
Abstract
Aim of this manuscript is to propose a clear and easily applicable classification for turbinate surgery, based on the use of a numerical model, which could be introduced in the practice of Otolaryngologists and Maxillo-Facial surgeons.Applying this classification, it will be possible to offer an easy format when describing which turbinates are involved in a procedure, and to offer a quick method to record and analyse clinical data, also for scientific purpose.
We would like to propose a clear and easily applicable numerical classification that could be introduced in the practice of Otolaryngologists and Maxillo-Facial surgeons, for indicating which turbinate is involved in a procedure. To the best of our knowledge, no specific and similar classifications are available in the literature, so far.
Anatomically, turbinates are mainly 3, rarely 4, and are located in the lateral wall of each nasal cavity. The inferior turbinate is composed of conchal bone, while the middle and superior are part of the ethmoidal bone (sometimes is possible to find a supreme turbinate, still part of the ethmoidal bone). Pneumatization and paradox curvature of the middle turbinate represent the most frequent abnormalities in the anterior ethmoid region, often causing dysventilation of osteomeatal complex. The pneumatization of the middle turbinate is described to have several grades of extension; this can involve the vertical lamella (lamellar cell), the inferior bulbous portion of the middle turbinate (bulbous) or both parts extensively (concha bullosa). 1
The surgery of middle and inferior turbinates is often performed during the sinonasal surgery, alone or in association with septoplasty or other nasal procedures, such as functional endoscopic sinus surgery. Inferior turbinate hypertrophy represents, in fact, the most common cause of nasal obstruction, often associated to septal deflection and/or to chronic hyperplastic rhinitis, with or without polyps. 1 The role of turbinate surgery is commonly recognised in the literature. Several studies demonstrated that the association between turbinate surgery and septoplasty can offer a better postoperative result in terms of nasal breathing flow. 1
In the literature, other classification proposals of turbinates surgery are available; however, these (1) mainly involves inferior turbinates only, and (2) mainly focus on their pre- and postoperative size.2,3
Other sinonasal classifications available focus on nasal anatomical and radiological variations; in particular, Stammberger and colleagues established universally recognized landmarks for all rhinology surgeons.4,5
The present proposal is based on the use of a numerical model and aims to indicate which turbinates are involved (or have been involved in the past) in a procedure. The inferior turbinates are respectively named 1 on the right side, and 2 on the left, while the right middle turbinate is the number 3, and the left middle turbinate the number 4 (if eventually involved, right superior turbinate will be number 5 and left superior turbinate number 6). Therefore, odd numbers refer to the right side and even to the left (see also Figure 1A). In this way, for example, when surgery only involves the inferior turbinates, the procedure could be named as a “turbinoplasty 1.2” for example (Figure 1B). In case of a left septal deflection with a right inferior turbinate hypertrophy and a right concha bullosa, the surgeon could perform a “septoplasty with inferior and middle turbinates resection” (therefore named as “septoplasty with 1.3 resection”; Figure 1C). Finally, in case of a septal deflection with bilateral concha bullosa, one could perform a septoplasty with a middle turbinates resection (then easily named “septoplasty with 3.4 resection”; Figure 1D). This method could provide a useful standard for the preoperative planning and for postoperative report. Surgical reports could be detailed and fast writing, offering a clear tool for all Otolaryngologists and also Maxillo-Facial surgeons, especially in case of previous surgery.
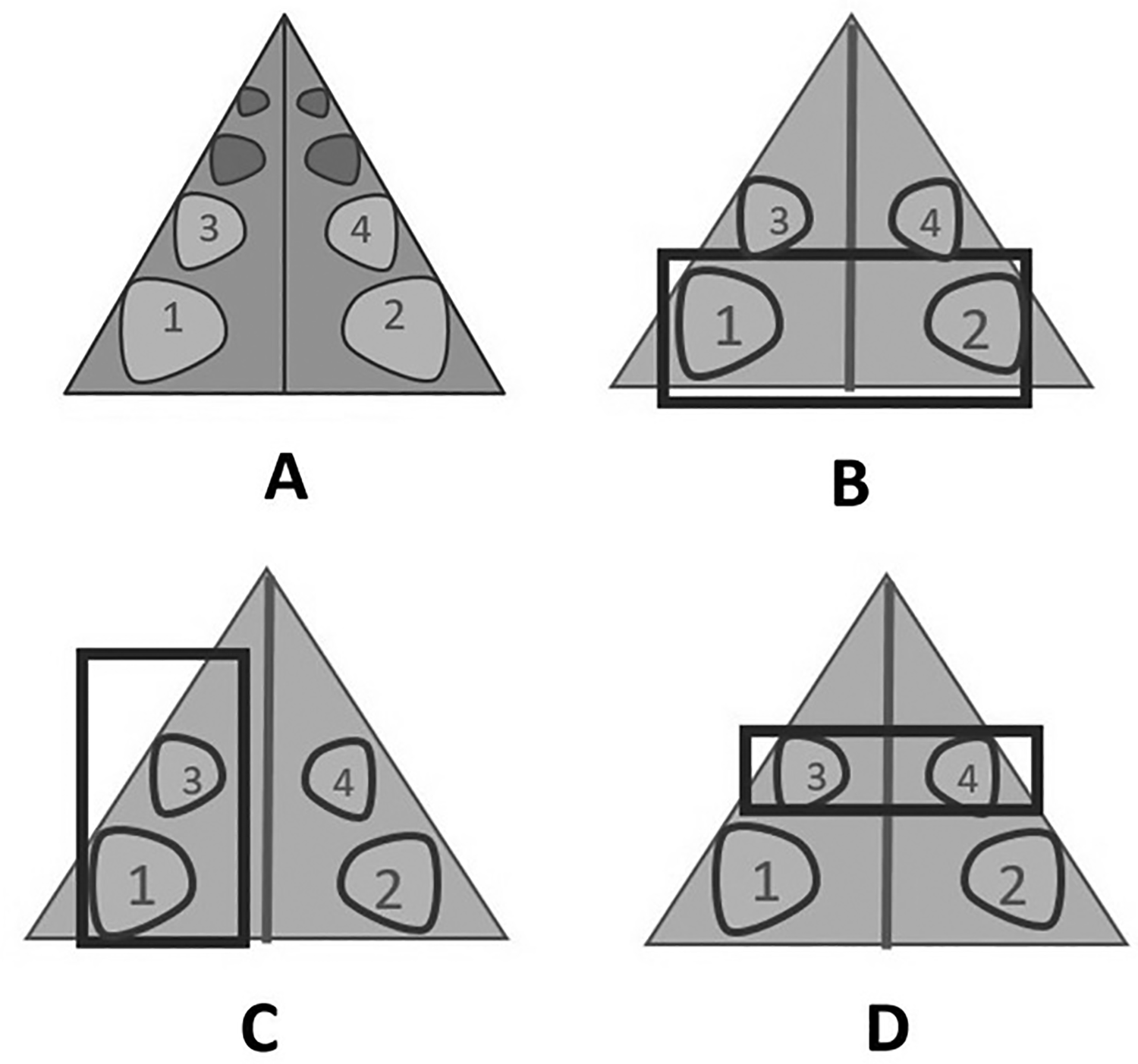
A, TUrbinate Surgery Classification (TUSC) schematic representation; (B) inferior (1.2) turbinoplasty; (C) inferior right (1.3) turbinoplasty; (D) middle turbinates (3.4) resection.
In conclusion, applying the proposed classification, it will be possible to (1) offer an easy format when describing which turbinates are involved in a procedure and (2) offer a quick method to record and analyze clinical data, also for scientific purpose.