
Abstract
Inflammatory pseudotumor (IP) is a clinically aggressive but histologically benign condition of unknown cause. It rarely appears in the nasal cavity and sinuses. Here, we describe a 24-year-old female with the main symptom of right nasal obstruction. Examinations showed dilation in the right maxillary sinus and a pale neoplasm in the nasal cavity. The neoplasm was completely excised under endoscope. Postoperative pathology showed significant proliferation of plasma cells and lymphocytes, indicating the presence of IP. No recurrence was found during 20 months of follow-up. Only 28 cases (10 males and 18 females, average 41.04 years) have been reported on Pubmed. The main clinical manifestations were nasal obstruction, epistaxis, facial swelling and pain, eyeball protrusion, diplopia, and other ocular symptoms. Inflammatory pseudotumor always erodes the surrounding bone and requires active treatments. Surgery is the optimal option with a good prognosis.
Introduction
Inflammatory pseudotumor (IP) is a clinically invasive but histologically benign mass of unknown etiology. Composing a large number of plasma cells, lymphocytes, fiber cells, histocytes, and eosinophils. Inflammatory pseudotumor is variously termed, such as plasma cell granuloma, inflammatory myofibroblastic tumor, histiocytoma complex, fibrous xanthoma, inflammatory myofibrohistiocytic proliferation, and so on. 1 Inflammatory pseudotumor commonly arises in the lung but may involve any organ. Inflammatory pseudotumor in head and neck accounts for less than 5%, mostly found in the orbit. 1
Inflammatory pseudotumor in the nasal cavity and sinus is very rare but highly recurrent and harmful. It is easy to be ignored or misdiagnosed due to the lack of typical clinical manifestations. Routine pathological tests often show the abnormal proliferation of plasma cells, lymphocytes, and other inflammatory cells. Few cases have been reported.2-20 Here, we present a case of IP in the maxillary sinus, and its clinical features were summarized through literature review.
Case Report
In March 2018, a healthy 24-year-old woman presented at our hospital with right nasal obstruction for over 1 year. No epistaxis, nasal pain, runny nose, and other discomfort were felt at onset, so the patient took no immediate treatments. Two months before the visit, her nasal obstruction worsened, accompanied by anosmia. Nasopharyngoscopy showed that the right nasal cavity was fully occupied by a large gray–white neoplasm with a smooth surface. The inferior turbinate was compressed, and the septum was deviated to the left. There was no obvious abnormality in the left nasal cavity. Computed tomography (Figure 1) showed that a soft tissue mass had expanded into the right maxillary sinus, destroyed the medial wall, involved the nasal cavity, and compressed the septum to the left. The bone window showed thinning of the posterior lateral wall of the maxillary sinus, suggestive of the origin of the lesion. Magnetic resonance imaging (MRI; Figure 2) showed the low signal intensity on T1-weighted image, inhomogeneous hyperintensity on T2-weighted image, and marked inhomogeneous enhancement on contrast-enhanced T1-weighted image. Preoperative routine examinations showed no special results. Endoscopic surgery was performed. Intraoperatively, we found the right nasal cavity was blocked by necrotic and gelatinous neoplasm, which expanded from the posterior lateral wall of the maxillary sinus. The medial wall of the maxillary sinus was partially destroyed. After removal of the neoplasm, the substrate of neoplasm was ablated by low temperature plasma. Next, after we opened sieve soaks and forehead recess, purulent exudate overflowed. Postoperative histopathology revealed a mixture of lymphocytes and plasma cells and significant proliferation of mucus glands and infiltration of mucus in the mass (Figure 3). Immunohistochemical staining showed positive CD138, CD3, CD20, κ, λ, and epithelial membrane antigen(EMA) but negative Des and S100.
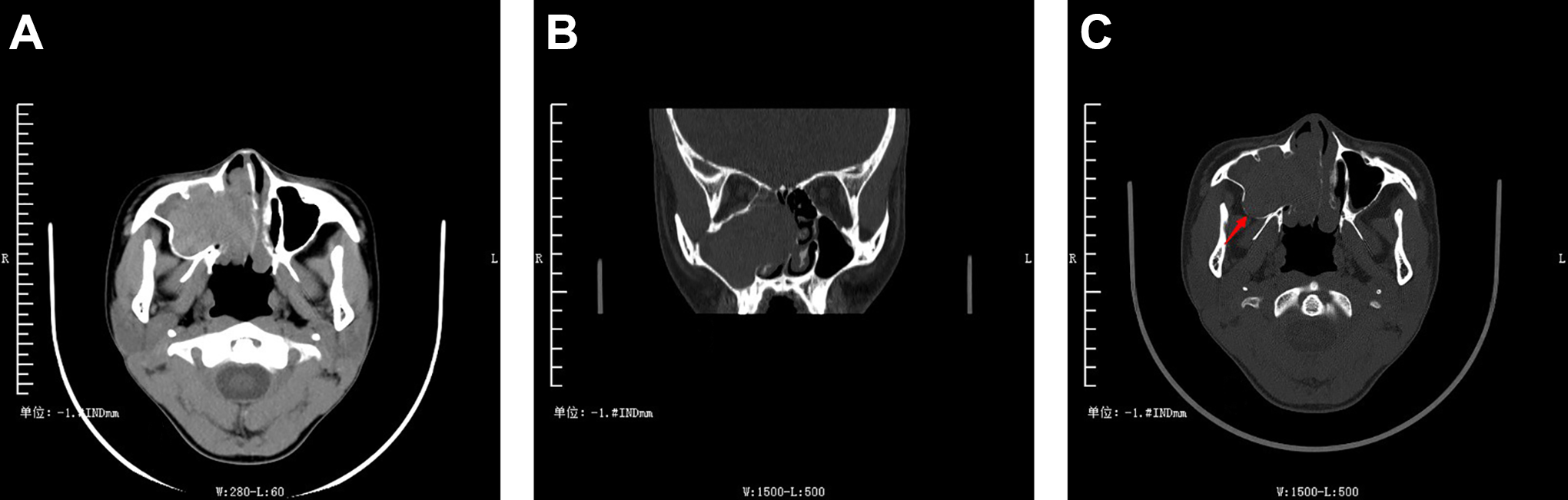
Computed tomography (CT) scan shows soft tissue mass with expansive growth in the right maxillary sinus which destroys the medial wall and grows into the nasal cavity and compressed the septum to the left (A and B). The bone window shows thinning of the posterior lateral wall of the maxillary sinus (↑), suggesting that the lesion originates there (C).
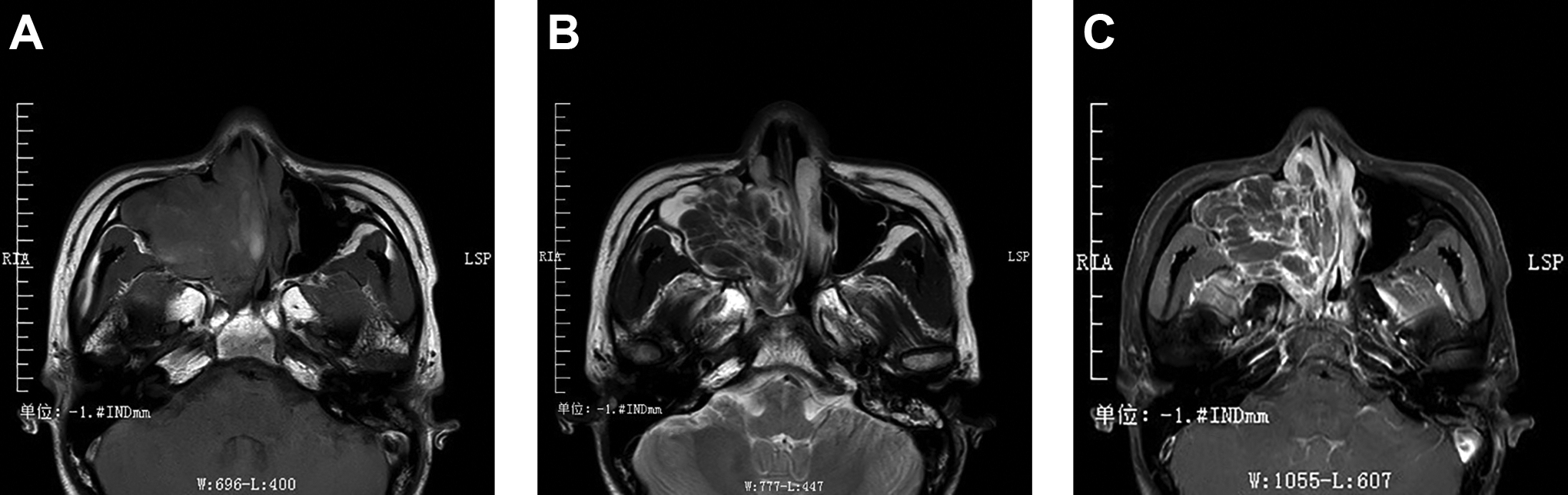
The right maxillary sinus tumor shows mild low signal intensity on T1-weighted image (A) and inhomogeneous hyperintensity on T2-weighted image (B). Marked inhomogeneous enhancement on contrast-enhanced T1-weighted image (C).
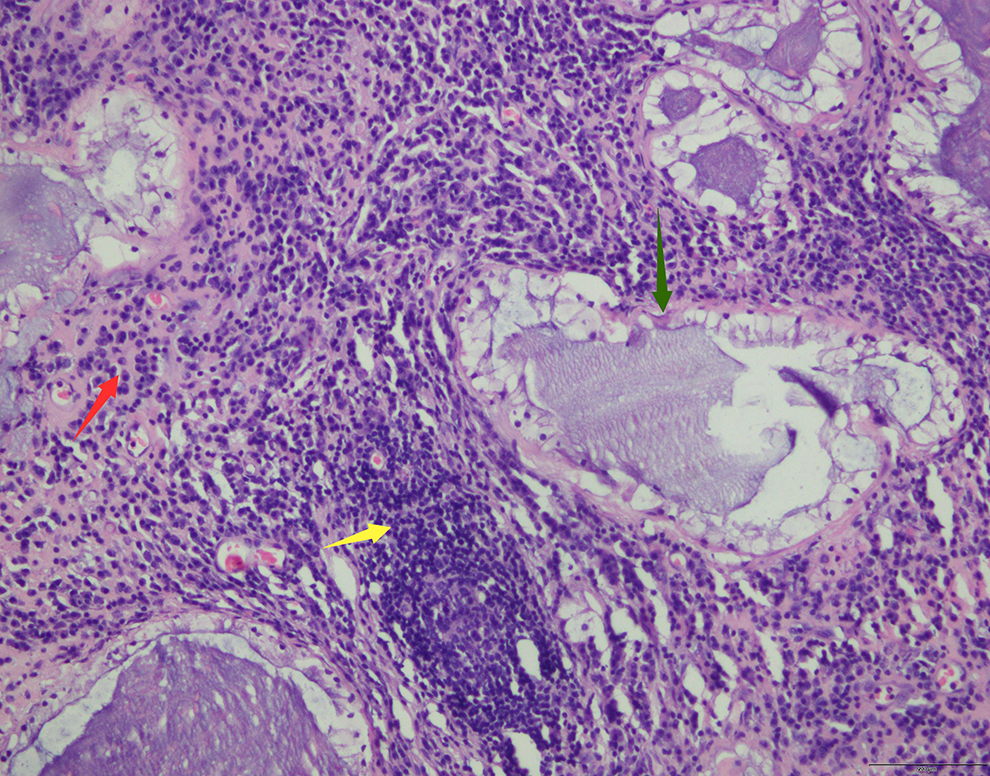
The tumor composed of a mixture of lymphocytes (yellow↑) and plasma cells (red↑) and significant proliferation of mucus glands (green↑). ×200.
This tumor’s growth pattern, imaging manifestations, pathology, and immunohistochemistry were not reported previously, making us difficult to establish a diagnosis, but its malignance could be denied. The patient was instructed to retake nasal endoscopy regularly, and the nasal mucosa was well epithelialized, without tumor recurrence at 3 months after surgery (Figure 4). Accidentally, a physician introduced a case with IP in the temporal bone. We discovered that our patient’s pathology and immunohistochemistry results were indicative of IP. It took more than 3 months for us to confirm it as an IP in the nasal cavity and sinus. Up to now, no evidence of recurrence has been observed (negative MRI at 18 months).

Postoperative examination. Nasal endoscopy was reviewed 3 months after operation showed that nasal mucosa was epithelialized well without tumor recurrence.
Literature Review
We searched the literatures published in the PubMed before 2019.12 using entries “IP/plasma cell granuloma/inflammatory myofibroblastic tumor” and “nose/nasal cavity/paranasal sinus.” Only 19 associated literatures and 28 cases (10 males and 18 females, average age 41.04 years, range 10-75 years) were identified (Table 1).2-20 The main clinical manifestations are nasal congestion (13/28), epistaxis (10/28), facial discomfort or facial swelling and pain (9/28), and ocular symptoms (7/28). The nasal cavity displayed tumor involvement in one side in 26 cases (10 left side, 16 right side) and both sides in the other 2 cases. Maxillary sinus is the most affected site (12/28), followed by nasal cavity, ethmoid sinus, and sphenoid sinus. Bone destruction occurred in 17 cases, invasion of subtemporal fossa in 6 cases, anterior skull base in 2 cases, slope and cavernous sinus in 1 case.
Inflammatory Pseudotumors Located in the Nasal Cavity and Sinuses Reported in the Literature on Pubmed.
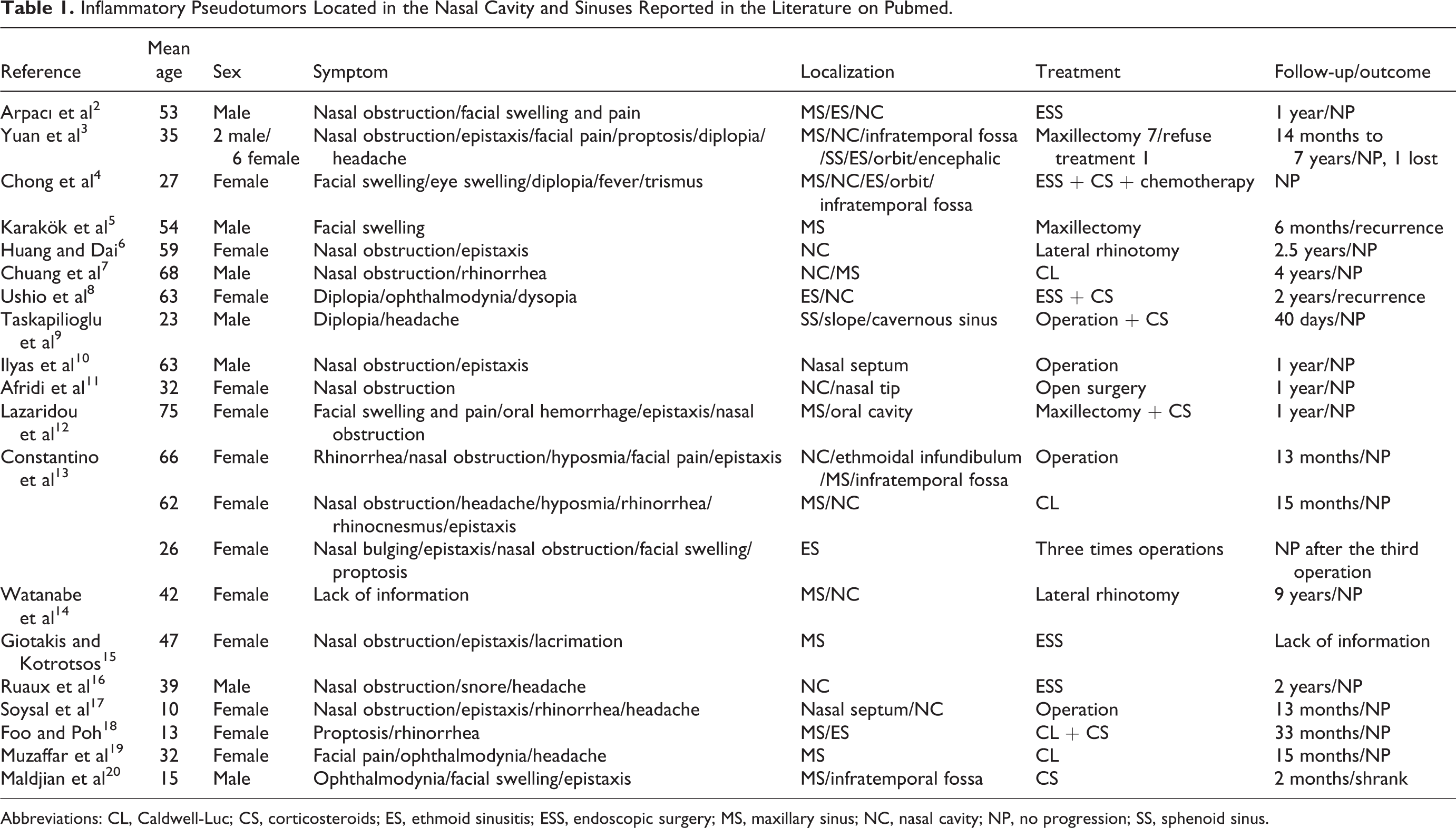
Abbreviations: CL, Caldwell-Luc; CS, corticosteroids; ES, ethmoid sinusitis; ESS, endoscopic surgery; MS, maxillary sinus; NC, nasal cavity; NP, no progression; SS, sphenoid sinus.
Surgery is usually considered as the first-line treatment. Twenty-six patients underwent surgical treatment. Caldwell-Luc operation and lateral rhinotomy were formerly chosen, but endonasal endoscopic surgery has become popular in recent years. One case was only treated with oral corticosteroid therapy, and the tumor shrank after 2 months. 20 Among the 26 surgery-treated patients, 21 were treated by operation alone. Two patients had recurrence, but no progression after the latest operation.5,13 The remaining 17 patients had no recurrence during the follow-up. The tumor relapsed in one patient 2 years after surgery and became smaller after corticosteroid therapy. 8 Three patients were given adjuvant oral corticosteroid after operation and no recurrence was found.9,12,18 One case was assisted with both oral corticosteroid and chemotherapy after surgery and no recurrence was found. 4
Discussion
Inflammatory pseudotumor may be seen in both sexes, at all ages, and in any part of the body (mostly in the lung). Orbit is the most likely involved site in the head and neck region. 1 Similar to malignant tumors, IP can damage the surrounding bone and invade adjacent organs.1,4 The pathogenesis of IP is still obscure, which may be related to immunity, acute infection response, and postinflammatory reparative process.21,22 Studies have found that about 50% of patients with IP have a rearrangement of anaplastic lymphoma kinase genes located on chromosome 2p23. 23 In this review, one patient with a history of nasal drug abuse demonstrated mycobacterium avium infection. 10
Inflammatory pseudotumor in the nasal cavity and sinus demonstrate symptoms as the mass dilates to block the nasal cavity or press the surrounding tissue structures, usually without fever, emaciation, and other systemic symptoms. Some may be accompanied by enlarged lymph nodes in the neck, but it will not develop into lymphoma as orbital IP does. 20 Rhinoscopy reveals a pale or red-bluish substantial mass in the nasal cavity. The images show swelling of the soft tissue mass with bone destruction or infiltration into adjacent tissues, and mild to moderate enhancement appears after the injection of contrast medium. 3 The pathology of IP is mainly characterized with spindle cells, lymphocytes, and plasma cells, which are sometimes mixed with extracellular collagens, fibroblasts, neutrophils, and other inflammatory cells. The present case also exhibited abundant mucus glands which may lead to a gelatinous mass. Probability of plasma cell tumors was excluded by immunohistochemical examination. In immunohistochemical staining, IP is usually positive for vimentin, EMA, CD138, CD20, CD68, and negative for S100.
Treatments for IP in the nasal cavity and sinuses depend on tumor location, biological behavior, and the general condition of the patient, mainly including surgical resection, oral glucocorticoid, chemotherapy, or combined treatments. Adjuvant radiotherapy can be tried, especially for those with contraindications for surgery and glucocorticoids or local recurrence. 16 In general, surgery is effective, and glucocorticoids or chemotherapy can be used as adjuvants. Corticosteroid therapy can significantly shrink the tumor size, but there are no follow-up data to confirm this efficacy.8,20 In addition, the course and dosage of corticosteroid therapy are unclear. It has been reported that IP in the nasal cavity and sinuses are less sensitive to glucocorticoids than orbit IP. 16 In our review, only one case was treated with postoperative adjuvant chemotherapy using oral corticosteroids. Therefore, no conclusion could be drawn on the efficacy of chemotherapy.
Conclusion
Inflammatory pseudotumor in the nasal cavity and sinuses is rare. It has no distinctive characteristics and is often diagnosed on the basis of medical history, rhinoscopy, imaging examination, and immunohistochemistry. Inflammatory pseudotumor always erodes the surrounding bone and requires active treatment. Surgery is the main option with a good prognosis.
Footnotes
Authors’ Note
J.L. the first author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.