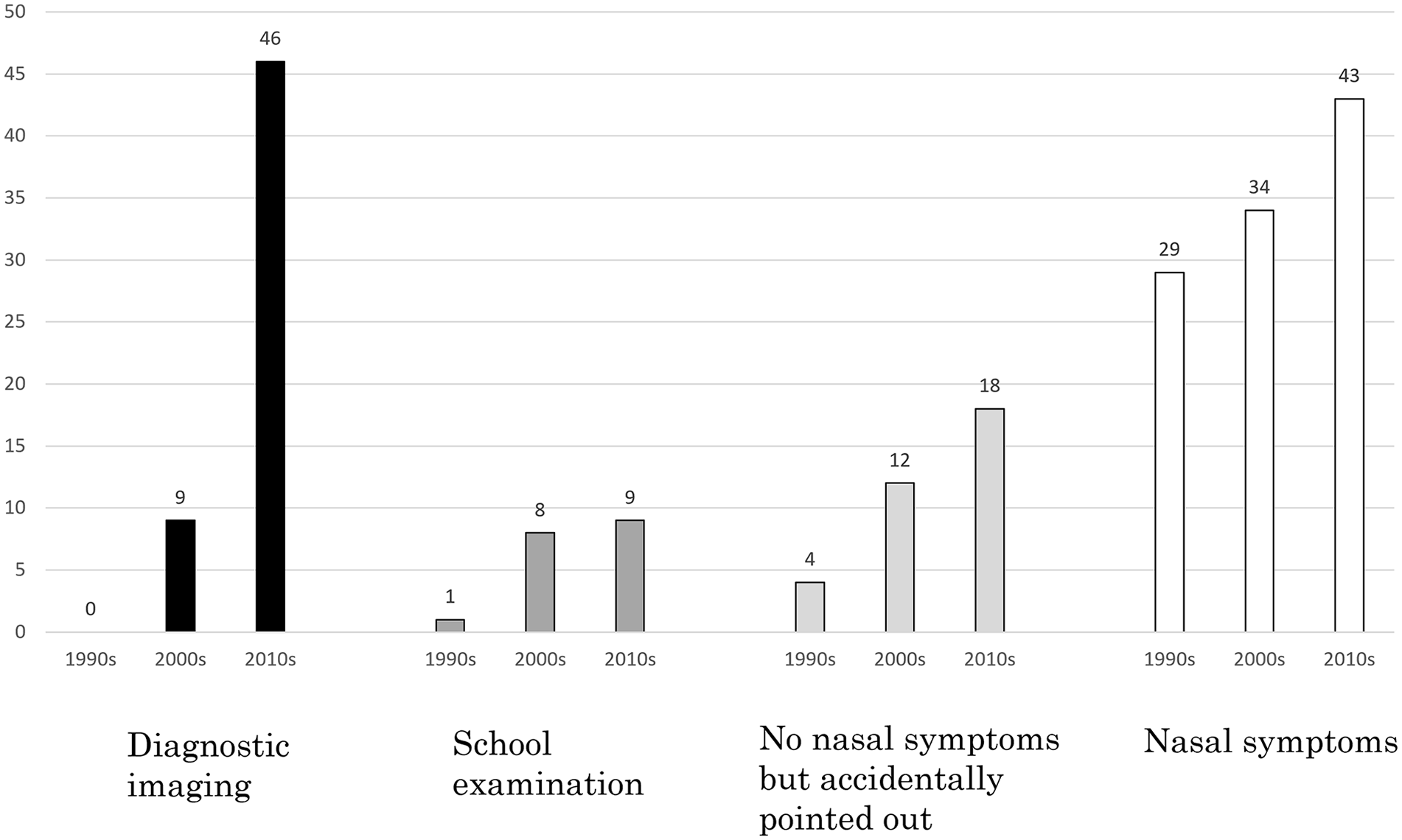
Reason for consultation and change over time.
Reporting Department
The reporting department was the Department of Oral Surgery in 52 cases and Department of Otolaryngology in 80 cases.
Analysis by decade yielded the following results. In the 1990s, 16 of 19 cases (84.2%) were reported by Departments of Otolaryngology. In the 2000s, the percentage of cases reported by Departments of Oral Surgery began to increase (15/34 cases; 44.1%). In the 2010s, 45 of 79 cases (57.0%) were reported by Departments of Otolaryngology, while the remaining 34 cases (43.0%) were reported by Departments of Oral Surgery. The numbers of cases reported from both departments were twice as high in the 2010s as in the 2000s (Figure 4).
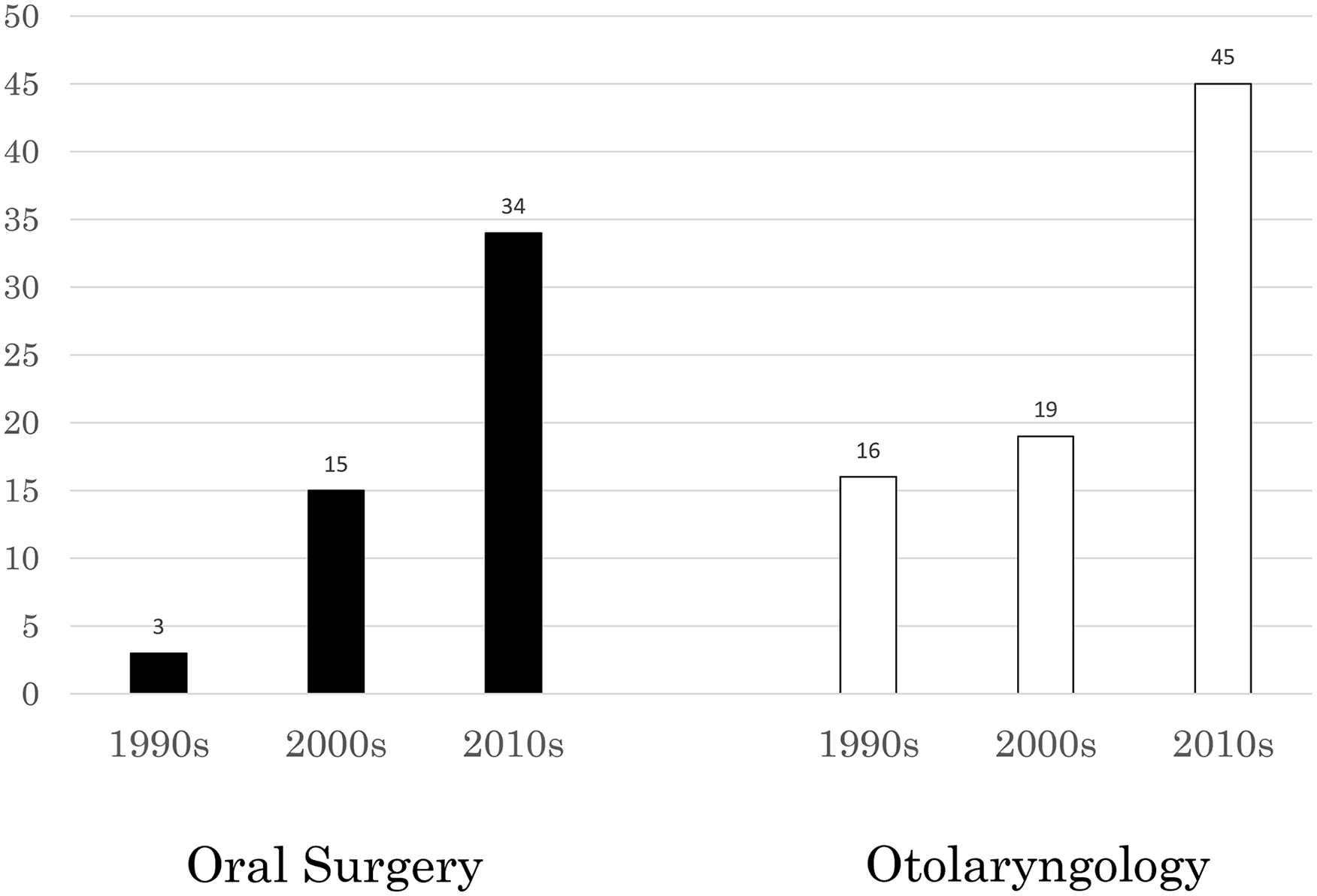
Reporting department.
Impact Positions of Intranasal Supernumerary Teeth
Supernumerary teeth were observed in the left nasal cavity in 69 cases, in the right nasal cavity in 61 cases, and in the nasal septum in 2 cases.
Relationship Between Surgical Approach and Impact Position
The nasal approach was applied when the intranasal supernumerary teeth were classified as IA, IB, IC, IIA, or IIB by an impaction position on the nasal side and with an anterior location. The oral vestibular approach was applied when the teeth were Class IIB, IIIA, or IIIB by impaction position, which are on the oral side and with an anterior location. The palatal approach was applied only when the intranasal supernumerary teeth was Class IIIB, which is on the oral side (Table 2).
Relationship Between Surgical Approach and Impaction Position.
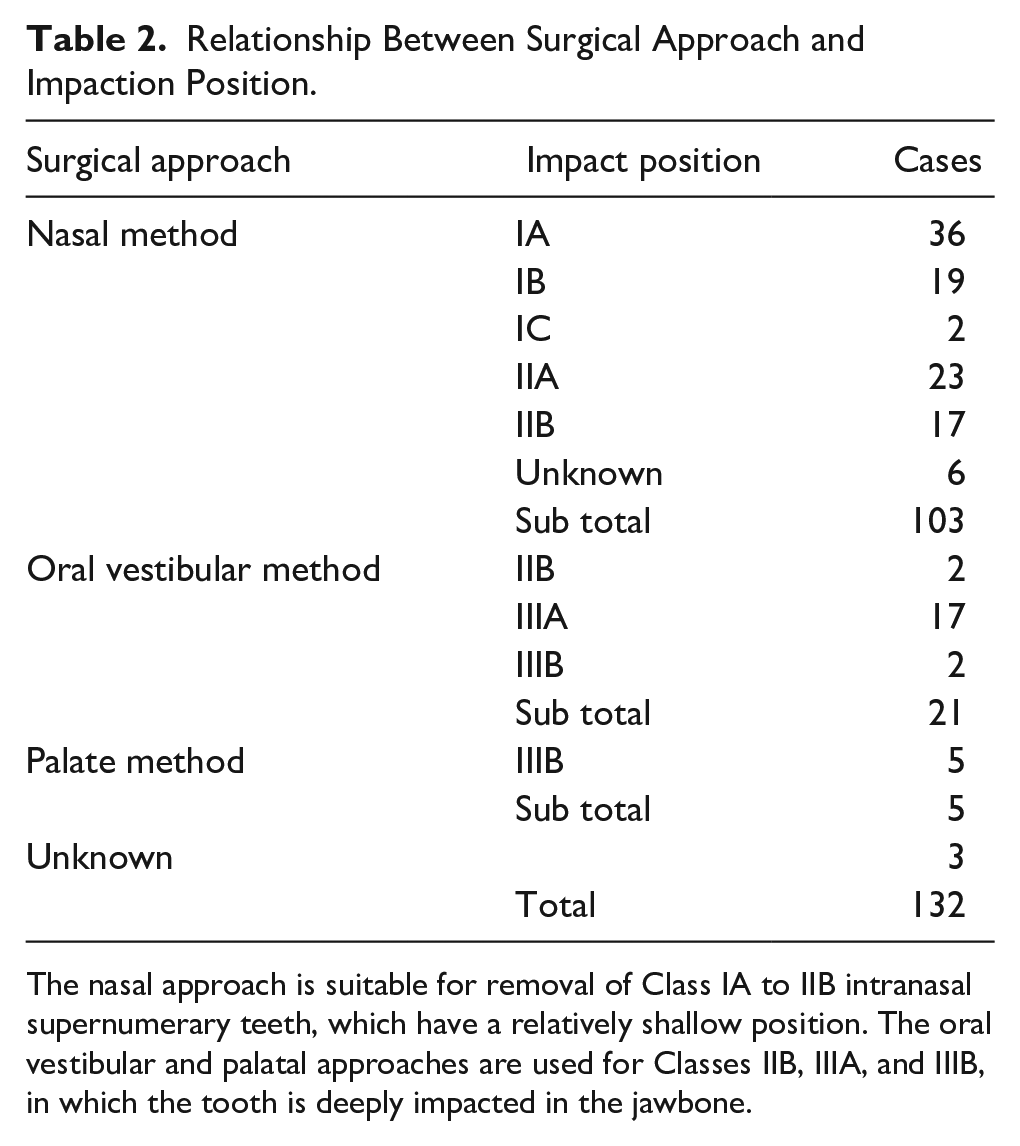
The nasal approach is suitable for removal of Class IA to IIB intranasal supernumerary teeth, which have a relatively shallow position. The oral vestibular and palatal approaches are used for Classes IIB, IIIA, and IIIB, in which the tooth is deeply impacted in the jawbone.
Relationships of Anesthesia with Surgical Approach and Impaction Position
General anesthesia was performed in 97 cases, while local anesthesia was performed in 35 cases. General anesthesia was applied for all surgical approaches and impaction positions.
Local anesthesia was applied only for the nasal approach. Supernumerary tooth removal under local anesthesia was possible in cases of Class IA, IB, and IIA teeth. The 17 cases of Class IIB impaction location in the present study included 4 cases (one of which is reported below), in which local anesthesia was abandoned for general anesthesia due to ineffectiveness (Figures 5 and 6).
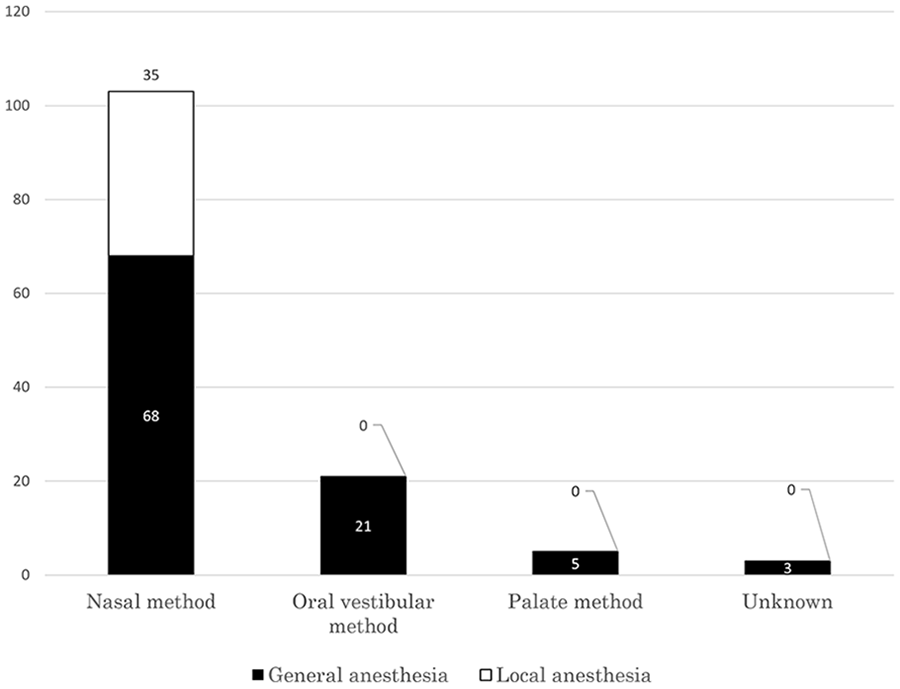
Surgical method by anesthesia.
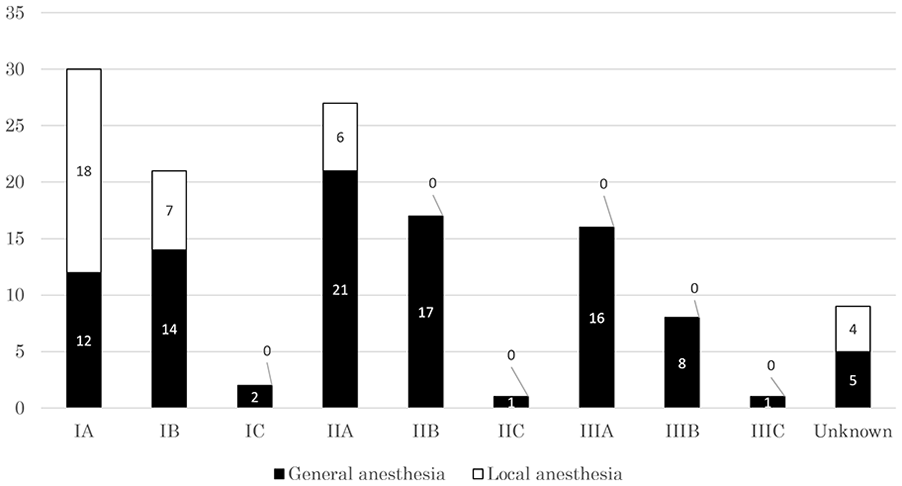
Impact classification by anesthesia.
Case Presentation
Patient: 30-year-old man.
Initial Examination: June 2010.
Chief Complaint: Right nasal cavity discomfort.
Medical History/Regular Medicine/Family History: Unremarkable.
History of Current Illness: Despite having perceived an anterior nasal drip since March 2010, the patient did not seek consultation. In May 2010, right nasal cavity discomfort and intensification of an anterior nasal drip prompted the patient to seek consultation at the Department of Otolaryngology of a nearby hospital. On June 13, endoscopy revealed a tooth-like structure in the right nasal cavity. An attempt to extract the tooth under local anesthesia was abandoned due to intense pain. On June 30, the patient was referred to the Gunma University Hospital Department of Oral and Maxillofacial Surgery for detailed examination.
Present Condition
General Findings: Height 163 cm, body weight 55 kg, medium build. No abnormalities in systemic condition.
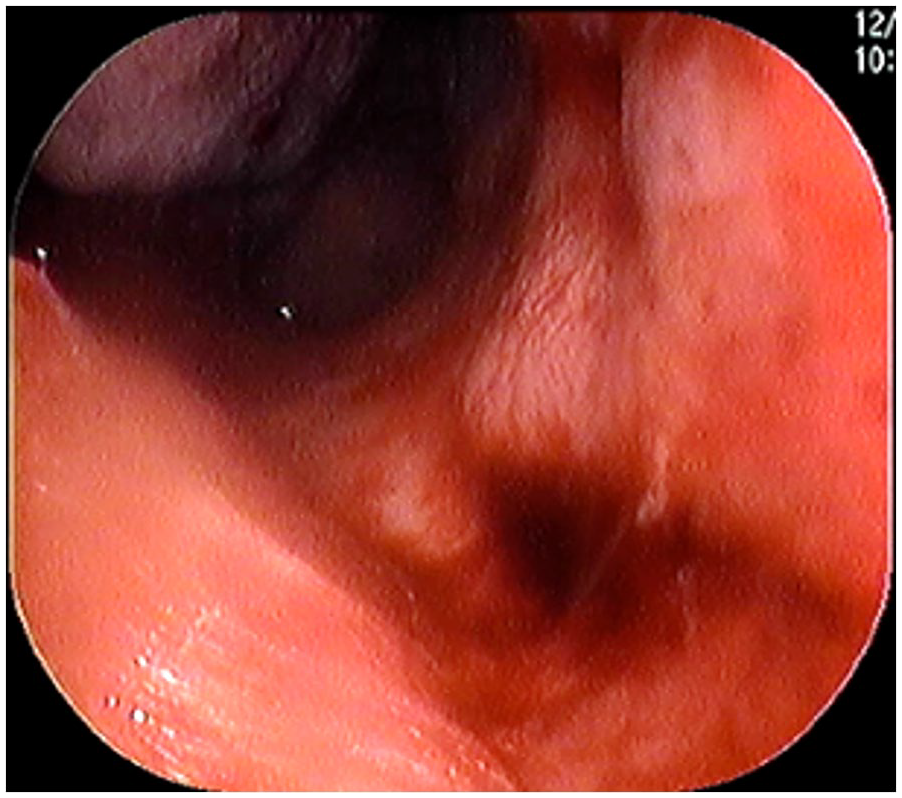
Intranasal Findings: The patient’s face was bilaterally symmetrical. The right nasal cavity demonstrated transparent anterior nasal drip (Figure 7). Additionally, a white tooth-like structure was observed at the bottom of the right nasal cavity (Figure 8).
Facial findings.
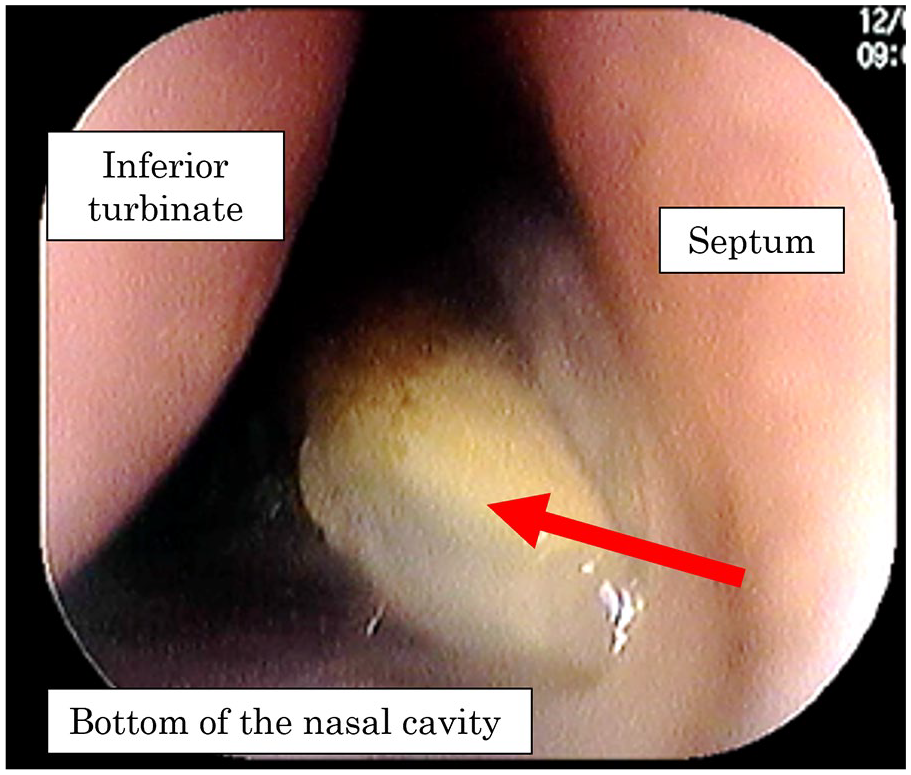
Intranasal findings at initial visit.
Imaging Findings
Computed tomography revealed an inverted impacted supernumerary tooth in the right nasal cavity. The anterior-posterior impaction position was in the middle-third of the bottom of the nasal cavity (from the canine to the first molar); while vertically, more than one-third of the total length of the supernumerary tooth was impacted in the jawbone (Figure 9).
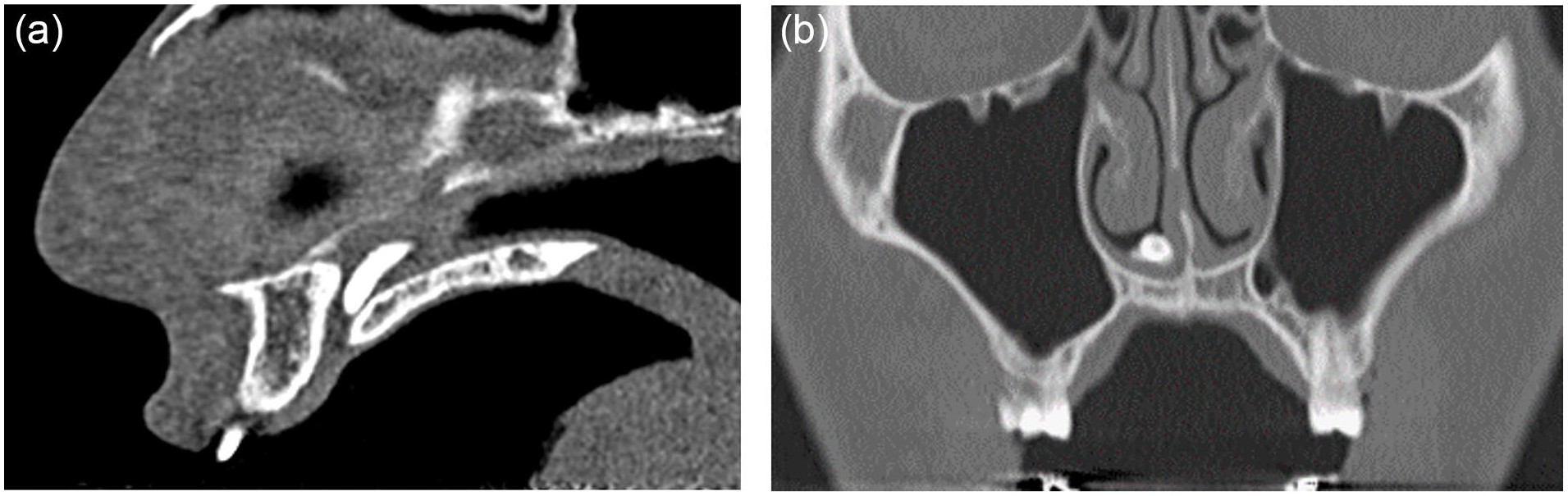
Computed tomography imaging findings. (a) Sagittal section: an inverted impacted supernumerary tooth can be seen near the nasopalatine duct, and (b) Frontal plane: an inverted impacted supernumerary tooth can be seen in the bottom of the right nasal cavity.
Clinical Diagnosis
Right intranasal supernumerary tooth (Class IIB).
Intervention and Course of Treatment
Due to family circumstances, the patient temporarily stopped visiting the hospital. Two years later, he resumed hospital visits. He underwent endoscopic supernumerary tooth extraction under general anesthesia. Prior to removal, we inserted gauze into the right posterior nasal cavity to prepare for tooth dislodgment (Figure 10). The tooth was grasped with forceps and was extracted easily. The patient did not experience epistaxis or any other postoperative complications and was discharged the next day. Anterior nasal drip and discomfort subsequently disappeared, and the patient’s progress has been favorable (Figures 11 and 12).
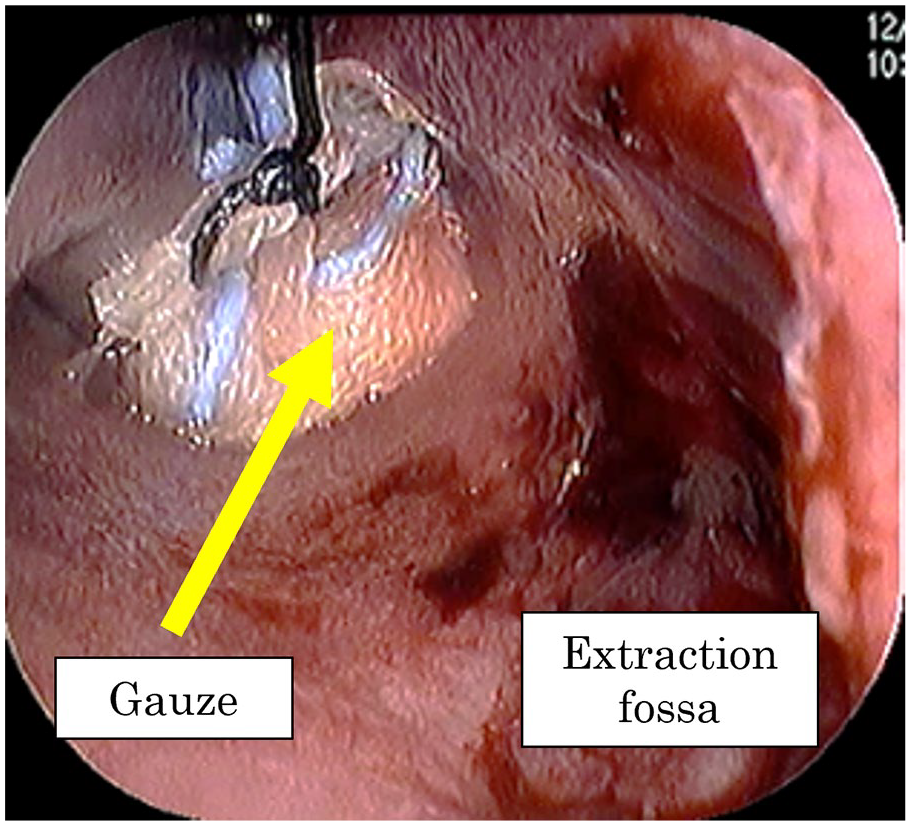
Surgical findings (extraction).

Extracted intranasal supernumerary tooth.
Postoperative intranasal healing.
Discussion
Supernumerary teeth in the central anterior maxilla are considered to occur more frequently in men than in women (men-to-women ratio 1.25-2.5:1).2-7 In addition, while consultations for supernumerary teeth in the central anterior maxilla are considered the most common for patients aged 4 to 9 years, reported patient ages have ranged from young children to older individuals.5-9 In the present study, supernumerary teeth in the nasal cavity possessed similar characteristics to supernumerary teeth in the central anterior maxilla. However, the reason for the more common appearance of both maxillary central supernumerary teeth and intranasal supernumerary teeth in males is unknown.4,10
Our and many other studies have reported that the bilateral difference in intranasal supernumerary teeth is not statistically significant.11,12 Many studies have also reported no bilateral difference in supernumerary teeth in the maxillary anterior region,5,7 suggesting that intranasal supernumerary teeth and maxillary central supernumerary teeth possess similar characteristics.
The above characteristics of maxillary anterior and intranasal supernumerary teeth are consistent, suggesting that intranasal supernumerary teeth are maxillary central supernumerary teeth that have erupted in an inverted fashion and can be considered as a subtype of maxillary central supernumerary teeth.
In the 1990s, patients with intranasal supernumerary teeth, who presented with nasal symptoms, were examined at Departments of Otolaryngology, and thus most reports of supernumerary teeth came from these departments. Presumably, if supernumerary teeth migrated to the nasal cavity, it did not result in bacterial infection or inflammation and therefore did not yield nasal symptoms, patients remained asymptomatic and did not undergo consultation at healthcare facilities; therefore, healthcare facilities had few opportunities to detect intranasal supernumerary teeth in asymptomatic patients.
From the 2000s onward, the number of such reports increased due to the increased opportunities for health screenings, digitalization of X-ray images from 2000 onwards, and early detection of intranasal supernumerary teeth in asymptomatic cases, due to the prevalence of computed tomography.13-20
When subjective nasal symptoms occur or when tests, such as diagnostic imaging, reveal findings of infection, intranasal supernumerary teeth should be extracted before the infection worsens. Additionally, intranasal supernumerary teeth are known to migrate over time. Therefore, even in the absence of subjective symptoms or abnormal imaging findings at a given point in time, migration of supernumerary teeth over time can lead to communication with the nasal cavity and infection by resident nasal bacteria;21,22 thus, follow-up should be performed regularly. In the event that infection findings or other abnormalities are observed during such follow-up, the therapeutic strategy must be changed to extraction (Figure 13).
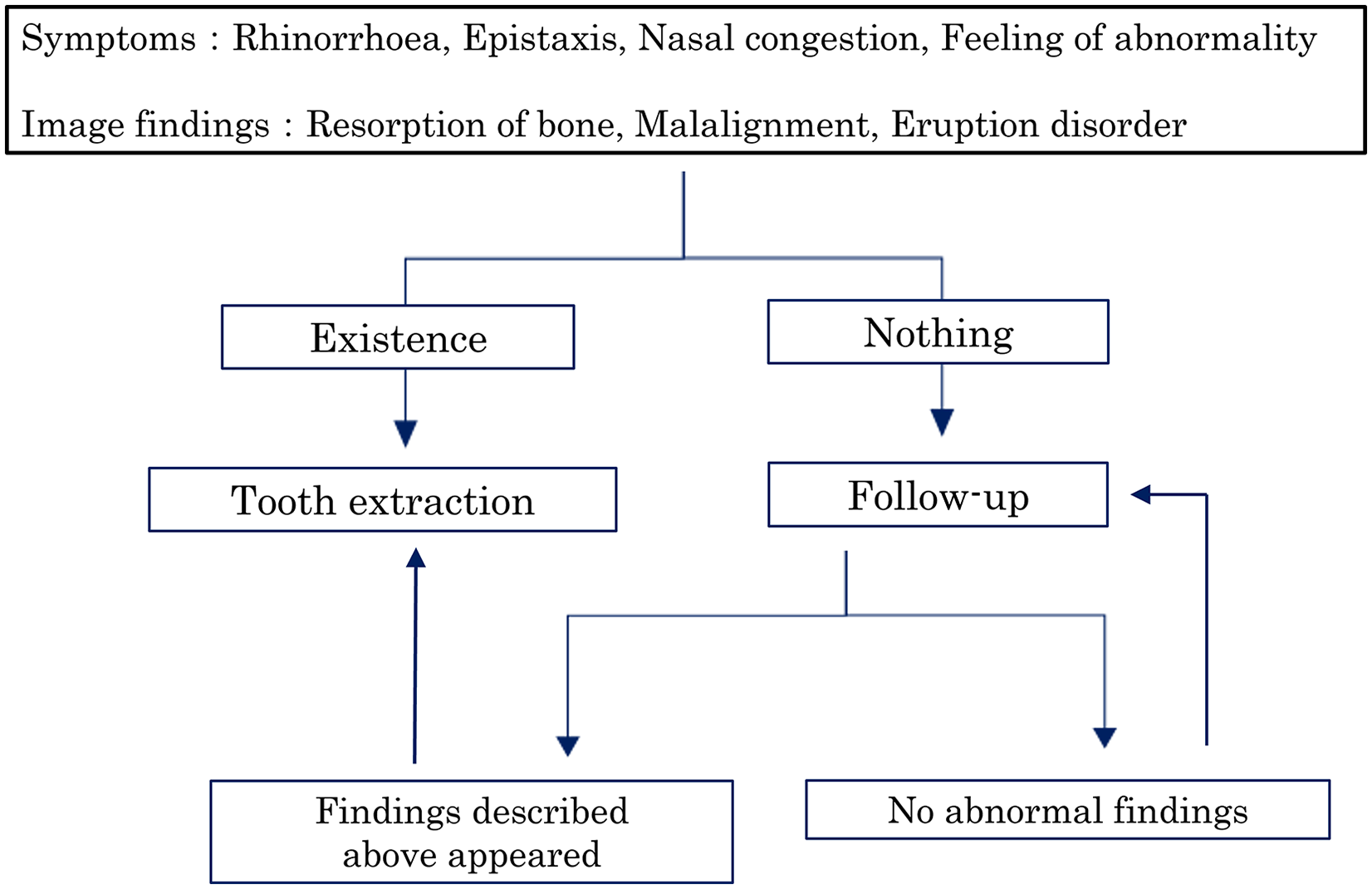
Protocol for intranasal supernumerary teeth treatment.
In the present study, supernumerary teeth could be extracted under local anesthesia only for Classes IA, IB, and IIA as defined by impaction position. In 4 Class IIB cases, including our patient, local anesthesia was ineffective, prompting a change to general anesthesia. Therefore, the criteria for selecting an anesthesia method should be as follows. Under local anesthesia, extraction should be performed only for Classes IA, IB, and IIA, which are on the nasal side and with an anterior location. Under general anesthesia, extraction can be performed at any impaction position. At a depth of IIB or more, general anesthesia should be selected due to the increased surgical invasiveness. For a depth of less than IIB (nasal/anterior side), general anesthesia should be selected when local anesthesia is technically difficult or when the patient experiences anxiety or pain with extraction under local anesthesia.
The criteria for selecting a surgical approach should be as follows. In the present study, Classes IA, IB, IC, and IIA, which are positioned on the nasal side and anteriorly, all extractions were suitably performed with a nasal approach, which was considered appropriate for relatively shallow positions. At greater depths, the visual field is difficult to secure with the nasal approach, making the palatal and oral vestibular approaches preferable. For Class IIB cases in the present study, either the nasal or oral vestibular approach was selected. In this event, since both approaches can be used for extraction, the approach should be decided flexibly based on the surgeon’s judgment and the patient’s condition (Figure 14).
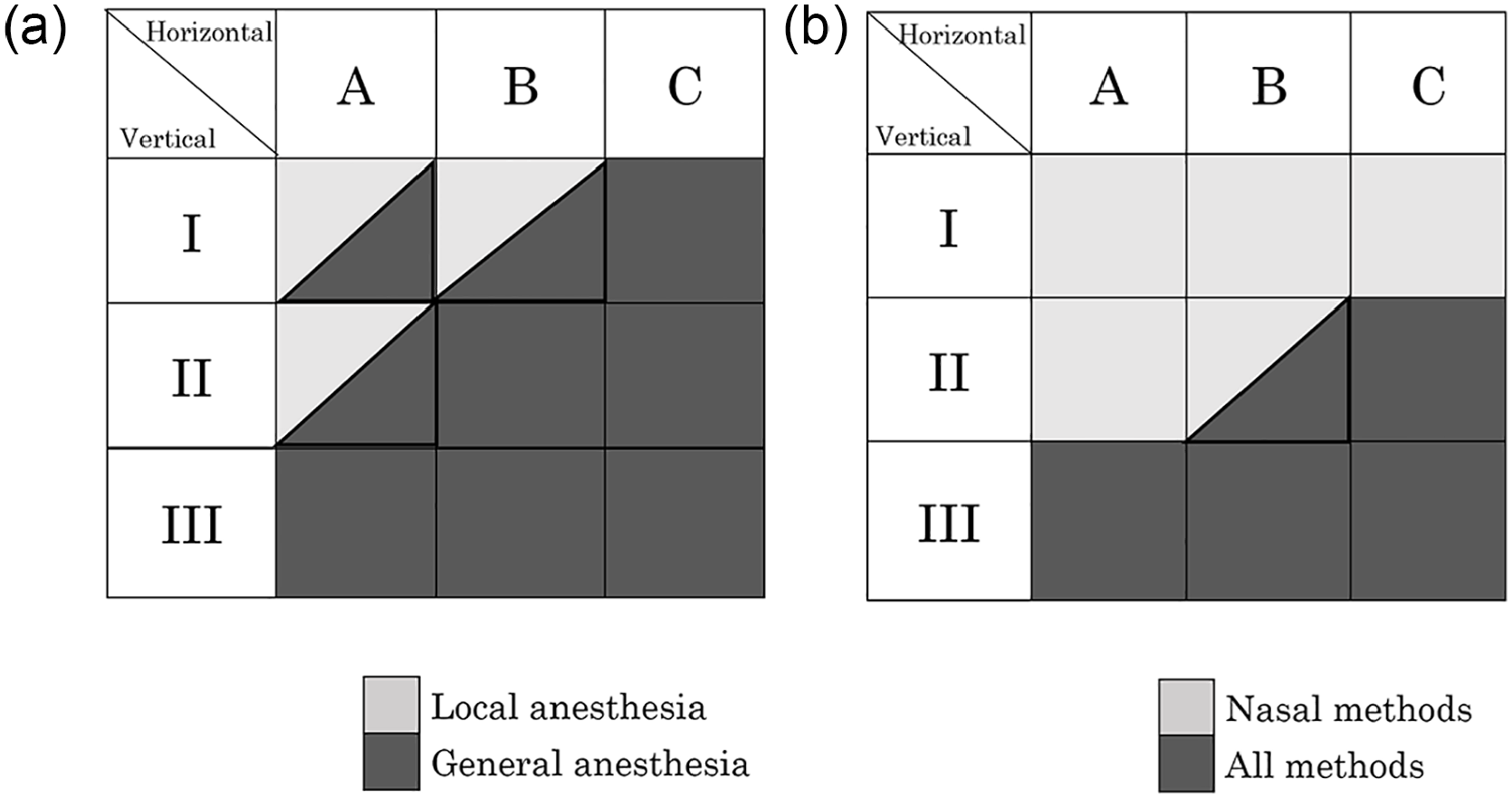
Selection criteria for anesthesia and surgical techniques. (a) Relational diagram of impaction position and anesthesia method. Classes IA, IB, and IIA intranasal supernumerary teeth are positioned relatively shallow, meaning that extraction can be performed under local anesthesia. General anesthesia can be applied for all impaction positions, and (b) Surgical method selection criteria by impaction position. The nasal approach is applicable for extraction of intranasal supernumerary teeth in Classes IA, IB, IC, IIA, and IIB. When the tooth is impacted more deeply in the jawbone, an oral vestibular or palatal approach should be selected.
Based on our comprehensive literature analysis, we classified the vertical and horizontal impaction positions of intranasal supernumerary teeth (Figure 14a and b) to create a protocol for diagnosing and treating these teeth (Figures 13 and 14). This protocol enables accurate understanding of the impaction positions of intranasal supernumerary teeth, the selection of a suitable surgical approach and anesthesia method, and systematic diagnosis and treatment of intranasal supernumerary teeth.
By comprehensively analyzing the literature on intranasal supernumerary teeth, we have created a system for classifying the impaction positions of intranasal supernumerary teeth. This classification system facilitates the systematic diagnosis and treatment of intranasal supernumerary teeth. In conclusion, intranasal supernumerary teeth classification according to their vertical and horizontal impaction positions provides an accurate method for supernumerary tooth impact classification and facilitates the selection of suitable surgical and anesthetic methods, thereby enabling systematic diagnosis and treatment of intranasal supernumerary teeth.
Footnotes
Data Availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the institutional review board of Saitama Yorii Hospital (approval number: Y-211123.03).
Statement of Human and Animal Rights:
All procedures in this study were conducted in accordance with the institutional review board of Saitama Yorii Hospital’s (approval number: Y-211123.03) approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.