
Abstract
Parotid gland fistula after microtia reconstruction is relatively rare, with only 3 cases having been reported in the literature. It may be caused by the presence of an accessory parotid gland or surgical damage to parotid gland tissues. The principal treatment is dressing the wound. Here, we report the first case of parotid fistula after microtia reconstruction using a delayed retroauricular flap, which healed following wound dressing and an injection of botulinum toxin type A (CBTXA) into the parotid gland.
Keywords
Introduction
Microtia is the second most common facial deformity, after congenital cleft lip and palate. 1 It is principally caused by abnormal development of the first and second parotid arches during embryonic development and manifests as dysplasia of the auricle, mandible, and soft tissues, such as the masseter muscle and parotid gland, with a lateral transverse facial cleft or accessory ear. Surgical reconstruction is the preferred treatment, but this is frequently associated with complications, such as hematoma, infection, skin flap necrosis, exposure of the auricular cartilage scaffold, poor shape of the reconstructed auricle, or iatrogenic pneumothorax. 2 Of these, postoperative parotid gland fistula is very rare. Here, we report the first case of parotid gland fistula after microtia reconstruction using a delayed postauricular skin flap, which healed following dressing and the injection of botulinum toxin type A (CBTXA) into the parotid gland.
Case Report
A 19-year-old male patient with left-sided microtia (Figure 1) underwent first-stage microtia reconstructive surgery under local anesthesia in 2017. This involved a delayed postauricular skin flap formation, ectopic earlobe transfer, blind tract resection, and auricular cartilage backfill. Two weeks after this initial surgery, an abscess was identified below the original blind canal. He was then treated by debridement and intravenous antibiotics. After this healed, he underwent second-stage surgery under general anesthesia. An erect, 3-dimensional ear framework, which had been fabricated from autogenous rib cartilage, was covered with a delayed skin flap and postauricular fascia, overlying the grafted skin.

Preoperative lateral view of microtia.
One month after this surgery, a mass ∼2 cm long and 1.5 cm wide was identified below the patient’s left earlobe (Figure 2A). During the physical examination, a left-sided facial swelling and purulent discharge were identified, but no ectopic tissue was present in the external auditory canal. Computed tomography (CT) showed ankylotia and a mass, which was considered to be an abscess, with dysplasia of the middle ear, a sclerotic mastoid, and invisible ossicles, with a slight enlargement of the inner ear canal (Figure 2B). On the basis of prior clinical experience, debridement was performed under local anesthesia. No connection between the abscess sinus tract and the ear framework was identified during this procedure. In addition, cefathiamidine was administered intravenously for 3 days, and wound drainage was initiated.
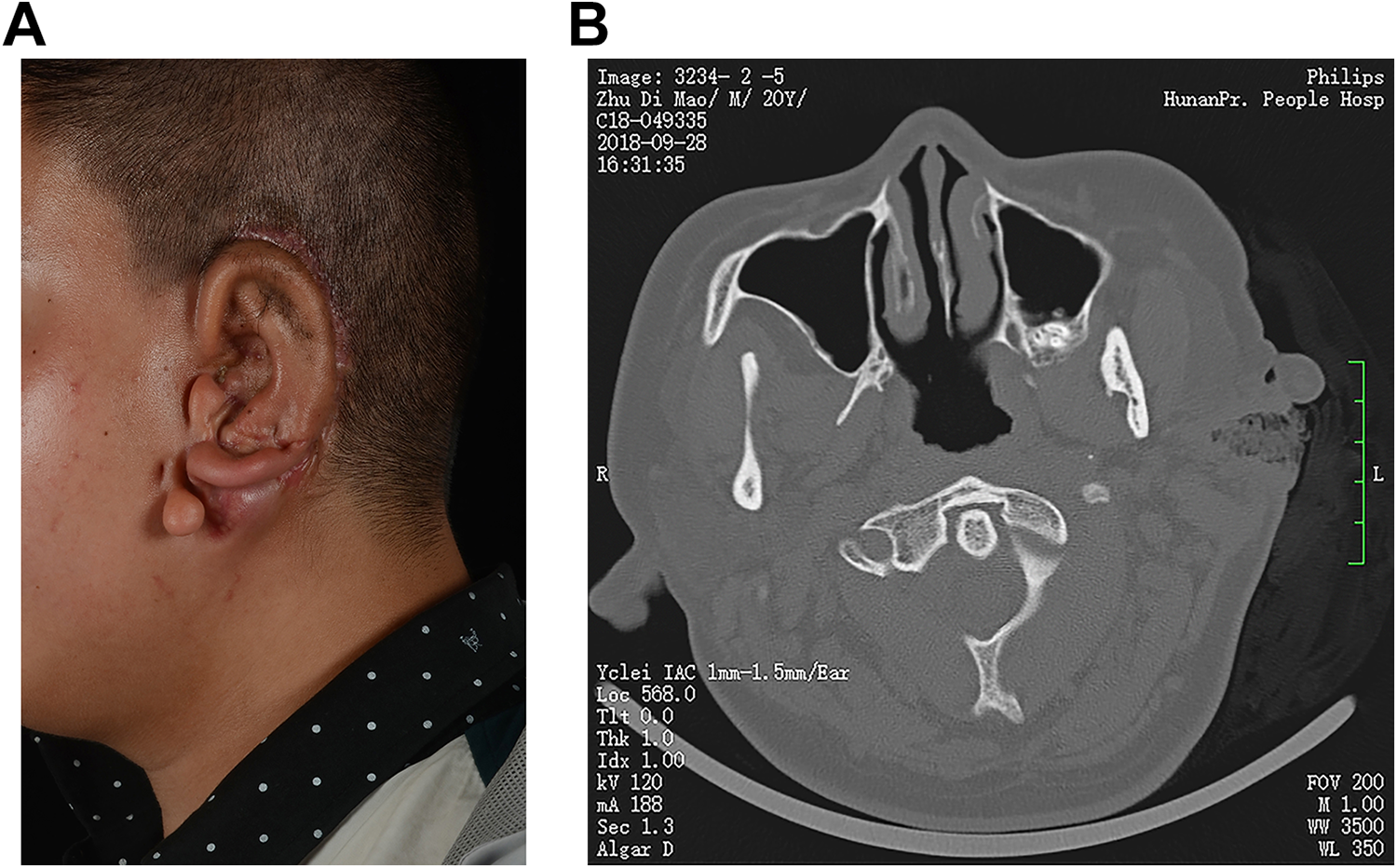
A, Abscess formation after auricular reconstruction. B, Computed tomography (CT) examination showed the formation of left ear abscess (coronal plane).
Two weeks later, repeat CT examination showed that an abscess or sinus tracts may have formed and the lesion was absorbed than before (Figure 3). During the treatment, the patient reported a sound reminiscent of water flowing over the wound when he was hungry; therefore, we took a sample of fluid from the wound to test for the presence of salivary amylase, and this was positive (>16 000 U/L), which confirmed the involvement of a salivary gland. Gram staining of the fluid yielded gram-negative rods and gram-negative and positive cocci. Therefore, a diagnosis of parotid gland fistula was made after consultation with a maxillofacial surgeon.
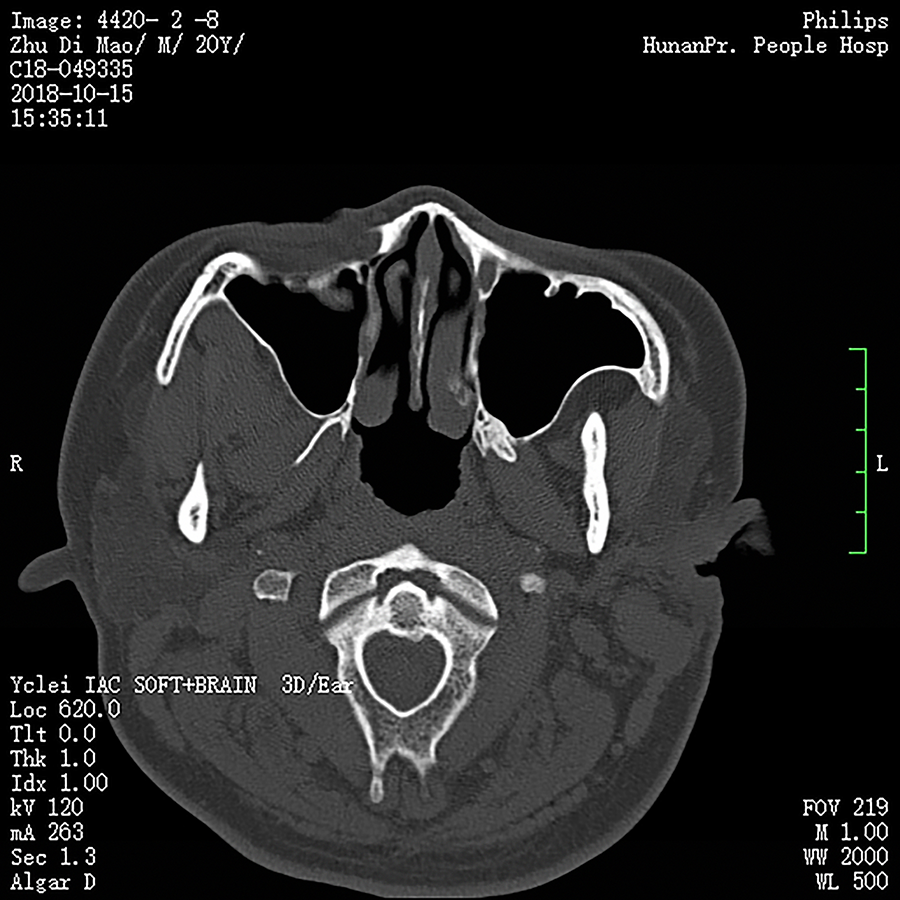
Computed tomography (CT) examination shows a reduced abscess (coronal plane).
The patient was required to avoid stimulating the secretion of saliva by avoiding hot and sour food items. Under sterile conditions, the superficial and deep lobes of the patient’s left parotid gland were injected with a total of 32 units (8 evenly distributed injections through the skin of 4U each) of CBTXA (Lanzhou Institute of Biological Products Co., Ltd; NMPA approval number: S10970037) via a 25-gauge spinal needle, on a single occasion. This was not associated with any complications and the patient’s symptoms subsequently improved significantly. When he returned 2 weeks later, he had recovered well (Figure 4). One year later, the patient underwent third stage of microtia reconstruction surgery, which yielded good postoperative results. There had been no recurrence of parotid gland fistula 2 years after the original diagnosis, and the patient was satisfied with the appearance of his reconstructed ear (Figure 5A and B).

The abscess wound healed.
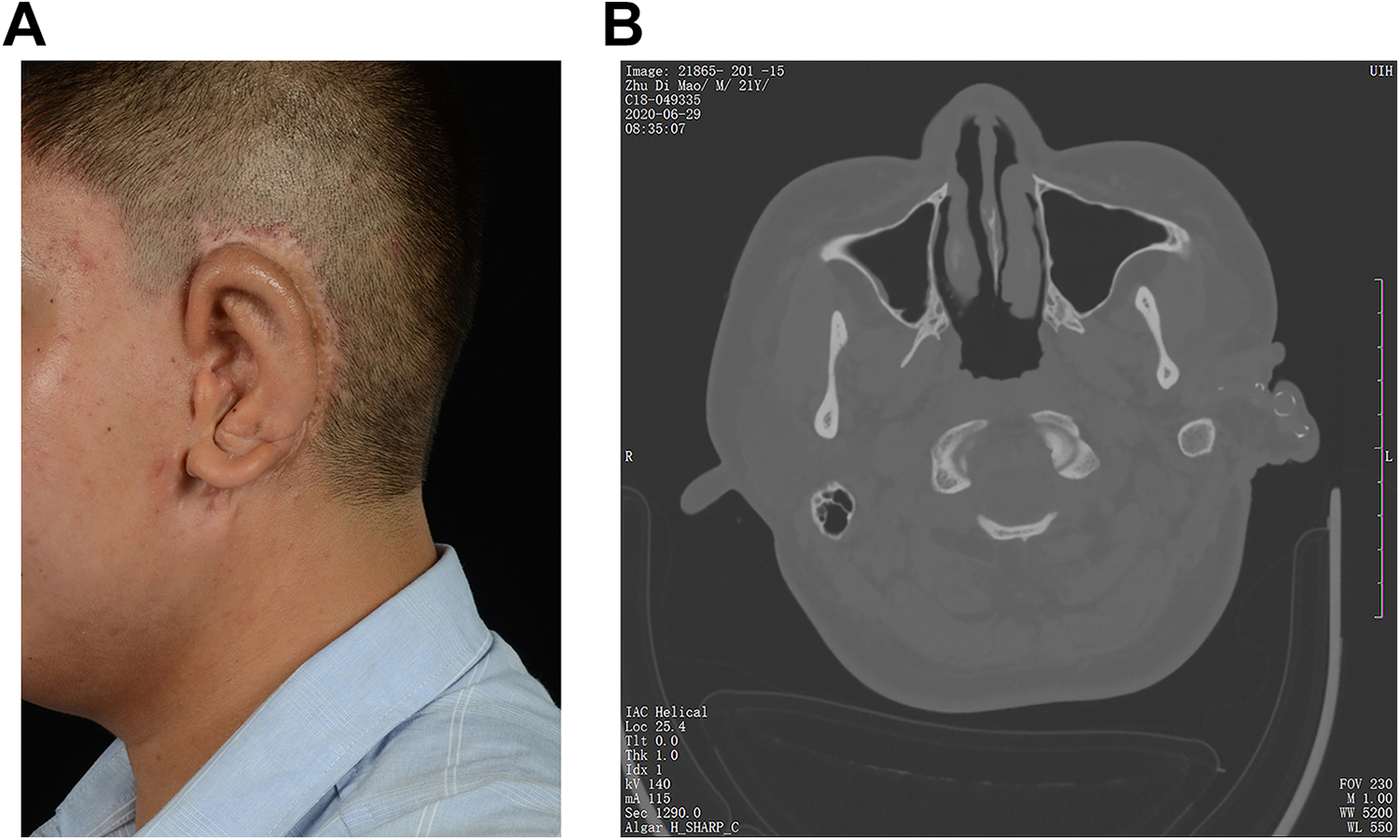
A, One-year follow-up after the third stage of microtia reconstruction. B, Computed tomography (CT) examination of 1-year follow-up after the third stage of microtia reconstruction (coronal plane).
Discussion
Since 2017, we have treated congenital microtia using our own delayed postauricular skin flap method. 3,4 In the present report, we describe a complication of this procedure in which the skin and soft tissues of the parotid region were repeatedly infected and a sinus tract formed. The final diagnosis was a parotid gland fistula, which is rare, with very few previous reports in the literature. Yavuzer et al 5 reported a case of parotid gland fistula that was diagnosed 7 days after microtia reconstruction in 2000, which might be consistent with the presence of an accessory parotid gland lying anterior to the parotid gland and superior to the masseter muscle. Even when the surgeons are familiar with the normal anatomy of the parotid gland region, a parotid gland fistula might develop in rare cases when the retroauricular fascia flap is raised deep to inferior to and anterior to the ear during surgery. However, unfortunately, images were not provided in the report to confirm the presence of an accessory parotid gland. Moreover, Morovic et al 6 reported 2 cases of parotid gland fistula after the second stage of concha reconstruction, and speculated that after surgery in the locality of the parotid, the inflammatory response and abnormal healing of the wound might cause traction on the parotid tissues, resulting in injury to the parotid fascia and ultimately parotid gland fistulation. There have been no previous reports of this complication in China.
After considering the whole process of diagnosis and treatment carefully, we can summarize the present case as follows. (1) An abscess developed in the parotid gland region and appeared after the first-stage surgery. We considered that the parotid gland might have been damaged during the resection of the congenital blind tract. (2) After the intravenous infusion of antibiotics, debridement, and drainage, the wound did not heal; therefore, a complication other than bacterial infection alone was considered. (3) During the treatment, the patient reported that he could hear a sound reminiscent of water flowing in his left ear when he was hungry. We considered that the patient wanted to eat when he was hungry, and therefore, salivary gland secretion increased as the result of a conditioned reflex. In addition, we observed that the fluid draining from the wound was clear. (4) The patient’s salivary amylase and CT examination findings were consistent with parotid gland fistula, and this diagnosis was made after consultation with a maxillofacial surgeon.
To treat the fistula, we used a single set of injections of CBTXA into the parotid gland, which yielded good results. Botulinum toxin type A is a safe and reliable drug that has been used in the cosmetic and therapeutic fields for many years. It inhibits the release of acetylcholine from nerve endings in the salivary glands, which reduces the secretion of saliva, thereby having a positive clinical effect in cases of parotid gland fistula. 7 -11 Botulinum toxin type A injection, combined with pressure bandaging can promote the formation of fascia on the surface of a damaged parotid gland, thereby reducing the overflow of saliva and permitting wound healing.
When masses or abscesses form below the earlobe after microtia reconstruction, the complication of parotid gland fistula should be considered, and salivary amylase testing and imaging should be undertaken, to reduce the chance of a clinical misdiagnosis of common wound infection. Assessment of the results of treatment of more patients with CBTXA is required before it can be definitively recommended as an appropriate treatment. However, CBTXA appears to be a safe and well-tolerated conservative treatment for parotid gland fistula.
Footnotes
Authors’ Note
Bo Zhang and Suqi Xu are joint first author.
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.