
Abstract
Objective
For microtia patients with excessively insufficient postauricular skin, it is difficult to obtain a satisfied outcome with existing strategies. In this study, we developed a modified tissue expander method for auricular reconstruction.
Methods
The modified tissue expander method divided into 4 stages. In the first stage, a 30 ml or 50 ml kidney-shaped tissue expander was implanted in the mastoid region. A short time expansion (average 33.5 days) was conducted subsequently. In the second stage, the expander was removed and a modified cartilage framework without tragus was inserted through the same incision. A crescent-shaped cartilage pad was inserted into the incision of cartilage-harvest site at the same time. In the third stage, the reconstructed ear was elevated. Lobule rotation and remanent modification were performed in the fourth stage. The patients were followed up between half a year and 10 years. The outcomes of the reconstructed ears were scored with evaluation criteria.
Results
From January 2010 to December 2019, a total of 45 microtia patients with excessively insufficient postauricular skin were performed the modified tissue expander method. Fourty-two patients showed satisfied outcomes. Complications such as hyperpigmentation in the skin graft area (3, 6.7%), scar hyperplasia (3, 6.7%) and folliculitis (1, 2.2%) were found. There were no complications related to the tissue expander.
Conclusion
The modified tissue expander method is an effective and safe technique for auricular reconstruction in patients having excessively insufficient postauricular skin, with satisfying medium-term results.
Introduction
Microtia is a common congenital craniofacial malformation, often associated with different extent of auricular deformities, atresia or stenosis of the external auditory meatus, and middle ear abnormities. 1 Ear reconstruction for microtia with costal cartilage remains a huge challenge for plastic surgeons around the world.
After Tanzer first introduced the modern ear reconstruction method, 2 Brent and Nagata developed the two-stage method,3-7 and the two-stage Nagata method becomes the mainstream option nowadays. 8 However, for microtia with insufficient skin coverage, the use of Nagata technique can lead to some complications, such as great tension of flap and deformation of framework. Tissue expansion is a good option to expand the insufficient postauricular skin flap. 9 Neumann, Park, and Zhang have made landmark contributions by developing tissue expansion methods, which obtained satisfied results these years.10-12 However, patients with tight and insufficient mastoid skin are more likely to suffer from the exposure of the expanders and the ischemia to the expanded flap. Moreover, complications such as necrosis and a thick capsule often occur in the late expansion period, which hindered the popularization of the expanded flap method. 13 As a result, a safe and effective technique for microtia patients with excessively insufficient postauricular skin is still required.
In our clinical practice, we introduced a modified tissue expander method to overcome soft tissue deficiency and avoid complications in long-term expansion. We introduced tissue expander under the postauricular skin flap to obtain thinner and larger skin coverage. After 1–1.5-month expansion, the framework was implanted without tension and obtained a distinct contour. Reconstructed ear elevation, lobule rotation, and modification of the remnant ear ensued. With this surgical strategy, minimal postauricular skin was required, and all patients achieved satisfied and stable results without severe complications.
Patients and Methods
Patients
Characteristics of Patients.
Operative procedures
Implantation of tissue expander
From a 3-4 cm incision within 0.5 cm of the hairline, the tissue expander pocket was created between the subcutaneous layer and the postauricular fascia. With the help of an X-ray film template and tissue expander, the range of dissection was approximately 0.5 cm around the tissue expander. The undermost bound was the level of the contralateral lobule, and the anterior bound was the remanent cartilage. With careful dissection, the postauricular fascia and subcutaneous vascular network should be preserved intact. Then a 30 ml or 50 ml kidney-shaped tissue expander was implanted in this pocket. The size of the tissue expander mainly depended on the size of the normal ear. Saline injection began at one week after introduction and reached about 50 ml in 4 weeks. The final volume of expansion was depended on the thickness and tension of the expanded flap by plastic surgeons. The second stage would be performed after one week of maintenance.
Framework implantation
The tissue expander was removed from the implantation incision. The seventh, eighth, and part of the sixth costal cartilage were harvested to fabricate the base frame and crescent-shaped pad. Unlike the cartilage framework in the Nagata method or traditional tissue expansion method,4,12 the base frame here was fabricated without tragus or support parts. Before implantation of the base frame, the thickness of the expanded flap was examined. The thick area, which may affect the appearance and showed good blood irrigation, could be removed properly. The framework was inserted into the expanded pocket through the same incision. Negative pressure derived from a drainage was used to form the contour of the framework (Figure 1). The crescent-shaped pad was then inserted into the incision of cartilage-harvest site waiting for ear elevation in the next stage. The drainage would be removed after around 5 days. Framework implantation. (Left, figure 1A) The expanded flap showed proper thickness. (Center, figure 1B) Fabricated ear framework. (Right, figure 1C) Instant outcome after ear framework implantation without capsulectomy.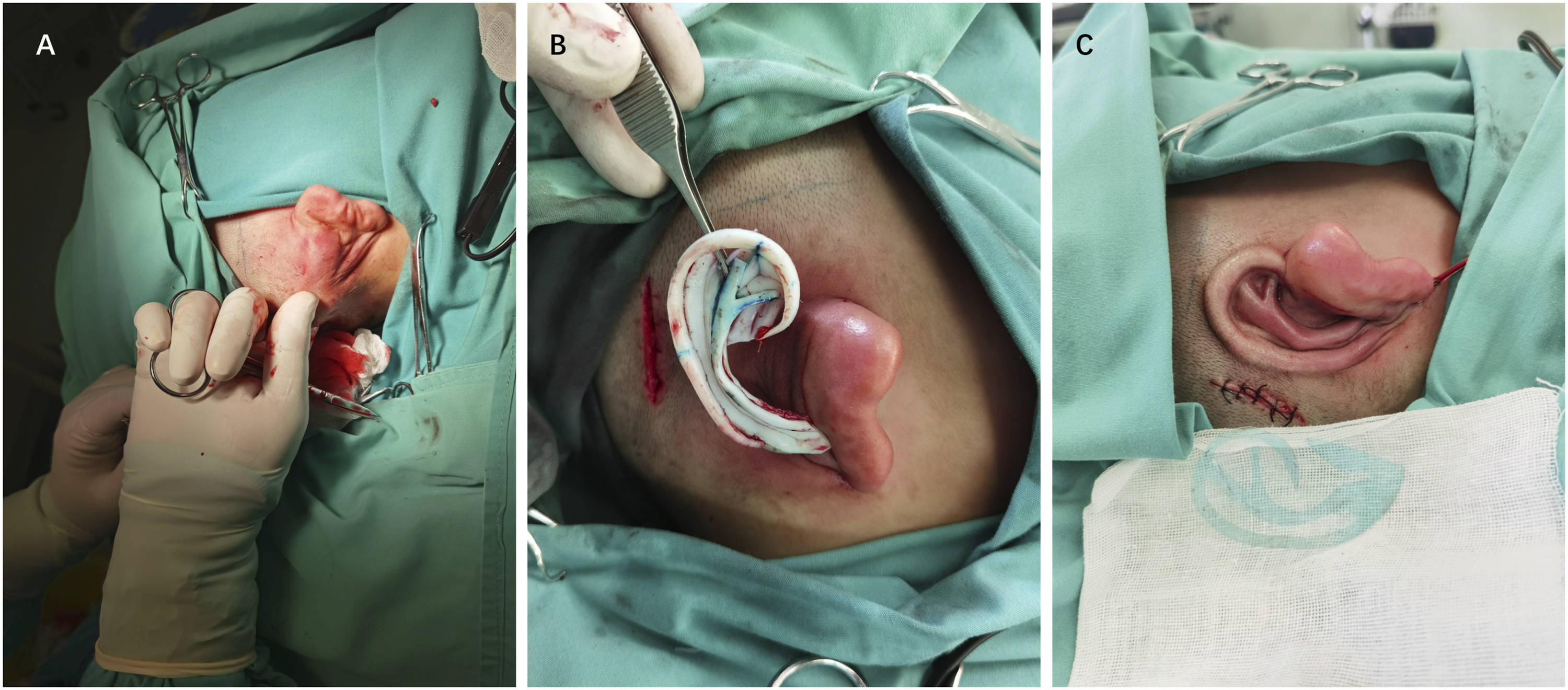
Reconstructed ear elevation
Six months after the implantation of the framework, the base frame was lifted from the helix incision. The crescent-shaped pad was removed from the cartilage-harvest site and trimmed into a suitable shape to enhance the projection of the reconstructed ear and form the concha cavity. We harvested the postauricular fascial flap with a pedicle in the remanent ear and fixed it to the helix to cover the posterior surface of the reconstructed ear. Full-thickness free skin grafts with suitable size were harvested from the cartilage-harvesting incision or groin to cover the fascial surface. The suture was removed after 10 days.
Rotation of the lobule and modification of the remnant ear
Lobule rotation of different types of microtia was performed with a variant Z-plasty, which was detailed by Nagata.4-6 From the lobule incision, the remanent cartilage was removed and reshaped into a tragus of the lobule type. With redistribution of the skin flap, crus of the helix, tragus, and the intertragus was formed, and the concha was deepened with removal of cartilage and soft tissue. This stage was performed about four months after ear elevation.
Follow-up
Scoring System of Reconstructed Ear.
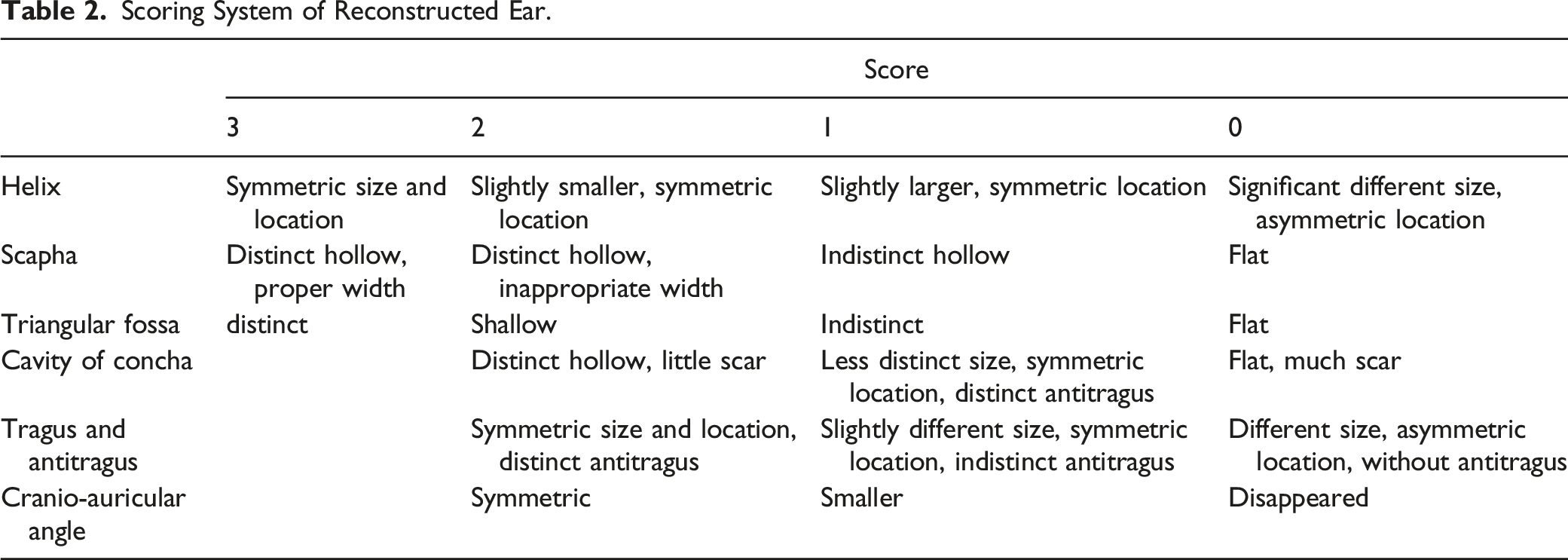
The surgery was completed in 43 patients so far. Two patients did not complete the last stage surgery for personal reasons. According to the scoring system of reconstructed ear mentioned in the Table 2, the last stage surgery can influence scores of tragus and the cavity of concha. As a result, we halved the score of “tragus and antitragus” and “triangular fossa and cavity of concha” for these 2 patients.
Results
A total of 45 patients (45 ears) were performed the modified tissue expander method in this study. The volume of saline injection was 47 ml–62 ml (average, 54 ml). The average time of the expansion period was 33.5 days (range 28-47 days). Complications occurred in 7 patients. Hyperpigmentation appeared in 3 patients (6.7%) in the graft area. And 3 patients (6.7%) showed scar hyperplasia on the reconstructed ear. Six months after ear elevation, they were conducted cicatrectomy and radiotherapy in our hospital. Complication requiring reoperation was found in one patient (2.2%), who suffered from folliculitis on framework. No complication related to tissue expanders was found. During the follow-up, fourty-two patients (93.3%) showed satisfaction with their reconstructed ears. Two patients (4.4%) had partially satisfactory outcomes, and one patient (2.2%) had an unsatisfactory outcome.
Case Reports
Case 1
This was a 33-year-old man with trauma on the left ear. Five years ago, the patient was involved in a car accident that resulted in the loss of most of the structure of his left ear, leaving only a small portion of the tragus. The scar contraction and the postauricular skin was excessively taut (Figure 2A). After 38 days with 55 mL of normal saline injected in total, the patient underwent the second stage surgery (Figure 2B). The reconstructed ear at 1.5 year of follow-up showed a quite distinct appearance and the patient was very satisfied (Figures 2C,2D). The score of this patient was 11. Case 1, a 33-year-old male with left auricular trauma. (A) Preoperative side view of lobule-type microtia. (B) Preoperative side view after first stage with full expansion. (C, D) Side view and back view of the reconstructed ear 1.5 year after the stage of ear elevation.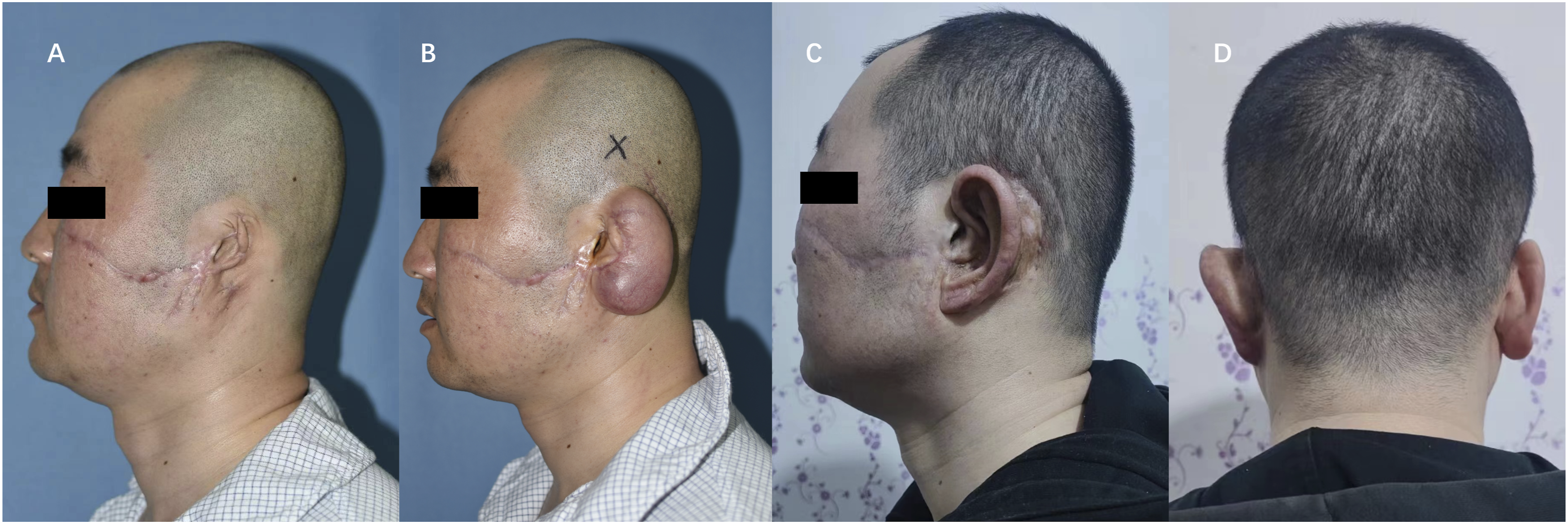
Case 2
This was a 10-year-old boy with congenital lobule-type microtia on the right side. Postauricular skin represented excessive tautness (Figure 3A). This boy received a 50 ml kidney-shaped expander implantation. And 37 days later, he underwent ear reconstruction with a volume of 54 ml saline (Figure 3B). The ear framework remained distinct before the stage of ear elevation (Figure 3C). After a 3.5-year follow-up, the antihelix cartilage showed little absorption, yet the whole ear showed a quite good appearance (Figures 3D,3E). The score of this patient was 11. Case 2, a 10-year-old boy with lobule-type microtia on the right side. (A) Preoperative side view of lobule-type microtia. (B) Preoperative side view after first stage with full expansion. (C) Preoperative side view before ear elevation. (D,E) Side view and back view of the reconstructed ear 3.5 year after the last stage.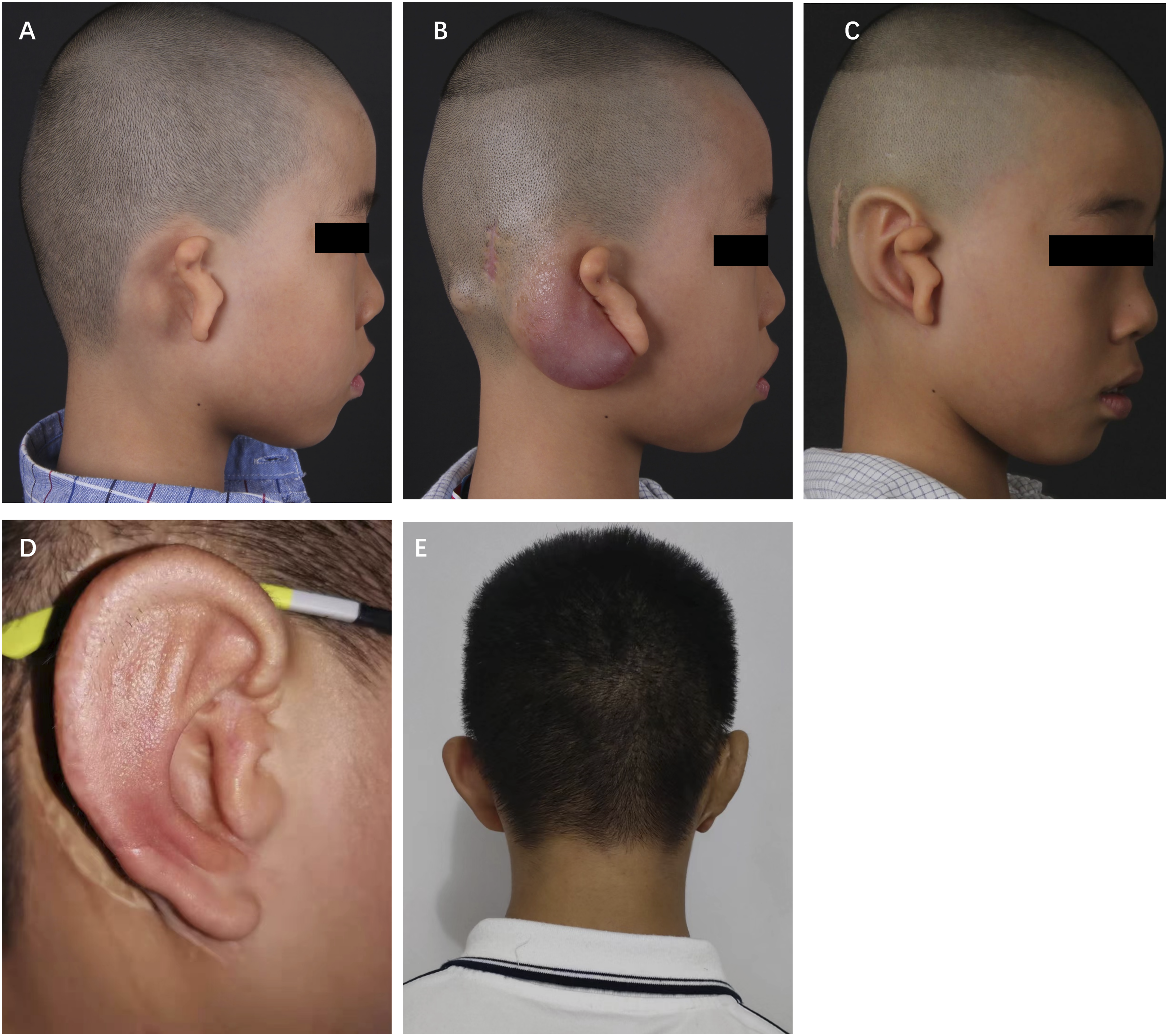
Case 3
This was a 6-year-old boy with right lobule-type microtia (Figure 4A). The residual ear represented a small lobule. This boy received 50 ml kidney-shaped expander implantation and mandibular lengthening at the same stage. The ear reconstruction was performed after a 35-day injection with a final volume of 52 ml of saline (Figure 4B). The mandibular lengthening device was removed in the final stage. Before the modification of the remanent ear, the ear framework showed an excellent appearance compared with the contralateral ear (Figures 4C, 4D). And 3-year follow-up showed that there was still distinct contour (Figure 4E). The score of this patient was 12. Case 3, a 6-year-old boy with right lobule-type microtia. (A) Preoperative side view of lobule-type microtia. (B) Preoperative side view after first stage with full expansion. (C,D) Preoperative side view before ear elevation. (E) Side view of the reconstructed ear 3 year after the last stage.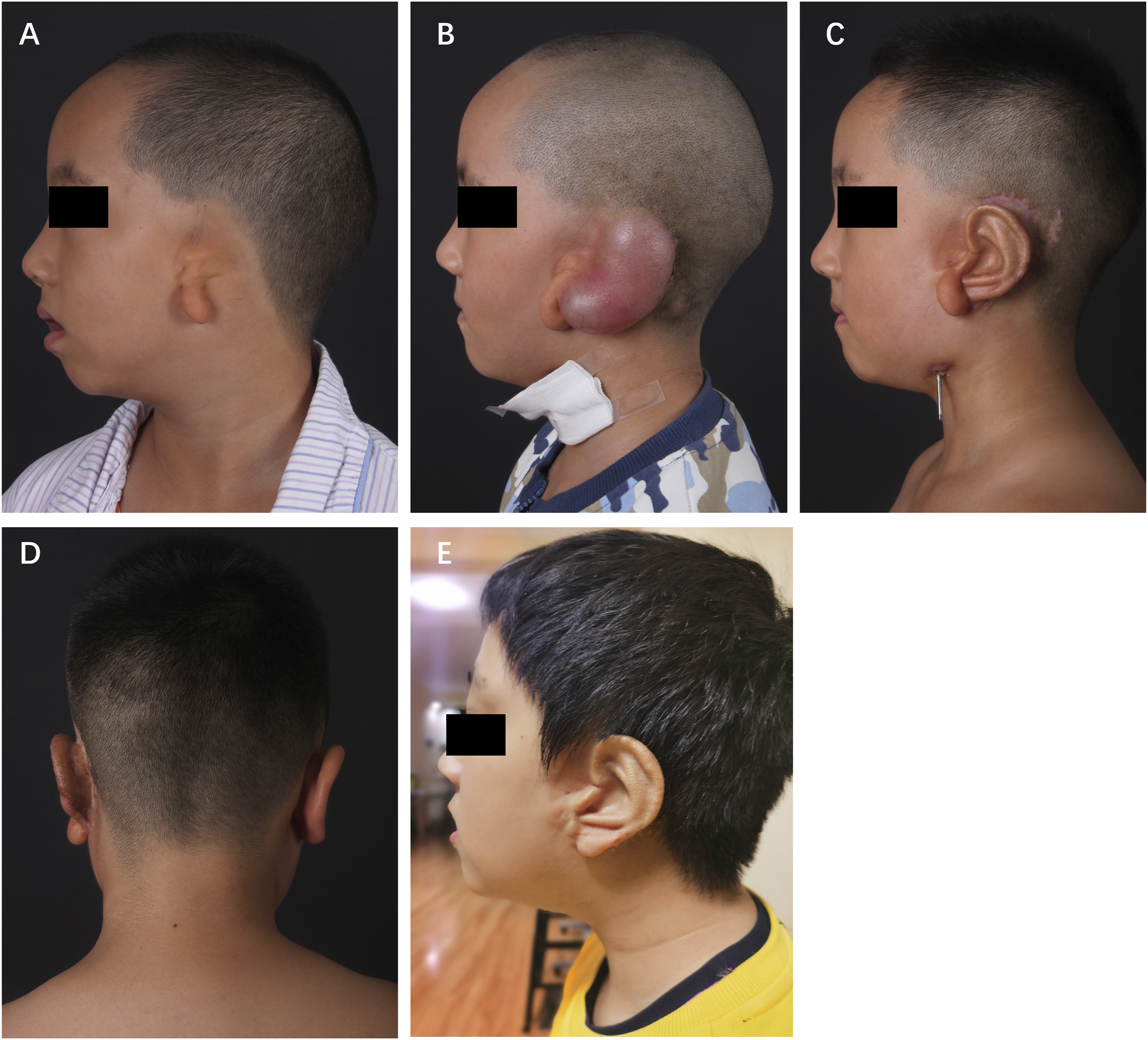
Discussion
Successful reconstructed ears always have 2 requirements: (1) a vivid and stable framework and (2) a tension-free skin coverage with sufficient blood supply. Due to the close location, matching color, and texture with the contralateral ear, postauricular skin was seen as the suitable coverage for the anterior aspect of the ear framework.4,11,15 However, low hairline, low elasticity, excessive thickness, and scarring in the periauricular region can lead to very insufficient skin for ear reconstruction. 16 Although the two-stage Nagata method is the mainstream option for auricular reconstruction, 8 the barriers to apply the Nagata method are the inadequate thickness and tension of the postauricular skin. Thick and taut skin coverage resulted in indistinct contours. Excessively insufficient skin also leads to great tension and poor adhesion of the skin and the notch of framework. The dead space between framework and flap could result in seroma and the consequent absorption of the protruding cartilage.
Tissue expansion is a good method to overcome the problems mentioned above.9,14,17 Traditional tissue expansion method was usually applied to enlarge the area of the postauricular skin and make it thinner. However, for patients with poorly elastic skin, especially combined with a relatively large contralateral ear, they always required more skin coverage and long-term expansion.18-20 The frequency of saline injection is also difficult to control, as too rapid expansion leads to problems in the blood supply of expanded flap, while too slow causes an overly thick capsule and waste of time.9,13 Furthermore, research showed that complications such as necrosis of the expanded flap and exposure of the tissue expander often occurred in the late expansion period. And in patients with postauricular scars, flap necrosis would be more common, especially in the late period of expansion, and blood supply and skin tension should be carefully monitored.9,13 Long-term compression of the tissue expander can also affect the blood supply of postauricular fascia flap.
In terms of the sequence of operations, we adopted a rather cautious strategy. This strategy was carried out in 4 stages: implantation of tissue expander, fabrication of the ear framework, elevation of the reconstructed ear and modification of the remanent ear. Compared to the Nagata method and the traditional tissue expansion method, our strategy has some advantages for patients with excessively insufficient postauricular skin as below: (1) Sufficient skin to envelop the base framework. Compared with the Nagata method, the tissue expander could increase the volume of the mastoid skin. With the gradual expansion process, the postauricular dermis and subcutaneous layers can be thinner and the increased skin could easily cover the cartilage frameworks.
12
(2) Less complications related to tissue expander. Short-term tissue expansion has been used for a decade in our center to overcome skin deficiency. To our observation, even though the expanded flap restricted to some extent, it would not cause excessive pressure to the framework. For the base frame in our strategy was wrapped in a dilated cavity, there was enough space for restriction. Besides, compared with the multiple-layer frameworks in the traditional tissue expansion method,11,12 the base frame in our strategy was fabricated without tragus and support parts. It was relatively flat and received less pressure during flap restriction. With the short-term expansion, few complications which were often seen in the late expansion period such as necrosis of the expanded flap occurred with this strategy.
13
(3) Sufficient vascular supply of the flap. The vascular supply is the most important reason for the whole arrangement. Research showed that the vascular supply of postauricular skin consists of both perforators in vertical and subcutaneous blood networks under the dermis, which derive from the remanent ear.
21
The introduction of tissue expander damaged the perforator vessels, so the margin, especially the remanent ear, became the main blood supply of the mastoid skin flap.
11
However, lobule rotation, removal of residual cartilage, and redistribution of skin of the remanent ear would damage the blood supply of this region. Thus, we chose the original incision from tissue expander implantation to insert the ear framework in the second stage. Six months after ear elevation of the third stage, the mastoid region was settled down, and lobule rotation, removal of residual cartilage, and modification of the remanent ear were performed.
The security of the operation was ensured by spreading stages, and the 45 patients showed no signs of complications related to poor blood perfusion. But an increased number of operative stages may delay the normal social life of the patients and the loss of economic benefit. As a result, patients underwent this strategy should be selected prudently. Patients represented with the following characters should be considered as having excessively insufficient postauricular skin: (1) Previous operations such as preauricular fistula excision, canaloplasty, and other deformity correction, which may damage the pedicle of the remnant ear, should be taken into account; 22 (2) Trauma in the periauricular skin area such as burns, bites, or cuts can also be included; (3) severe hemifacial microsomia; (4) After the postauricular skin was pinched and pulled, thick and taut skin was identified.
There are several key technical points to recapitulate.
Park holds the opinion that the dissection of pocket discontinued at 1.5 cm to the remanent cartilage to preserve the vascular supply of the expanded skin flap. 11 However, according to our clinical practice, blood vessels are more abundant in remanent cartilage. Therefore, in the first stage of tissue expander implantation, the dissection of the pocket ended at the cartilage of the remanent ear. For the distance from the helix crus to the outer canthus of the unaffected side is always larger than that of the microtia side, the reconstructed ears located behind the remanent cartilage were found no obvious asymmetry in the 45 patients in this study. 14
Due to the reaction of the immune system, a capsular pocket was formed after the implantation of the tissue expander. 23 One of the most common complications of the expanded flap method is the thick capsule, which may lead to an indistinct contour.17,24 Regarding the management of the tissue expander capsule in this study, in addition to the margin of the expanded flap, there was not a capsule that was overly thick. With an average injection of 52 ml of saline, the expanded flap was thin enough to cover. As is demonstrated in Figure 1, the contour of the reconstructed ear was distinct with even skin coverage. Sometimes a thick capsule can be found in the margin of the expanded flap; local capsule removal can be performed under the dermis due to conservation of the remanent ear.
Nagata proposed the regular use of the temporoparietal fascia flap to elevate the reconstructed ear. 7 However, many surgeons prefer the postauricular fascial flap and view the temporoparietal fascia flap as a tool of salvage. 25 Reinisch et al. published their work on the secondary salvage of unsatisfied ear reconstruction. Unless the temporoparietal fascia flap was damaged in a prior operation, it was still the first choice of covering flap. Among the 144 salvage patients, 76 patients (53%) used temporoparietal to improve unsatisfied appearance, to repair exposure, flap failure, and infection related to cholesteatoma. 26 In this study, we used the postauricular fascia flap to cover the posterior area of the reconstructed ear as Park described in 2000. 11 The anterior postauricular fascia flap is easier to harvest and the use of it could preserve the temporoparietal fascia flap.
The intervals between the second, the third and the fourth stage should be prolonged for safety, especially for patients with scars in the remanent ear. The blood supply of the postauricular region derived from the remanent ear and any damage to that area would result in poor vascular perfusion, which may lead to the failure of ear reconstruction.
Conclusions
The modified tissue expander method is an effective and safe technique for auricular reconstruction in patients having excessively insufficient postauricular skin, with satisfying medium-term results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Special Research Fund for Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (YS202041 to QC).
Ethical/Consent Statement
All procedures involving human participants were approved by the institutional ethics committee and conformed to the ethical standards of the institutional and national research committee and the World Medical Association Declaration of Helsinki (June 1964). Written consent forms were received from all individuals.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.