
Abstract
Glomus tumors are rare vascular tumors that originate in the glomus bodies. These tumors are uncommon in the head and neck region and are extremely rare in the nasal cavity. Intranasal glomus tumors mostly have a clinical and radiologic indolent behavior. This report presents the clinical, pathological, and radiological features of a 60-year-old female patient with a glomus tumor that has an atypical size and location.
Introduction
Glomus tumors (GT) are benign vascular tumors that originate from glomus bodies. The incidence of intranasal GT is limited to case reports reported in the literature. Another review of the literature stated that tumors are located more frequently in the nasal septum, their size is less than 1 cm, and the predominant symptom is epistaxis and/or nasal obstruction. 1 Most cases of nasal GT cases are benign, although aggressive or malignant changes can develop very rarely. 2 We presented a 60-year-old female patient with a glomus tumor obliterating the right nasal vestibulum and nasal cavity.
Case Report
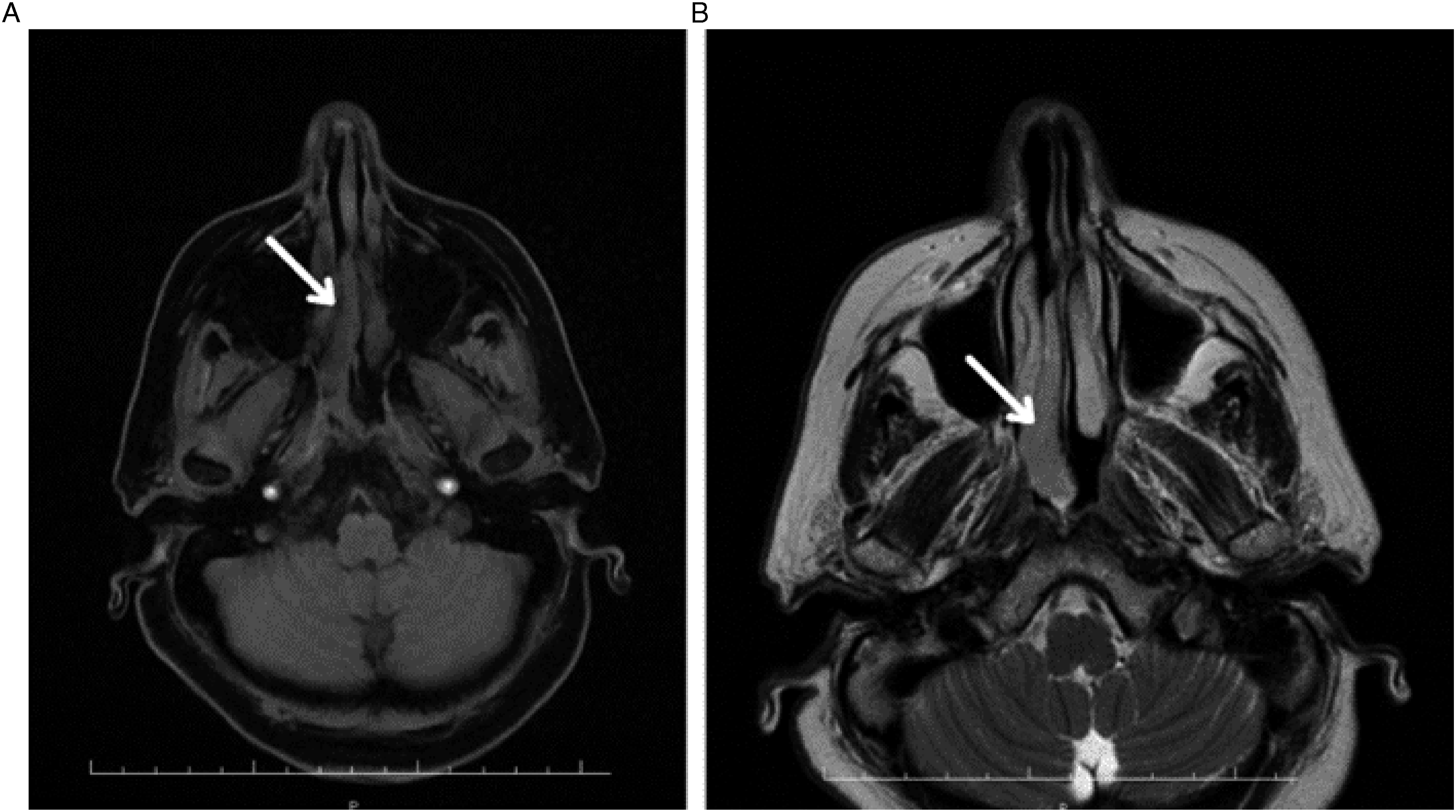
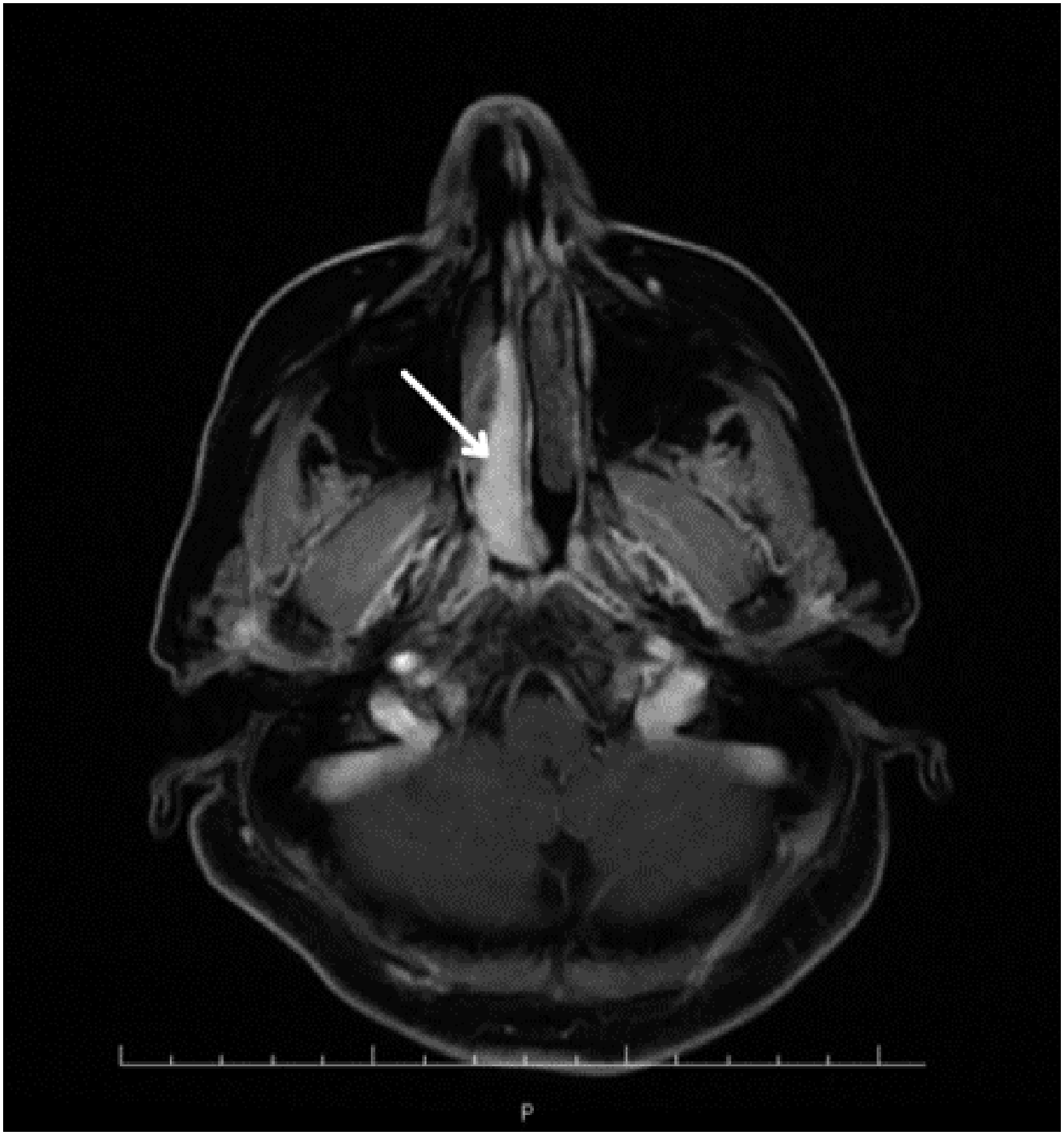
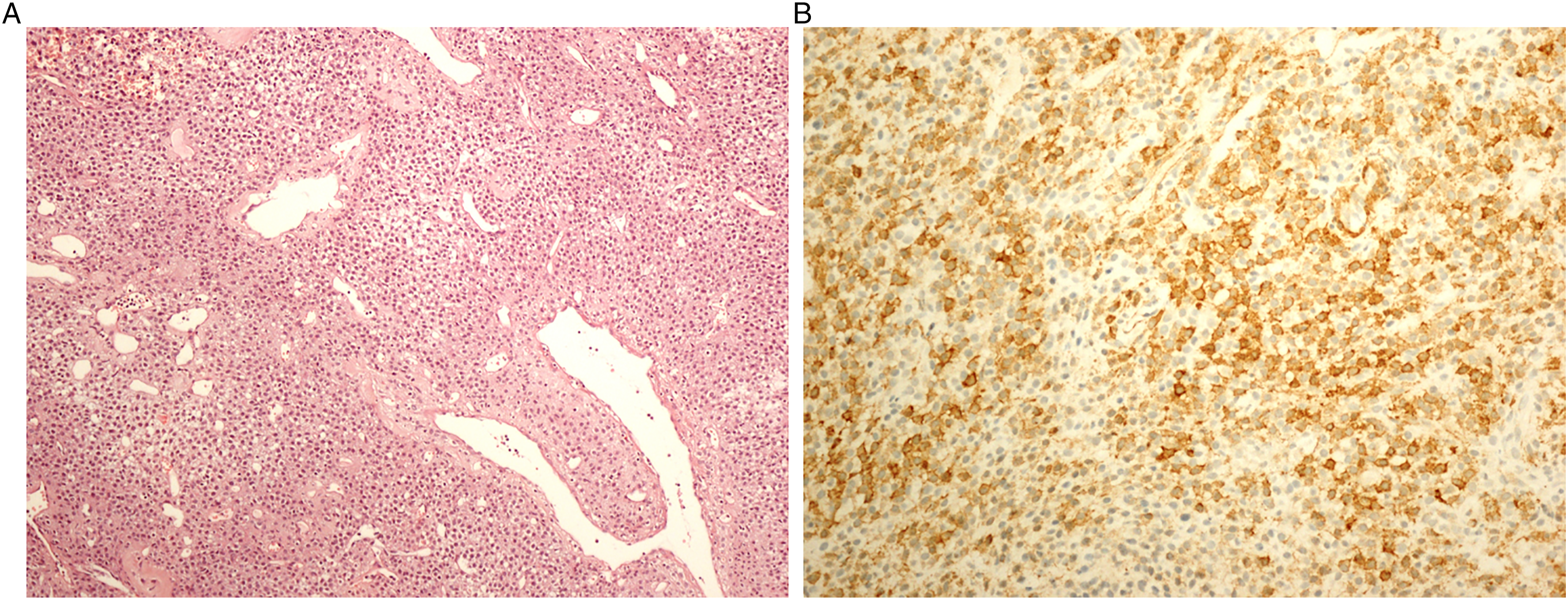
A 60-year-old woman was admitted to our hospital’s otolaryngology clinic with pain, right nasal obstruction, epistaxis, and snoring. Anterior rhinoscopy revealed a smooth-surfaced polypoid mass located on the posterior right side of the nasal septum and expanding to the choana. Computed tomography (CT) demonstrated a well-circumscribed tubular soft tissue density that extends from the medial side of the middle turbinate to the right side of the nasopharyngeal air passage (Figure 1). Contrast–enhanced magnetic resonance imaging (MRI) revealed a well-circumscribed mass obstructing the right nasal cavity and nasopharyngeal air passage, isointense on unenhanced T1-weighted (T1W) fat-saturated image, and mildly hyperintense on T2-weighted (T2W) image (Figure 2A-B). The lesion showed homogeneous and intense contrast enhancement on post-contrast images (Figure 3). Radiological imaging also showed that the mass did not have an extension to structures nearby. After imaging, a punch biopsy was performed. Microscopic evaluation revealed a tumoral lesion composed of uniform round cells with bland nucleus eosinophilic cytoplasm and branching vasculature. Tumor cells were immunohistochemically positive for SMA (Figures 4A-B). Therefore, the histomorphological and immunohistochemical features were compatible with GT. The patient went to surgery afterward. The result of excisional biopsy was a glomus tumor with uncertain malignant potential. No intracranial or orbital extension was demonstrated during the operation. There was no recurrence during the 48-month clinical follow-up of the patient and a CT examination was performed in the post-operative 15th month (Figure 5). Axial non-contrast CT image; a well-circumscribed tubular soft tissue density extending from medial side of the middle turbinate to right side of nasopharyngeal air passage (white arrow). Axial magnetic resonance images; a well-circumscribed mass obstructing right nasal cavity and nasopharyngeal air passage demonstrating isointense signal on unenhanced T1-weighted fat-saturated image (A) and mildly hyperintense signal on T2-weighted image (B) (white arrowheads). Intense and homogenous contrast enhancement in the lesion on axial post-contrast T1-weighted fat-saturated image (white arrow). Sheets of round shape glomus cells and branching capillary-sized vessels in microscopic evaluation (H&E, ×100) (A) and positive immune staining with SMA (İHC, x200) (B). No recurrence in the right nasal cavity on axial non-contrast CT image performed at the post-operative 15th month.

Discussion
GTs are rarely found in the head and neck region and are seen less frequently in the nasal cavity. These tumors constitute 0.4% of non-epithelial tumors of the nasal cavity, paranasal sinuses, and nasopharynx. 3 In the sinonasal region, GTs usually show a benign clinical course. 4 The local recurrence rate of GT is about 10% and can be greater than 30% in the case of incomplete resection.
Most of the reported intranasal glomus cases are seen in the older population with a mean age of 54 (24–89). Females seem to be affected more frequently (female/male ratio: 2). 1 Our patient was a 60-year-old female.
The most common symptoms in patients with glomus tumors are nasal obstruction and/or epistaxis. Patients may present with pain and may even be asymptomatic.1,4 In the case presented, the patient's symptoms were pain, intermittent nasal obstruction, and epistaxis, as reported in the literature.
The gross appearance of intranasal GTs resembles a nasal polyp and other more common vascular tumors, such as hemangioma. 4 They also usually have a size of less than 1 cm. 1 The GT in our case had a polypoid appearance similar to that of the literature. However, it differs in that it was large enough to obliterate the right nasal cavity.
In microscopic examination, the tumor cells (glomus cells) surround small vessels. Glomus cells are uniform, large, spherical cells with eosinophilic granular-staining cytoplasm and centrally located round nuclei. Cellular atypia is not observed. 2 In our case, the histomorphological and immunohistochemical features were compatible with the glomus tumor.
There are no specific or well-defined imaging findings on CT for differential diagnosis. On MRI, glomus tumors typically appear as well-circumscribed masses that are iso-hypointense in T1W images and hyperintense in T2W images, and demonstrate homogenous and marked enhancement in post-contrast images. 5 The findings in our case were consistent with the aforementioned MRI features. Both CT and MRI examinations indicated that the mass had high vascularity and no prominent bone invasion.
Treatment of intranasal GT is total excision. The prognosis is excellent, except in cases of incomplete resection. Similarly, the tumor was completely excised and no recurrence was observed in the 48-month follow-up in our case.
Conclusion
The nasal cavity is an atypical position for the GT. In this article, we present a patient with intranasal GT, which differs from the literature due to its larger size. To our knowledge, the number of intranasal glomus tumors reported in the literature is very limited. Therefore, we believe that it is important to describe the features of this case and to emphasize its similarities and differences with other reported cases. The clinical, pathological, and radiological features were similar to those of other reported cases except for the size of tumor. In the nasal cavity, GTs should be kept in mind when the differential diagnosis of lesions with T2-hyperintensity and homogeneous, marked contrast enhancement on MRI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.