
Abstract
Objective:
This article discusses a treatment technique for ectopic earlobe in microtia reconstruction using a delayed postauricular skin flap.
Methods:
From January 2015 to September 2018, microtia reconstruction using a delayed postauricular skin flap was performed on 10 patients with microtia. During the operation, the position of the affected-side earlobe was designed according to the position of the opposite side. The ectopic earlobe was corrected by performing asymmetric Z-plasty or using an irregular “Y-V” advancement skin flap. This allowed full use of the remnant tissue of the microtia-affected ear to form a soft, plump, and realistic earlobe.
Results:
After the earlobe displacement surgery, the blood supply of the earlobe was good, and the reconstructed earlobe survived well without ulceration in all 10 patients. All patients were followed up for 2 months to 2 years. During this time, the positions of the reconstructed ear and the healthy side were basically symmetrical, and the shape of the earlobe formed by the remnant ear was natural.
Conclusion:
The use of asymmetric Z-plasty or an irregular “Y-V” advancement skin flap for the treatment of ectopic earlobe in microtia reconstruction using a delayed postauricular skin flap is a safe and effective method.
Introduction
Microtia is a common congenital craniofacial deformity, and microtia reconstruction is a relatively complicated surgical procedure. The earlobe is located at the lowest end of the auricle. It contains no cartilage tissue and is only composed of skin and subcutaneous fat. Its shape is specific, and attaining a natural and symmetrical earlobe is of great significance in auricle reconstruction. The remnant ear is the most effective autologous material for auricle reconstruction. However, because of the different shape and location of the remnant ear, how to reasonably and fully utilize the ectopic earlobe of the remnant ear tissue to create an earlobe with a realistic shape and symmetrical position is often problematic. From January 2015 to September 2018, we achieved good surgical results through the treatment of ectopic earlobe in microtia reconstruction using a delayed postauricular skin flap. 1
Patients and Methods
This study involved 10 patients (8 male, 2 female; age range, 6-26 years, average age, 13 years) with unilateral congenital microtia. The left ear was affected in 1 patient, and the right ear was affected in 9.
First Stage
The first stage involves delaying the postauricular skin flap and earlobe plasty. First, the ideal location and size of the reconstructed ear are delineated, and the delayed skin flap is prepared according to this location and size. Part of the remnant auricular cartilage is also cutoff to ensure the best positioning of the ear framework in the second stage. Most cases of ectopic earlobe are treated using 1 of the following 2 methods.
Asymmetric Z-plasty
When the ectopic earlobe is positioned backward and downward, asymmetric Z-plasty is adopted (Figure 1A-B). According to the position of the normal earlobe, the location of point a is the correct position of the affected-side earlobe. The position of point a determines the upward or forward movement of the ectopic earlobe. The terminal bottom of the remnant ear is point b, and an asymmetric Z-flap is designed based on points a and b (Figure 1A-B). The axis a-c determines the direction of the earlobe, and this direction affects the smooth and natural connection between the reconstructed auricle and the earlobe.
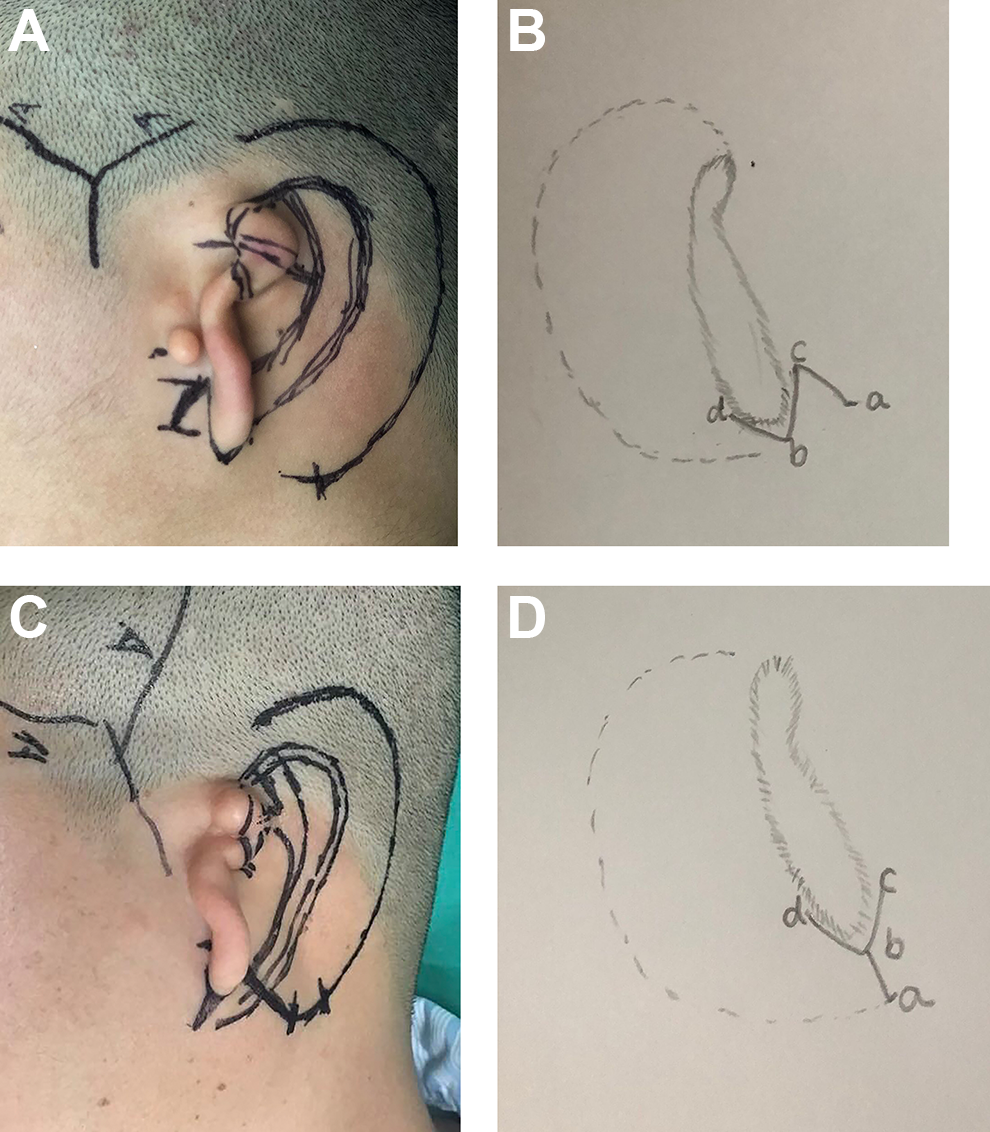
Schema of repair designs. A and B, Asymmetric Z-plasty. C and D, Irregular “Y-V” advancement skin flap.
Irregular “Y-V” advancement skin flap
When the ectopic earlobe is tilted upward, an irregular “Y-V” advancement skin flap is adopted. The correct position of the affected-side earlobe is located at point a, and the terminal bottom of the remnant ear is located at point b. Line a-b and the end of the remnant ear are cut to form a “Y-V” advancement skin flap (Figure1C-D).
Asymmetric Z-plasty is more commonly used in the treatment of ectopic earlobe. The most appropriate surgical method can be selected according to the actual location of the ectopic earlobe.
Second Stage
The procedure in the ear field begins with a skin incision along the original incision lines of the delayed skin flap. The purpose of this incisions is to form a retroauricular skin flap and retroauricular fascia flap. The 3-dimensional costal cartilage framework is placed between the delayed skin flap and the fascia flap. An oblique cut is placed across the upper part of the remnant ear tissue to form the earlobe flap. The earlobe flap is cut open from the middle of the earlobe and thinned appropriately, covering the lower end of the framework to form the earlobe and part of the helix. The surface of the fascial flap is grafted with a medium-thickness skin graft.
Third Stage
After the second operation, the earlobe flap is combined with helix of the reconstructed auricle to form a local small incisure, which is repaired to make the helix line smooth and natural. The earlobe, which is pulled back because of the scar behind the ear, is released by a skin flap or skin grafting to achieve a natural and lifelike shape of the earlobe.
Results
All 10 patients in the present study underwent primary wound healing. The patients were followed up for 6 to 12 months after the second operation. The color, size, and position of the reconstructed ear were basically symmetrical with those of the healthy side, and the shape was lifelike and 3-dimensional. The reconstructed earlobe survived well and maintained a natural shape (Figures 2-4). The patients and their families were satisfied.
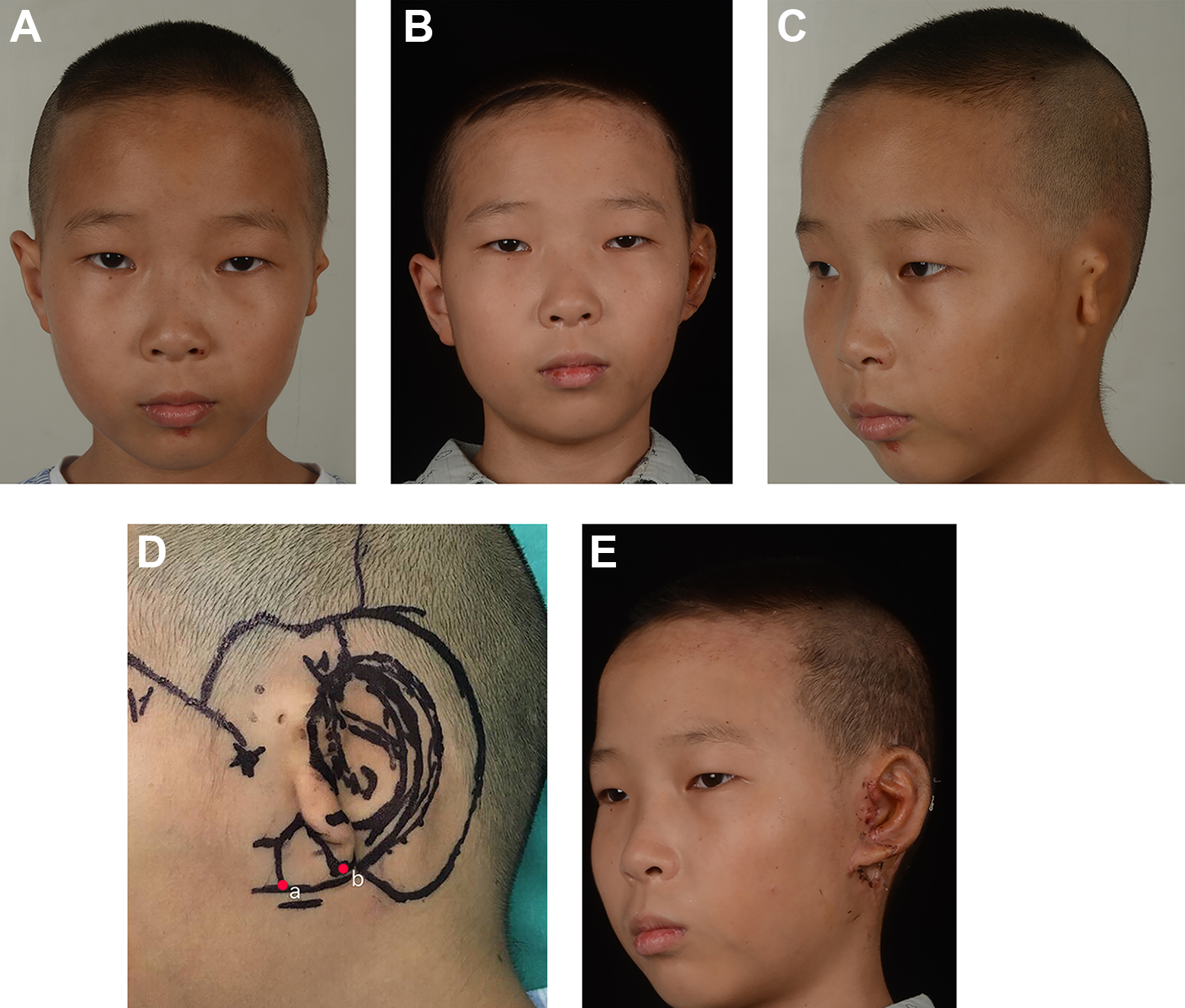
Typical cases. A, Preoperative positive. B, One year after the second-stage operation. C, Preoperation of oblique profile. D, Preoperative design. E, One week after the third-stage operation (third-stage surgery was performed 1 year after second-stage surgery).
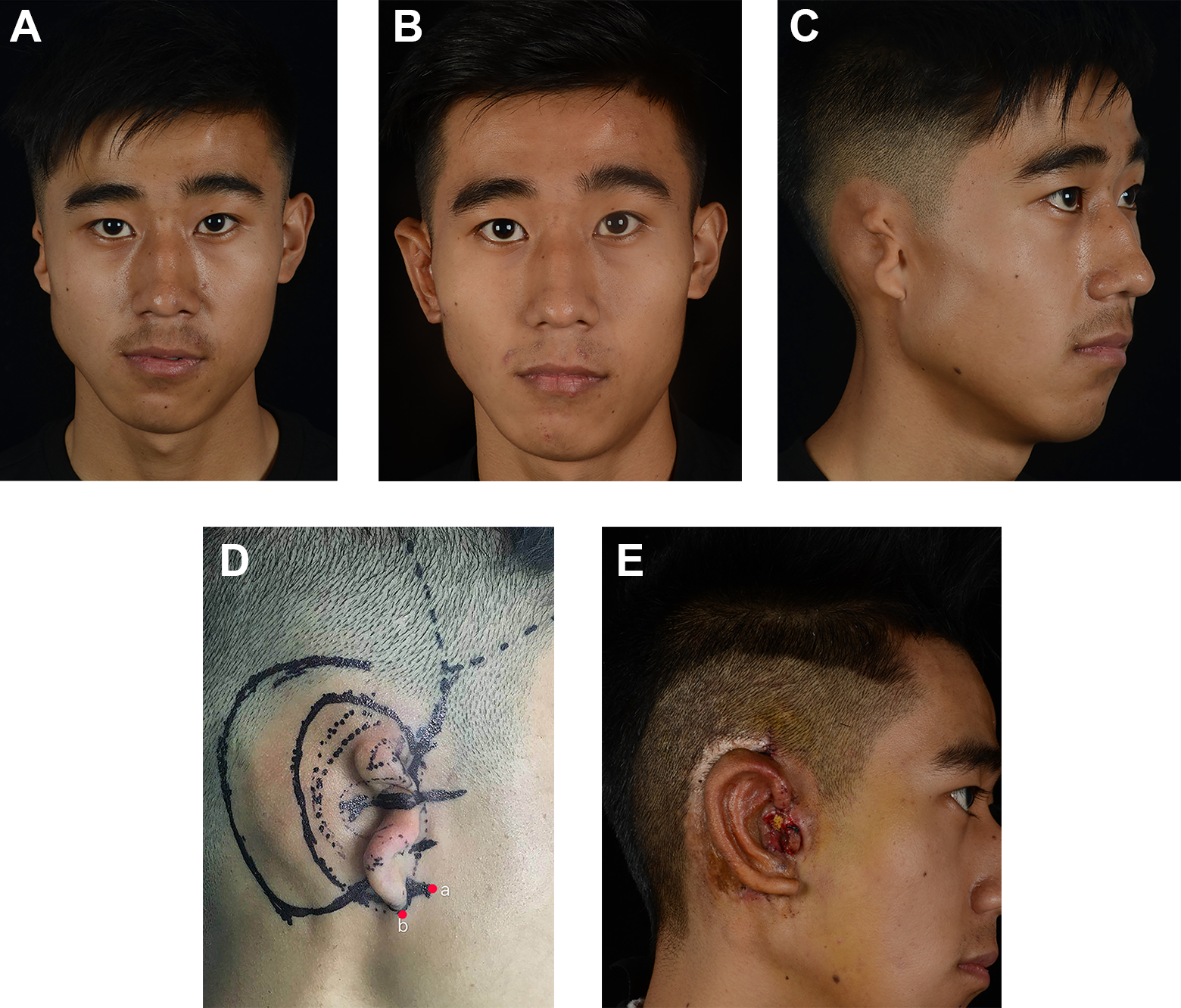
Typical cases. A, Preoperative positive. B, One year after the second-stage operation. C, Preoperation oblique profile. D, Preoperative design. E, One week the after third-stage operation (third-stage surgery was performed 1 year after second-stage surgery).
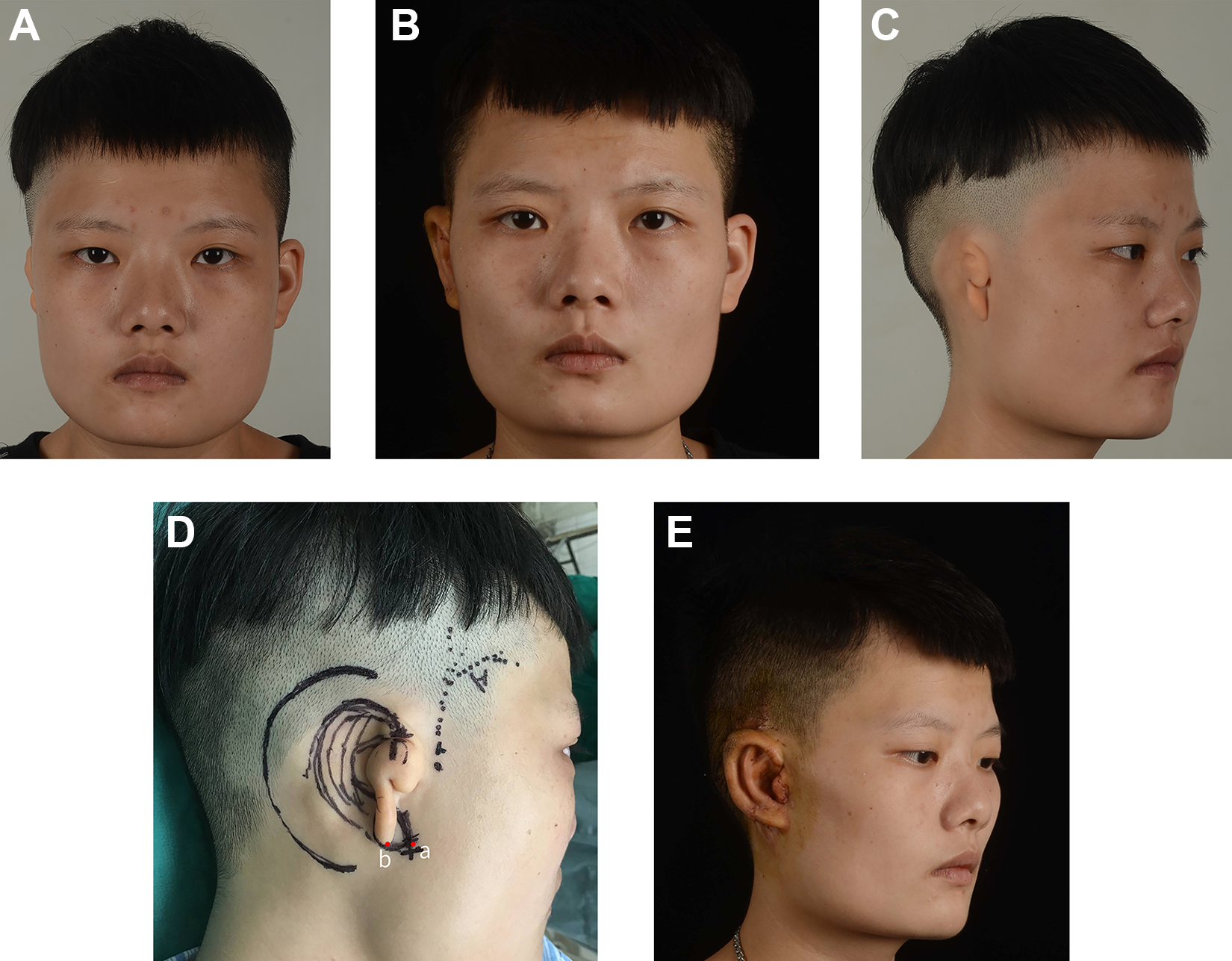
Typical cases. A, Preoperative positive. B, One year after the second-stage operation. C, Preoperation oblique profile. D, Preoperative Z-plasty design. E, One week after the third-stage operation (third-stage surgery was performed 1 year after second-stage surgery).
Discussion
Microtia can be classified into three degrees of severity according to the development of the auricle. In grade I microtia, each part of the auricle can be identified, with small cavity of concha and ear canal opening are present; however, the contour is small, and the inner surface of the ear canal often ends blindly. In grade II microtia, most structures of the auricle are unidentifiable; the remnant ear is irregular, showing a peanut shape, scaphoid shape, or sausage shape; and the external auditory canal is often closed. In grade III microtia, the remnant ear consists only of a small skin tag or hill, or only an ectopic earlobe. The reconstructed ear is usually located at the central parallel line of the long axis of the remnant ear and the long axis of the affected ear, determined according to the distance between the eyes and ears of the healthy side. Therefore, the reasonableness of the position of the ectopic earlobe is the key to the reasonableness and symmetry of the reconstructed ear. Tanzer (1976), 2 Brent (2002), 3 and Nagata 4 introduced several methods of microtia reconstruction in which the earlobe was reconstructed by cutting open the remnant ear tissue. Using remnant ear tissue to cover the end of the framework can improve the appearance of the stiffened costal cartilage. Compared with an earlobe that has been reconstituted by costal cartilage, the shape of the earlobe is life-like, and the color is similar to the healthy side. In the present study, the residual ear tissue was sufficient, and the subcutaneous adipose tissue of the reconstructed earlobe was abundant, soft in texture, and realistic to the touch. Various surgical methods are currently available to reconstruct the earlobe. Each method basically includes the following 2 aspects. First, a framework is implanted or an expander 5 is placed along with earlobe reconstruction in a single-stage procedure. Second, the earlobe was reshaped after the framework implantation. The earlobe is reshaped after the expander, or framework has been placed in a single stage because of the need to protect the blood supply of the pedicle of the skin flap, and the incision and translocation of the ectopic ear tissue are limited to some extent. The ear framework is fixed for staging surgery to maintain the continuity between the earlobe and the helix, the symmetry, and shape of the reconstructed earlobe are also greatly limited. These 2 treatment methods for the ectopic earlobe are not commonly used and may have even been abandoned.
In this study, we performed microtia reconstruction using a delayed postauricular skin flap and a 3-dimensional autogenous costal cartilage framework. The advantages of treating the ectopic earlobe at the same time as performing delayed flap plasty are as follows. Initially, the delayed skin flap design was performed in the first stage of surgery, most of the remnant ear cartilage can be remove in preparation for proper placement of the ear framework. The position of the earlobe can only be reasonable if the position of the ear framework is reasonable. Additionally, this technique ensure complete use of the ectopic earlobe. The round shape of the earlobe is very difficult to attain in the reconstruction of the earlobe. The end of the residual ear is mostly spherical with clinical severity of grade II or III. This end is used to reconstruct the earlobe, and the shape of the earlobe is realistic. However, because of its inappropriate location, it is impractical and may have even been abandoned in other methods of auricle reconstruction. We performed a delayed skin flap operation and adjusted the ectopic earlobe at the same time. The position of the affected-side earlobe was designed according to the position of the opposite-side earlobe. Asymmetric Z-plasty or an irregular “Y-V” advancement skin flap was used at the base of the residual earlobe, and the position of the earlobe was adjusted. Because this method does not involve ear framework placement or expander placement, and because there is no interference of the blood supply of the flap covering the expander or the framework, the affected side can be symmetrical with the healthy side, forming a soft, plump, and realistic earlobe. Finally, in the second stage of surgery, the prepared earlobe was cut in the middle and thinned appropriately to cover the lower end of the framework to form a continuity between the earlobe and helix. Because the ends of the delayed skin flap contain scars tissue after wound healing, the blood supply may be poor. If necessary normal skin pedicle can be retained at both ends of the incision scar to ensure the survival of the reconstructed earlobe. The auricle is positioned at a certain angle in relation to the face. When designing the flap, the inclined position of the earlobe should be symmetrical with the other side.
The treatment of ectopic earlobe in microtia reconstruction using a delayed postauricular skin flap is a safe and effective method to maximize the use of residual ear tissue and thus achieve the reconstruction of a symmetrical and realistic earlobe. When the ectopic earlobe is positioned backward and downward, asymmetric Z-plasty is adopted. When the ectopic earlobe is tilted upward, an irregular “Y-V” advancement skin flap is adopted. The degree of irregularity of the design is based on the need to adjust the position of the ectopic earlobe for reasonable flap formation. Accurate determination of the appropriate earlobe position is the key to successful surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.