
Abstract
Pyogenic granuloma (PG) is a benign fibrovascular proliferative lesion on the skin and mucous membranes, but its pathogenesis remains unclear. PG usually occurs on the head and neck region, fingers and toes. The oral gingiva is the most common location for pregnant patients, while it is rarely found in the nasal cavity. This case is notable not only for its uncommon site and size but also for its gradual growth after delivery. Endoscopic surgery can achieve the desired cosmetic effect and a satisfactory airway. A rapidly growing hemorrhagic lesion in the nasal cavity should be considered as a differential diagnosis.
Introduction
PG is a benign fibrovascular proliferation lesion with an unknown etiology. 1 It commonly occurs on the skin and oral mucosa but rarely in the nasal cavity. 2 PG’s pathogenesis is under discussion, but it has been associated with hormones, local trauma, and immunosuppression. 3 PG most often occurs in the anterior septum, with epistaxis and nasal obstruction as the main symptoms. 1 Most of these lesions are small and involute spontaneously after delivery. 4 Complete surgical excision (with or without pre-operative embolization) is the most effective therapeutic option among others.1,5,6
In this case report, we describe a pregnant woman with a rapidly growing nasal PG, which caused recurrent epistaxis and progressive nasal obstruction. Notably, the tumor did not go away after delivery, but instead continued to grow and even protruded from the nasal cavity. The patient was successfully treated by endoscopic resection. Furthermore, PG patients’ clinical presentation, diagnosis, and treatment are briefly reviewed.
Case report
A 37-year-old female patient was found to have a left nasal tumor 2 months ago with no obvious inducement, but with nasal stuffiness and epistaxis. She had been treated in other hospitals, but no significant improvement was found after nasal spray, even when the tumor grew larger and protrusion was found outside the nasal cavity. The patient sought further diagnosis and treatment at the outpatient department of Lanzhou University Second Hospital. The outpatient department admitted the patient for nasal tumor based on the medical history and specialized physical examination. Notably, the patient was admitted 3 weeks postpartum, and the lesion was discovered during her pregnancy and enlarged quickly, but it did not reduce in size after delivery and even grew larger. She had no other medical history.
Physical examination revealed an irregular-shaped tumor with a dark-brown necrotic surface in the left nasal passage extending about 1.5 cm to the left anterior naris (Figure 1). It was impossible to perform a nasal endoscopy into the left nasal passage due to the tumor completely blocking the left anterior nasal cavity. Clinical photograph showing the lesion obstructing the left anterior nasal cavity and protruding from anterior naris.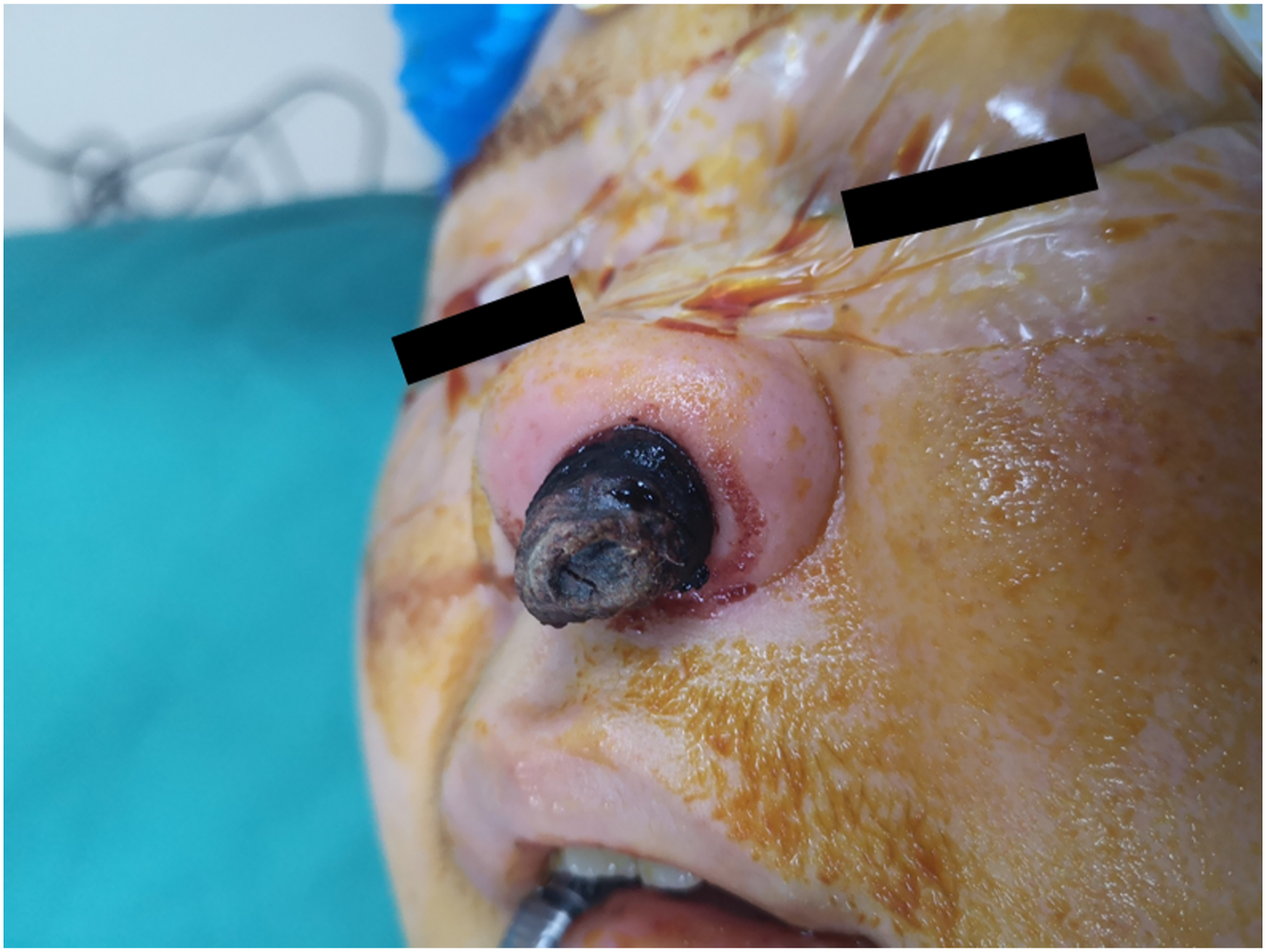
A computed tomographic scan of the paranasal sinuses revealed a leftward deviation of the nasal septum and a focal lesion in the anterior left nasal cavity with encapsulated clear margins measuring 2.7 × 1.8 cm (Figure 2). A benign nature was considered because no evidence of bony erosion or extension to the paranasal sinuses was found. Considering the possibility of severe epistaxis during the operation, a routine pathological biopsy was not performed. Computed tomography axial scan showing a soft tissue density mass in the left nasal cavity.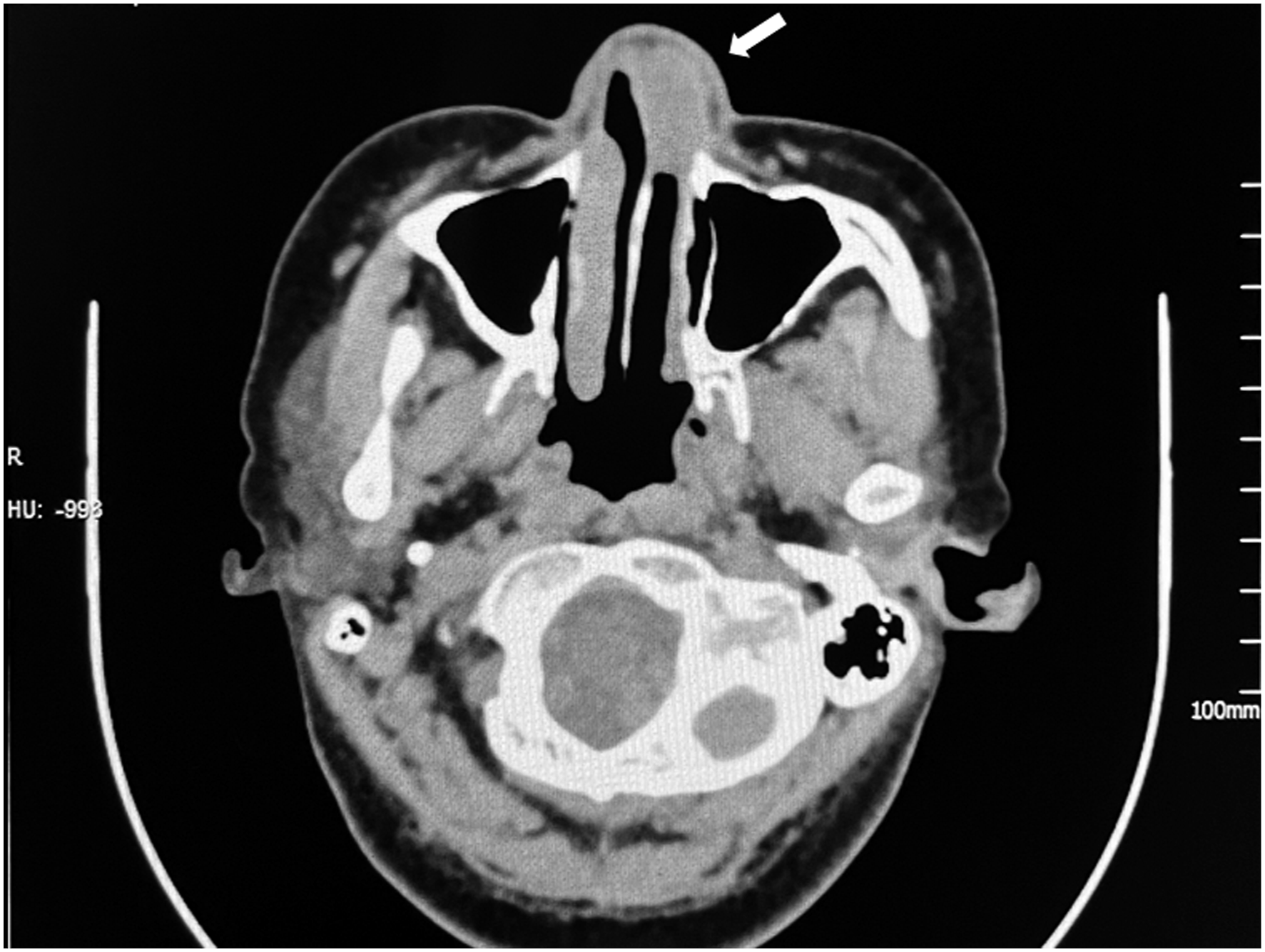
She underwent surgery for the lesion removal and straightening of the nasal septum via an endonasal approach under general anesthesia. Intraoperatively, the tumor was found to originate from the nasal septum. The nasal septum mucosa and perichondrium were resected in a circular way at 3mm around the base of the tumor, and the free edge of the mucosa was repaired. No obvious residue was found. Macroscopically, the excision was about 4.5 × 1.8 cm, partly a dark brown and friable tumor with a smooth surface, and partly a dark and necrotic tumor with a rough surface.
Histopathological examination revealed a benign PG with hemorrhagic necrosis on the surface, a small purulent exudate, and bacterial tumors (Figure 3). The postoperative course was uneventful. The patient was followed up clinically, and no evidence of recurrence transnasal endoscopy was found over the subsequent 6 months. Photomicrograph of the lesion (surgical specimen, hematoxylin and eosin stain, ×100).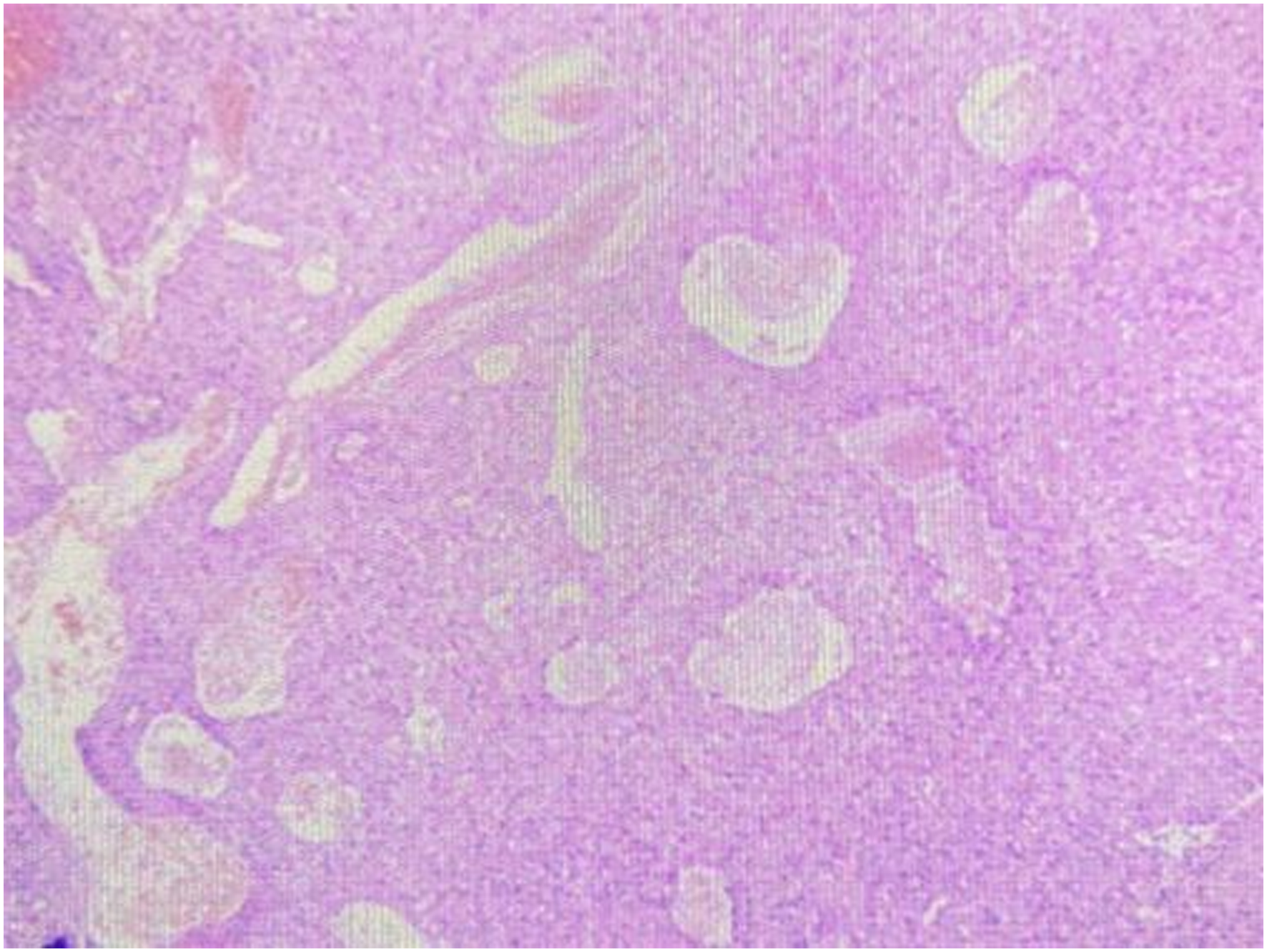
Discussion
The term "PG" was first used to describe individual granulomatous tissue in 1904. However, in 1980, Stacey Mills suggested using the term “lobular capillary hemangioma” to better describe its histological features, noting that PG was a misnomer because the tumor was neither pyogenic nor granulomatous. 1 Both terms are now widely used in various kinds of literature. The term “pregnancy tumor” is more commonly used to describe such lesions when they occur during pregnancy. 7
No underlying etiology for the development of PG has been demonstrated. 1 Hormones: Although previous studies found no significant differences of estrogen and progesterone receptors within lesions between the female and the male, 8 and after 40 years old, the male to female ratio is 1:1, 9 we cannot directly rule out the possibility of hormonal influence in pathogenesis. Because many kinds of literature have reported that female patients have hormonal changes, such as a history of oral contraceptives and pregnancy. 9 PG represents a proliferative vascular lesion; therefore, an imbalance of promoters and inhibitors during the angiogenic process is likely involved. Progesterone regulates the VEGF-A-VEGFR2 signaling, which is a key promoter of angiogenesis. 10 Although the molecular mechanism of lobular capillary hemangioma regression post parturition remains unclear, it has been proposed that it is due to a decrease in circulating estrogen and progesterone and vascular endothelial growth factor levels post parturition;5,6,2 Trauma: These lesions may occur secondary to local trauma, such as nose picking, nasal packing, insect sting, nasal fracture, long-lasting nasal intubation, and nasal surgery including rhinoplasty;3,8,11-13 Drugs: Iatrogenic factors exist, such as the use of epidermal growth factor receptor (EGFR) inhibitors, antiviral drugs, immunosuppressants, and chemotherapeutic agents. 13
PG has a proclivity for the skin and mucous membranes and occurs in all ages. In adults, cutaneous lesions most commonly occur in trunk and extremities, followed by head and neck. In children, however, they appear most frequently in head and neck, followed by trunk and extremities. Subdigital or peridigital PG typically involves the proximal or lateral folds of nails, and sometimes may involve multiple fingers. 13 Mucosal PG occurs most often on the gingival mucosa and also on lips, tongue, buccal mucosa, and palate,1,4,14 but rarely in the epiglottis, esophageal, and gastrointestinal tract.15-17 In pregnancy, the prevalence of PG ranges from 0.5 to 5%, 18 with the majority of cases occurring on the oral mucosa, especially the gingivae.5,19
PG is relatively uncommon in the nasal cavity.4,18 In 3 case series of PG confined to the nasal cavity, lesions were present on the nasal septum in the majority of patients, at 55%, 66.7%, and 76.3%, respectively. In 20%, 12.1%, and 15.8% of cases, lesions were present on the turbinate, with remaining cases on the vestibule, uncinate process, and ethmoid sinus. 8 The lesion in this case also occurred on the nasal septum and even protruded from the nostril. It could be that the area near the nostril is more vulnerable to local trauma. The most common symptoms are easily bleeding and nasal obstruction, but the pain is relatively rare. The lesion is usually visible on an intranasal endoscopic as a gray-to-pink, red or dark, irregular and friable tumor, often with a pedunculated base.5,18,20 Lesions may vary in diameter from a few millimeters to 4 cm during the presentation. 21 In this case, the tumor was large, irregular in shape, and fragile in texture. One part was brown-black polypoid, and the other part was black necrotic. The black and dry part may be related to its exposure to the environment for a long time. These lesions have been reported to resolve spontaneously postpartum, suggesting a role for hormones in the development of PG. The reason why the tumor, in this case, did not resolve and even grew larger after delivery merits further exploration.
On computed tomography (CT), PG appears as a well-defined tumor of soft tissue density, with marked enhancement but no calcification. 22 The magnetic resonance imaging (MRI) features of nasal PG show high heterogenous T2 signal intensity, with a thin peripheral isointense or hypointense ring. 5
There is no denying that imaging plays a crucial role in observing the extent of a nasal tumor and in guiding clinicians in their surgical planning. PG is easily misdiagnosed as a malignant tumor due to its rapid growth. CT, MRI, and nasal endoscopy play an important supporting role in diagnosis and treatment, but the imaging findings are nonspecific. Ultimately, the diagnosis mainly depends on histologic examination. PG is a benign vascular tumor caused by excessive granulation tissue reaction, typically characterized by disorderly capillary growth, inflammatory cell infiltration, and increased stromal deposition. 23
In male adolescents, angiofibroma should be excluded. Kaposi’s sarcoma should be excluded in immunocompromised patients. If a patient has a family history of hereditary hemorrhagic telangiectasia, it should be differentiated from telangiectasia. The differential diagnosis of nasal PG includes other diseases prone to bleeding, such as inverted papilloma, esthesioneuroblastoma, and angiosarcoma.1,8,18
Various therapeutic methods, such as surgical management, laser treatment, or drug therapy, have been used to successfully treat the disease. For nasal PG, treatments such as cautery, laser therapy, embolization, intranasal steroids, and harmonic scalpel are available, though endoscopic surgical resection (with or without pre-operative embolisation) remains a treatment option to reduce recurrence.
Conservative treatment can be attempted when the tumor is small. If the tumor remains after the treatment or does not resolve on its own after delivery and even if it continues to grow, as in this case, it is easy to mistake it a malignant tumor, causing severe psychological pressure to the patient and affecting the appearance of the patient. At this time, nasal endoscopic surgery can be considered. In addition to the conventional nasal endoscopy and CT examination, MRI can be supplemented. Then the operation should be performed as soon as possible after the surgical contraindications are excluded. When encountering a large tumor, pre-operative embolization can be performed to reduce the tumor before surgery. This patient also received surgical treatment. In order to remove the tumor completely, we also removed the nasal septum mucosa and perichondrium in a circular shape at 3 mm around the base of the tumor. She recovered well after the operation with satisfactory nasal ventilation and cosmetic effect.
In order to avoid unnecessary damage to the patients’ mucous membranes, nasal intubation, and nasal packing should be performed as gently as possible and foreign bodies should be removed as soon as possible. Nose picking should be avoided during pregnancy, especially in the third trimester.
Conclusion
PG is a benign lesion that usually occurs on the skin and oral mucosa but rarely in the nasal cavity. The tumor in this case can be easily misdiagnosed as a malignant tumor due to its large size and rare appearance. Rhinologists should include PG in their differential diagnosis when assessing recurrent nasal bleeding lesions, especially in patients with a history of trauma or pregnancy. If the lesion does not regress spontaneously after delivery, surgical removal with or without pre-operative embolisation is the accepted therapy. Further research is needed to prove the causal relationship between pregnancy and PG.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received specific grant from National Natural Science Foundation of China (grant number: 82160214).
Data availability statement
All data generated or analyzed during this study are included in this article.
Ethical approval
The study was approved by the institutional review board of Lanzhou University Second Hospital. The patient provided written informed consent.