
Abstract
Background
This case highlights the eerie nature of rhinorrhea in a small child, which can be easily overlooked or attributed to common causes such as allergic rhinitis and upper respiratory infections. However, in rare instances, it can be a manifestation of a spontaneous cerebrospinal fluid (CSF) leak, leading to potentially severe consequences such as bacterial meningitis. Understanding the importance of timely diagnosis and appropriate surgical intervention is crucial in preventing long-term complications and ensuring the well-being of children affected by spontaneous CSF rhinorrhea. Spontaneous CSF rhinorrhea is uncommon in the pediatric population, but can lead to significant morbidity and mortality if left untreated. Proposed mechanisms include the presence of a congenital skull base defect 1 and increased intracranial pressure or hypertension. This work demonstrates endoscopic uninarial repair of a pediatric spontaneous CSF leak in a 2-year-old patient.
Case
This patient was a 2-year-old male with a 6-month history of clear rhinorrhea, intermittent headaches, and a previous episode of pneumococcal bacteremia complicated by meningitis. A β2-transferrin assay of collected nasal drainage was positive and computed tomography cisternography revealed active CSF extravasation at the right sphenoid sinus roof (Figure 1).
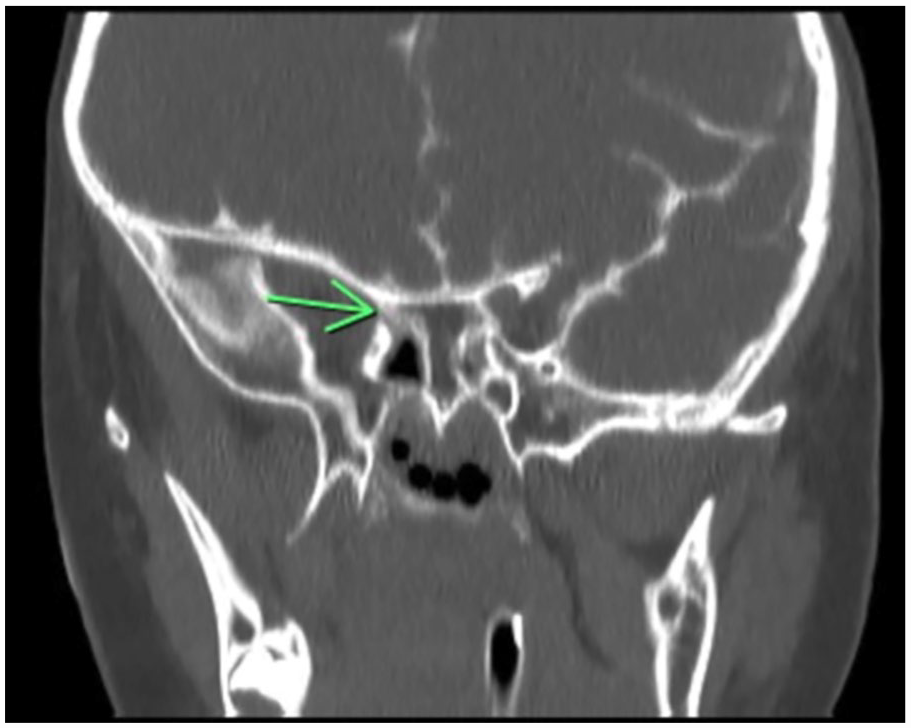
Computed tomography cisternography (coronal) demonstrates a skull base defect across the right sphenoid sinus.
Surgical Technique
The procedure was performed under general anesthesia. Diagnostic nasal endoscopy with a 4-mm 0-degree endoscope was initially unremarkable for an overt CSF leak. A Cottle elevator was used to outfracture the right inferior turbinate to improve endonasal access. One milliliter of 1% lidocaine with 1:100,000 epinephrine was injected into the axilla of the right middle turbinate. A right middle turbinectomy was performed, preserving the middle turbinate mucosa on the back table for subsequent use as a free mucosal graft.
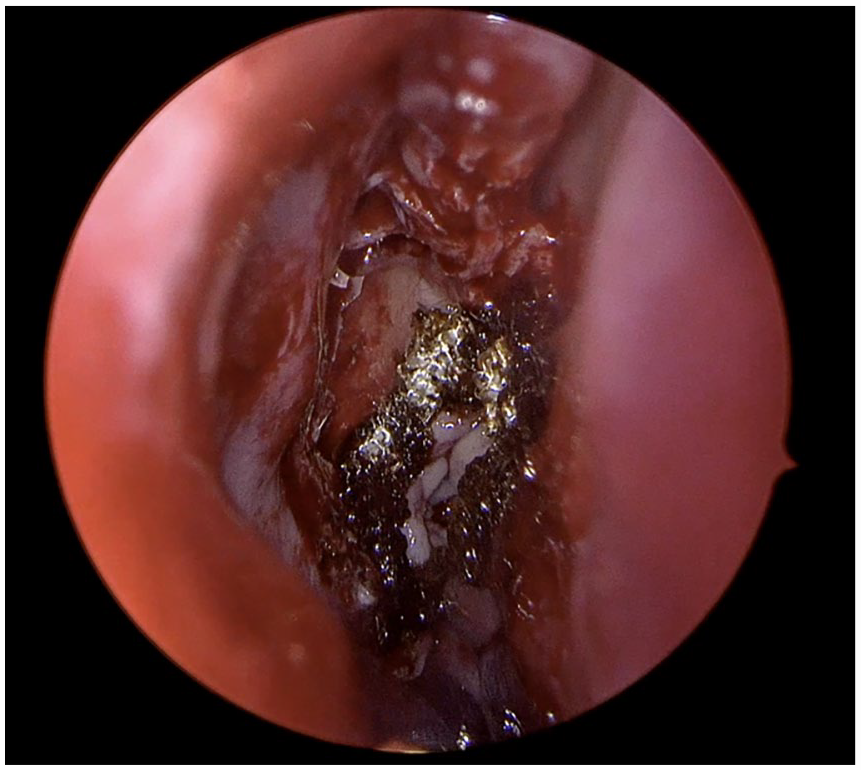
A total sphenoethmoidectomy was performed using 1 and 2mm Kerrison rongeurs and a Mushroom punch. A Cottle elevator was used to strip all mucosa from the right sphenoid sinus before identifying the precise location of a low-flow CSF leak using a Valsalva maneuver (Figure 2). A ball tip probe was used to gently position the free mucosal graft against the skull base defect and to ensure complete graft contact with underlying bone. Lastly, Surgicel was used to create a seal around the edge of the free mucosal graft and Gelform was placed within the ethmoid cavity to further buttress the cranial basae reconstruction (Figure 3). A lumbar drain was placed and removed on postoperative day 3. Prophylactic cefazolin was administered while the lumbar drain was in place. The patient did not experience any postoperative complications.

Cerebrospinal fluid (CSF) leak site across the right sphenoid sinus.
Final skull base repair with free mucosal graft in place with surgicel buttressing the skull base reconstruction.
Postoperative Outcome
Second look nasal endoscopy and debridement in the operating room under general anesthesia on postoperative day 21 revealed a viable mucosal graft with no evidence of CSF leak on multiple Valsalva maneuvers. At 1 year postoperatively, there was no evidence of CSF leak recurrence or long-term complications.
Discussion
Congenital skull base defects are thought to be related to Sternberg’s canal, the result of incomplete fusion from the lateral greater wing of the sphenoid with the posterior basisphenoid. 2 Earlier studies have disputed its location and existence. Nonetheless, recent studies have found that Sternberg’s canal is a consistent anatomical structure with an incidence that is inversely proportional to the studied population’s age. 1
Endoscopic approaches are becoming increasingly popular due to their minimally invasive nature and high success rates. 3 The use of endonasal pedicled flaps such as the nasoseptal flap (NSF) has become a commonly employed technique for CSF leak repair. The NSF is a reliable and versatile flap based on the posterior septal branch of the sphenopalatine artery. Even though recent publications in children undergoing endoscopic endonasal approaches demonstrate no impact on craniofacial growth, 4 NSF use in the pediatric population has the potential for disruption of the sphenodorsal zone, an essential growth center. 5 It may also be more technically challenging to harvest in young children due to the small size of the nasal cavity. 6
The free middle turbinate (FMT) graft is an alternative reliable source of sinonasal tissue with reduced donor-site morbidity and good success rates in effectively repairing CSF leaks.7,8 Importantly, the use of this graft typically preserves nasal function, reducing the occurrence of postoperative complications related to nasal obstruction or altered airflow. However, limited availability of graft tissue endonasally may necessitate alternative techniques (ie, abdominal fat graft, fascia lata graft, pericranial flap, etc.) which must be considered in cases with larger skull base defects.
Following CSF leak repair, postoperative nasal debridement within 4 weeks is critical to remove accumulated crusting, debris, and clots which may impede adequate healing and create a potential nidus for infection. This also promotes neovascularization and a more efficient healing process. Finally, it can help identify any areas where the mucosal graft may be nonviable and at risk for complications (ie, persistent CSF leak), allowing for prompt identification and intervention.
Conclusion
The uninarial endoscopic endonasal approach is safe and feasible for repairing spontaneous CSF leaks in the pediatric population. The middle turbinate free mucosal graft is a valuable and effective tool in the armamentarium of the pediatric skull base surgeon to reconstruct low-flow CSF leaks with minimal sinonasal morbidity.
Footnotes
Consent Statement
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
Our institution does not require ethical approval for reporting individual cases or case series.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.