
Abstract
Prostate cancer metastases involving the orbit and/or paranasal sinuses represent a rare oncological presentation. Patients can have a myriad of symptoms such as proptosis, periorbital swelling, blurry vision, rhinorrhea, epistaxis, anosmia, or others depending on the structures involved. The differential diagnosis of paranasal sinus masses on imaging studies is broad and can include inflammatory, congenital, or neoplastic masses; leading to the requirement of biopsy for definitive diagnosis. Tissue sample is usually obtained via an endoscopic approach. The prognosis of such a presentation is not well described in the literature, but it is usually guarded due to the advanced stage of the disease and generally a poorly differentiated primary tumor. Treatments usually aim to reduce the burden of disease and debulk the tumor mass for palliative purposes. We present a case of a 71-year-old male presenting with unilateral proptosis and periorbital swelling secondary to prostatic metastasis.
Introduction
Prostate cancer with metastases to the paranasal sinuses is a rare oncological presentation. 1 In general, prostate cancer metastasizes to regional pelvic lymph nodes and axial skeleton. 2 The most common malignancy spreading to the paranasal sinuses is a primary renal cancer; other reported sites of origin include breast, pulmonary, colorectal, central nervous system, thyroid, endometrial hepatic, or prostate.2-10 In previous reports, prostatic metastases involving the head and neck region included the parotid, pituitary gland, cervical spine, optic canal, and skin.11-16 Orbital metastases constitute around 1–13% of neoplasms involving the orbit.17-19
Several hypotheses exist regarding the routes that prostate cancer metastases can take to arrive at the paranasal sinuses. Previous literatures theorize that the primary tumor metastasizes via hematogenous dissemination, utilizing the non-valved vertebral venous plexus and traversing from the site of primary malignancy to the cavernous, pharyngeal, or pterygoid venous plexuses, and eventually depositing in the paranasal sinuses. The maxillary sinus is the most involved paranasal sinus, likely due to the strong vascular supply via branches of the external carotid artery that communicate with the pterygoid plexus.20-23 Lymphatic spread is another proposed mechanism of spread. The neoplastic cells travel from local pelvic or abdominal lymph nodes to the thoracic duct and then spread in a retrograde fashion to the head and neck regions via intercostal, mediastinal, or supraclavicular lymphatics.24-27
The presentation of paranasal sinus metastases is highly variable and may include ophthalmologic symptoms (proptosis, blurry vision, diplopia, and ptosis), rhinologic symptoms (nasal fullness, anosmia, epistaxis, and rhinorrhea), facial deformity, or headaches.27-31 We present a rare case of a 71-year-old male with a history of prostate cancer who presented in our emergency department with left periorbital edema and exophthalmos.
Case Report
A 71-year-old male with stage IV prostate cancer presented to the emergency department with a five-day history of left periorbital swelling and proptosis one month after completing chemo-radio therapy. This was associated with occasional blurry vision, without any complaints of eye pain, chemosis, nasal obstruction, or nasal discharge. On ophthalmological examination, his left eye was proptosed by 6 mm and extra-ocular movements were limited. His visual acuity, however, was 20/20 bilaterally. Laboratory results showed an elevated C-reactive protein of 35–68 mg/L, neutropenia (neutrophil 1.07x109/L) and elevated lactate dehydrogenase at 2015U/L.
Computed tomography (CT) scan demonstrated a left supraorbital extraconal mass measuring 2.8 × 3.5 cm involving the posterior orbit, and asymmetric sinusitis within the maxillary, ethmoid, and frontal sinuses (Figure1). Our patient was started on intravenous antibiotics for periorbital cellulitis with minimal response. He underwent further work-up with magnetic resonance imaging (MRI). This demonstrated a large extraconal mass located within the left superior orbit, a mass-like opacification of the left and posterior right ethmoidal air cells, and bilateral inferior frontal and left anterior temporal nodular pachymeningeal involvement with suspected leptomeningeal involvement. There was diffuse signal abnormality of the base of skull. (A) Computed tomography scan demonstrating left orbital extraconal mass (B) with resultant left-sided proptosis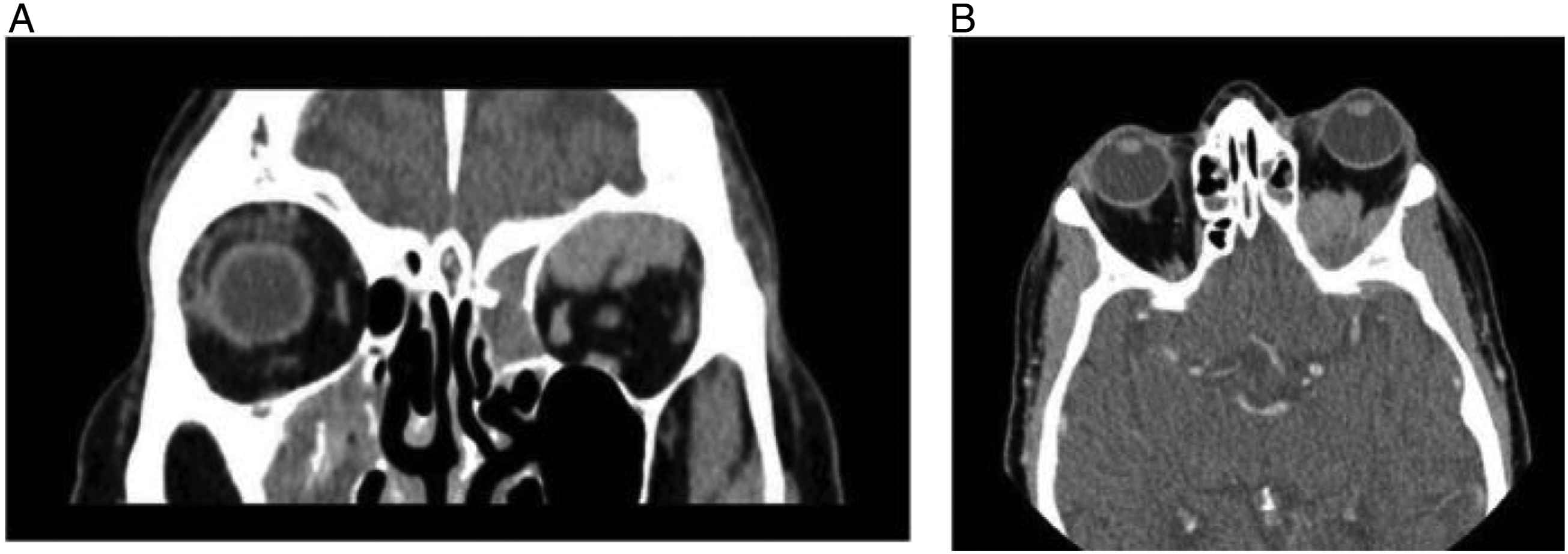
The patient underwent emergent functional endoscopic sinus surgery for debridement and biopsy. An abnormal, fleshy, polypoid lesion in the left posterior ethmoid region along the lamina papyracea and skull base were sent for histopathological analysis. On microscopic evaluation of the mass, the tumor showed a vaguely glandular and fused cribriform pattern of growth. The neoplastic cells had amphophilic cytoplasm, high nuclear to cytoplasm ratio, and conspicuous nucleoli with areas of high mitotic activity and lacked significant pleomorphism. There was also prominent lymphovascular invasion (Figure 2). Immunohistochemical stains show that the tumor is positive for AE1/AE3, NKX3.1, prosthein, and PSMA, while negative for racemase, p63, CK34BE12, CK5/6, p40, CK7, CK20, TTF-1, Napsin-A, synaptophysin, chromogranin, CD56, CD45, S100, HMB-45, Melan-A, and in-situ hybridization stain for EBER. Considering the clinical history, histology, and immunohistochemical profile, the diagnosis was consistent with metastatic adenocarcinoma of prostate origin. Unfortunately, the disease progressed, and our patient passed away shortly after initial presentation. (A) 10X H&E of left ethmoid mass excision. The tumor consists of atypical cells with prominent nucleoli (inset), and amphophilic cytoplasm showing a fused cribriform architectural growth pattern. (B) Evidence of lymphovascular invasion is noted. The lesion was diffusely positive for NKX3.1 (C) and showed positivity for PSMA (D)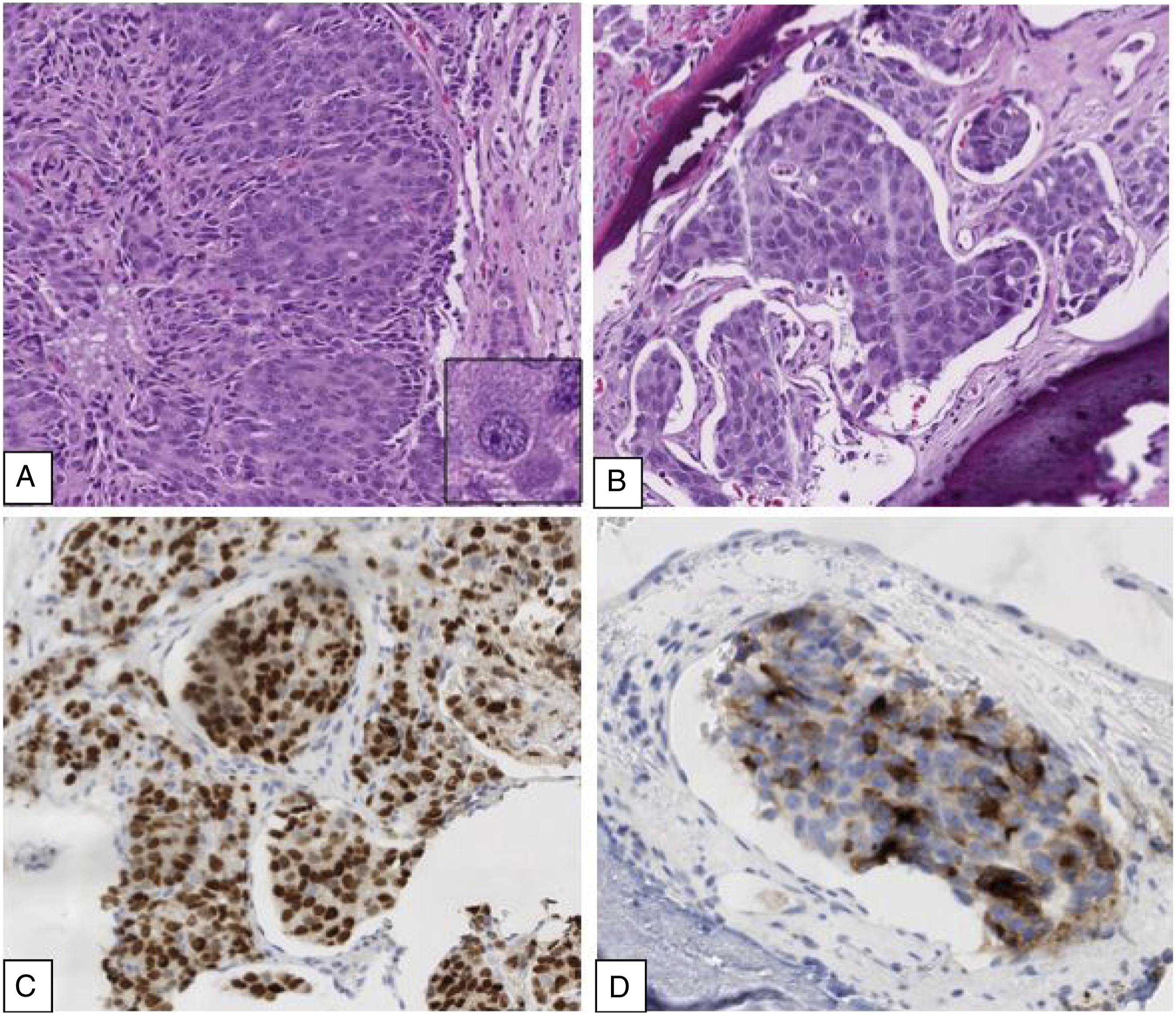
Discussion
The orbit is at the junction of many important anatomical structures, such as the brain, nose, nasopharynx, paranasal sinuses, and all ocular structures. Pathologies in any of these areas can place pressure on the orbital contents and cause proptosis, which was the primary complaint of this patient. Unilateral proptosis has a wide differential diagnosis, including hemangiomas, post-traumatic hematomas or encephaloceles, orbital complications arising from sinusitis, orbital pseudotumor, Graves’ disease, and primary and metastatic cancer diagnoses, granulomatous diseases, among others. 32
Paranasal sinus and orbital metastases of solid tumors continue to be relatively rare, with a quoted rate of 1% of patients with a cancer diagnosis having dissemination to the head and neck. 33 Renal cell carcinoma, followed by breast and lung cancers are the most common tumors that metastasize to the paranasal sinuses. For orbital metastases, breast and lung cancers are the most common primary malignancy, followed by prostate cancer, excluding leukemia and lymphoma.33,34 In a review of the US Healthcare Cost and Utilization Project Nationwide Inpatient Sample including 74,826 patients with metastatic prostate cancer between 1998 and 2010, there were no reported cases of metastases to the paranasal sinuses or to the orbit. 35 However, the diagnosis of metastatic disease was considered and prioritized for our patient given his medical history of recent and progressive prostate cancer.
It is important to understand the differential diagnoses, such as lymphomas, meningiomas, or infectious causes. Orbital and paranasal lymphomas are rare, respectively representing 2% and 0.17–1.5% of all lymphomas. However, 50% of orbital masses and 5.8% of nasal and sinus masses are lymphomas. 36 The clinical picture is similar to what our patient experienced, as they generally develop periorbital swelling, diplopia and proptosis, nasal or sinus congestion, and restriction of eye movement on examination. 36 Differentiating lymphomas from other malignant entities require tissue diagnosis.
Meningiomas can be considered in the differential diagnosis for this patient given the CT scan findings of nodular enhancement of the dura overlying the left cavernous sinus, anterior left temporal bone, and bilateral inferior frontal lobes. Meningiomas are the most common tumor of the meninges and are generally benign, although there are multiple variants that may behave more aggressively. 37
While our patient did not have the typical nasal symptoms of acute sinusitis, he presented with new onset visual changes, periorbital swelling and proptosis. A review of 200 patients with metastatic disease of the paranasal sinuses, 23.5% presented with proptosis and 24% presented with visual changes—symptoms shared with infectious complications of acute sinusitis. 38 An infectious etiology was considered for this patient due to the acuity of his symptoms, the asymmetric sinus involvement on initial CT scan, and his elevated C-reactive protein given that he was an immunocompromised host. Invasive fungal infections tend to happen in immunocompromised individuals (Poorly controlled diabetes, Patients undergoing chemotherapy, and hematological malignancies).Importance of early diagnosis in invasive fungal infections is highlighted by the high mortality (50–80%) owing to the invasive nature into the orbits and intracranial cavity; Thus, prognosis of such condition is dependent on early and precise diagnosis with rapid initiation of antifungal therapy and surgical intervention.38-40
However, given the patient’s personal history, thorough work-up to rule out metastatic disease to the paranasal sinuses is essential. These investigations are reliant on MRI/CT imaging that demonstrate characteristic features of the diagnosis, size and extension of the disease, and involvement of surrounding soft tissue and any at-risk structures. These results all assist in proper surgical planning. Additionally, histological analysis is of utmost importance since imaging alone is not sufficient to identify differences between primary malignancy and metastases involving the paranasal sinuses. 3
Management of metastases to the paranasal sinuses is usually with the goal of palliation. The goals of treatment are to improve the patient’s quality of life, reduce pain, and prevent epistaxis. Due to rarity of this presentation, there is no current consensus on best treatment option. Treatment options discussed in the literature include radiotherapy, chemotherapy, hormonal therapy, immunotherapy, and endoscopic surgery.41-43
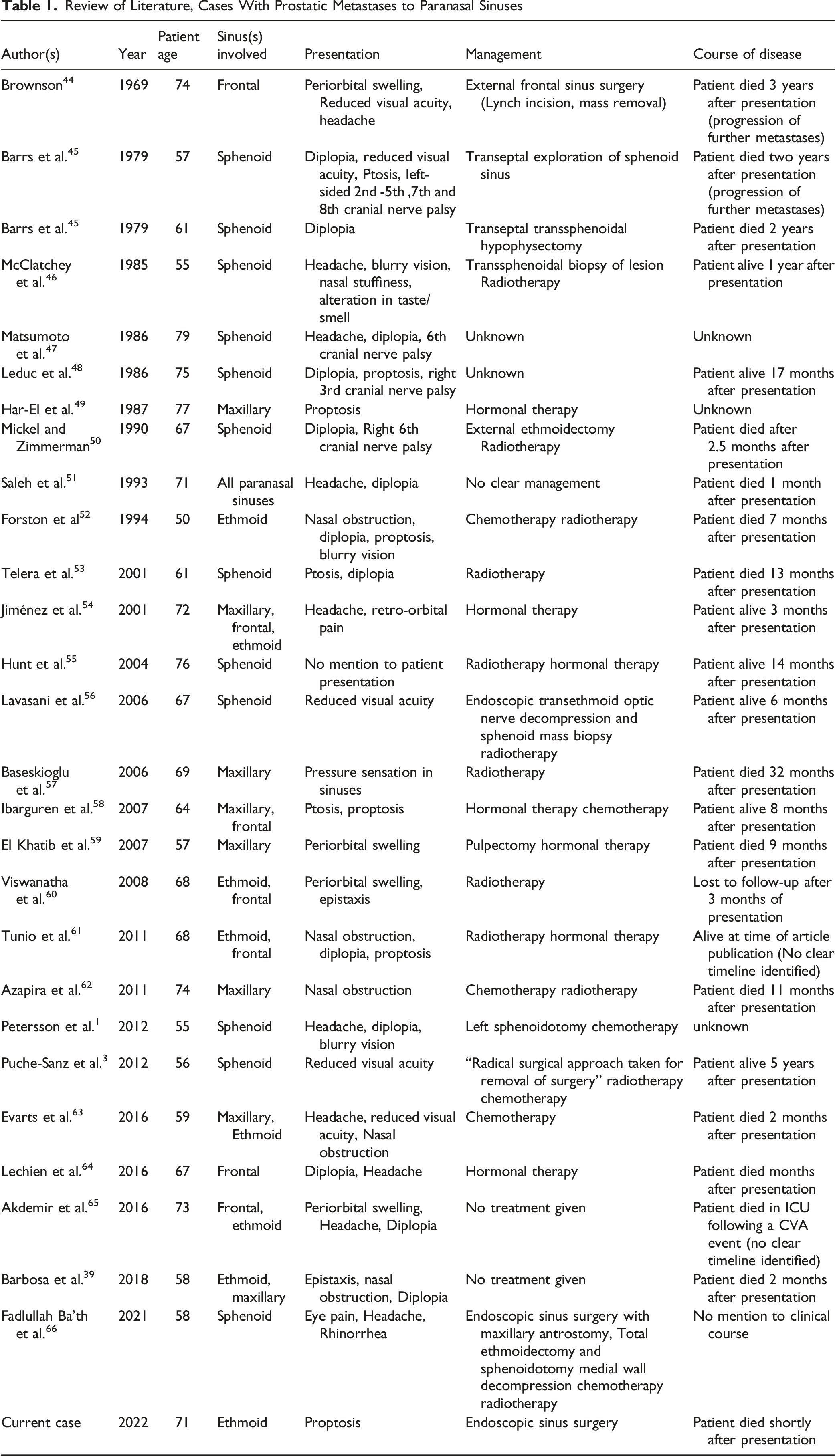
Review of Literature, Cases With Prostatic Metastases to Paranasal Sinuses
In conclusion, although our patient presented with relatively non-specific symptoms, his primary diagnosis of prostate adenocarcinoma raised our suspicion for a metastatic process, despite prostate cancer spreading to the paranasal sinuses and orbit being a rare entity. The purpose of the case is to highlight the importance of maintaining a broad differential diagnosis and staying alert to key features from history obtained when tackling unusual clinical cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval is not applicable for this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Informed Consent
Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.