
Abstract
Importance
The technique combining a crescent-shaped costal framework with the biomechanical properties of residual auricular cartilage is expected to enhance the structural stability and aesthetic outcomes of the reconstructed ear in mild conchal-type microtia.
Objective
To present a technique that integrates a crescent-shaped costal framework with the biomechanical properties of residual auricular cartilage to reconstruct mild conchal-type microtia, aiming to improve structural stability and aesthetic outcomes.
Design
Retrospective study.
Setting
Auricular Reconstruction Center, Plastic Surgery Hospital, Peking Union Medical College, between January 2023 and January 2024.
Participants
Patients with grade I or II conchal-type congenital microtia underwent auricular reconstruction using this refined technique. The procedure integrates a crescent-shaped costal framework with residual auricular cartilage to achieve single-stage ear reconstruction.
Intervention
The surgery technique combining a crescent-shaped costal framework with the biomechanical properties of residual auricular cartilage was used.
Main Outcomes and Measures
Postoperative outcomes were assessed based on the integrity of auricular subunit structures, bilateral symmetry, scar visibility, complication rates, Ear-Q (Appearance), and patient satisfaction.
Results
The study included 26 unilateral microtia cases (20 right ears and 6 left ears) with a mean follow-up period of 9.43 ± 3.57 months. According to aesthetic evaluations, 23 patients (88.46%) received 4 points (indicating an excellent aesthetic effect). Patient satisfaction was high, with 24 patients (92.31%) and their families reporting favorable outcomes. The mean Ear-Q (Appearance) score was 62.23 ± 18.68. Aesthetic results were rated as the highest score in 23 cases (88.46%). There were no significant dimensional differences between the reconstructed and unaffected ears, and no significant changes between immediate postoperative and final follow-up measurements.
Conclusions and Relevance
The combination of a crescent-shaped costal framework with residual auricular cartilage offers a reliable, aesthetically-refined, and technically-efficient approach for the repair of mild conchal-type microtia.

Keywords
Introduction
Congenital microtia, a common craniofacial anomaly, occurs in approximately 3.79 per 10,000 live births, 1 ranking as the second most frequent craniofacial defect and among the 10 most prevalent congenital disorders worldwide. The condition presents a wide range of clinical manifestations, from a small, malformed auricle to complete absence of the external ear.
Nagata2,3 classified microtia into 3 main categories: lobular type, concha type, and anotia. Tanzer 4 considered conchal-type microtia a severe form (grade III) of lop ear, whereas Cosman and Nagata excluded it from the lop ear classification and instead defined it as type II microtia. Type II microtia is further divided into type IIA, characterized by an underdeveloped conchal component, and type IIB, in which the conchal component is normal.5-6 Each subtype presents distinct anatomical challenges, requiring tailored surgical strategies for optimal reconstruction.
Concha-type microtia (CTM) is characterized by a hypoplastic helix and scapha, a poorly-defined antihelix, and a narrow external auditory canal, while the earlobe is typically preserved. Owing to the relatively-large amount of residual tissue, recent research has focused on developing surgical techniques that optimize the use of remaining skin and cartilage to achieve both functional and aesthetic reconstruction.
Although various techniques have been explored, 7 including auricular cartilage unfolding, autologous auricular cartilage transplantation, and composite tissue grafting, autologous rib cartilage grafting remains the gold standard for CTM reconstruction. Accordingly, previous studies have focused on refining framework sculpting techniques and optimizing skin incisions to maximize the utilization of residual tissue.8 -11
This study presents an approach that integrates a crescent-shaped costal framework with the biomechanical properties of residual auricular cartilage for the treatment of CTM. We aimed to explore whether the technique provides strong structural support, achieves improved aesthetic outcomes, and simplifies the surgical procedure.
Patients and Methods
A retrospective review was conducted on microtia patients who underwent auricular reconstruction using a crescent-shaped costal framework combined with residual auricular cartilage at the Auricular Reconstruction Center, Plastic Surgery Hospital, Peking Union Medical College, between January 2023 and January 2024. Postoperative outcomes, auricular substructure definition, and patient satisfaction were evaluated and analyzed.
This study was approved by the Medical Ethics Committee of the Chinese Academy of Medical Sciences, and written informed consent was obtained from the patients or from legal guardians for those under 18 years of age (protocol no. 2021-166). Inclusion criteria were as follows: (1) a diagnosis of unilateral type II CTM, (2) absence of surgical contraindications, and (3) provision of informed consent with willingness to perform this surgical method.
Surgical Procedures
The Crescent Cartilage Framework Fabricating
The entire surgical procedure was performed under general anesthesia. The curved segment of the seventh costal cartilage is typically harvested (Figure 1A). Using its natural curvature, a crescent-shaped framework is carefully sculpted with a scalpel. The central portion of the cartilage is hollowed to form a groove that replicates the morphology of the helix and scapha (Figure 1B).

Fabrication of the crescent-shaped cartilage framework. (A) The curved segment of the seventh costal cartilage is harvested. (B) A crescent-shaped framework is sculpted with a scalpel, and the central portion is hollowed to form a groove that replicates the contour of the helix and scapha.
Procedure for the Remnant Ear
After local swelling fluid injection, an incision is made along the helical rim and extended posteriorly to the auriculocephalic junction. Fibrous adhesions are released, and the residual auricular cartilage is fully exposed through complete dissection (Figure 2A-B). The cartilage is folded posteriorly and secured with 5-0 absorbable sutures to reconstruct the antihelix. The anterior segment of the helical cartilage is incised, advanced anteriorly, and fixed to the original crus of the helix to restore its contour. Simultaneously, the conchal cartilage is retracted posterosuperiorly and anchored to the periosteum of the skull to redefine the conchal cavity. Comparison with the contralateral ear at this stage reveals the absence of the superior helix and scapha.
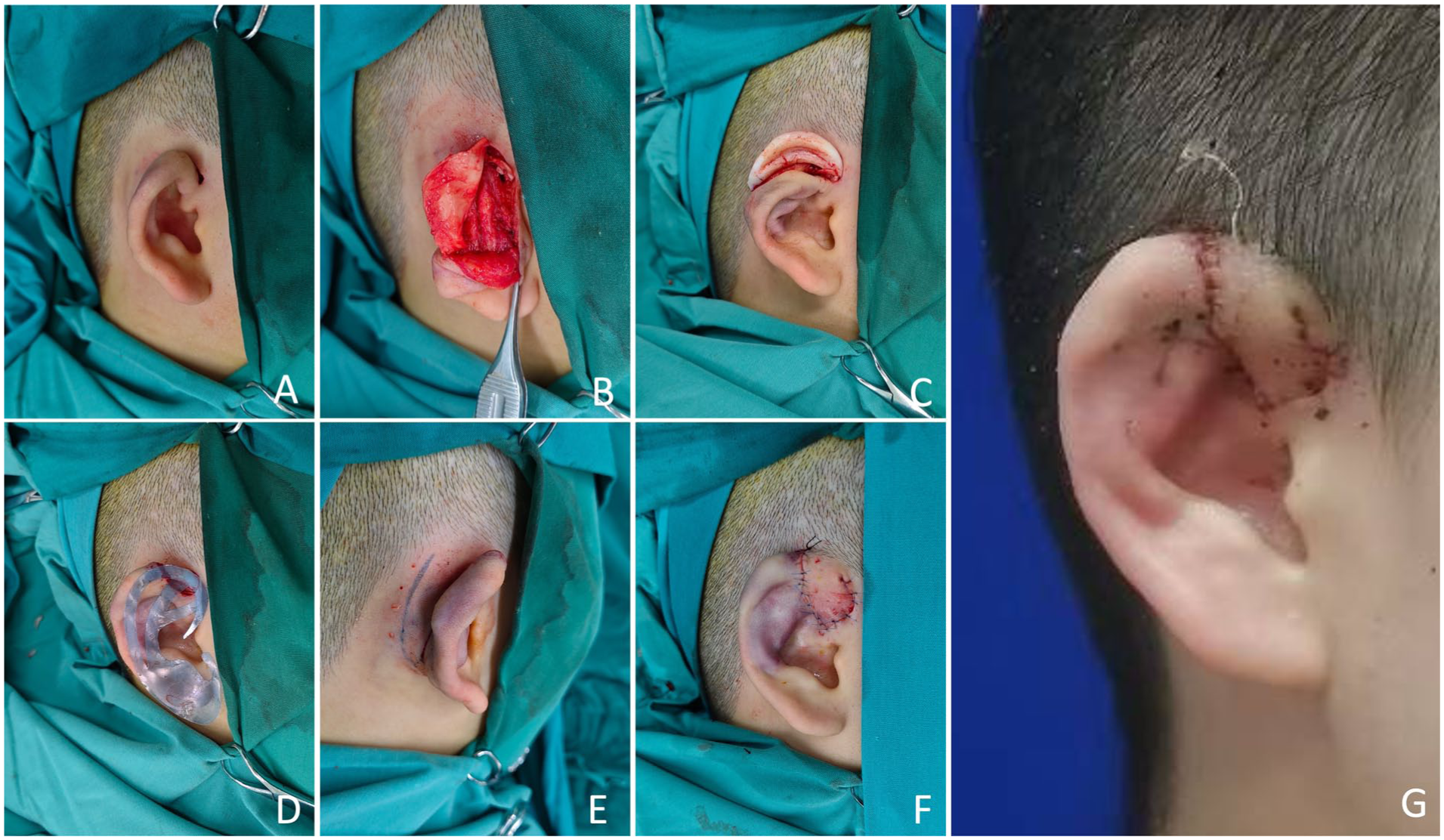
Surgical procedures of auricular reconstruction. (A) Preoperative view of the affected ear. (B) fibrous adhesions are released, and the residual auricular cartilage is completely dissected for full exposure. (C-D) The prefashioned crescent-shaped cartilage framework is sutured to the margins of the residual auricular cartilage to restore the contours of the helix and scapha. (E) A triangular pedicled skin flap is designed posterior to the auricle, elevated, and advanced anteriorly to cover the anterior helical cartilage. (F) Immediate postoperative view of the reconstructed ear. (G) Two-week postoperative observation of the reconstructed ear.
Management of Posterior Ear Flap and Crescent Cartilage Framework
The prefabricated crescent-shaped cartilage framework is sutured to the margins of the residual auricular cartilage to reconstruct the helical and scapha contours (Figure 2C-D). The biomechanical properties of the native residual cartilage reinforce the autologous costal cartilage framework, providing additional structural stability. Following reconstruction, the auricular dimensions closely approximate those of the contralateral ear.
A triangular pedicled skin flap is then designed posterior to the auricle, elevated, and advanced anteriorly to cover the anterior helical cartilage (Figure 2E).
Negative-pressure suction (−52 ~ −62 kPa) connected to a drain is applied for 5 days to enhance contour definition. Sutures are removed 14 days after surgery.
Evaluation of the Aesthetic Results
Standardized preoperative, immediate postoperative, and follow-up photographs were obtained for all patients. At the last follow-up, postoperative complications and patient satisfaction were documented. Satisfaction was evaluated using a 3-point scale (0 = unsatisfied, 1 = generally satisfied, 2 = highly satisfied). The EAR-Q12 -14 (Ear Appearance) questionnaire was also used to assess patient satisfaction with the morphological outcomes of the reconstructed auricle.
EAR-Q is a validated, Rasch-developed patient-reported outcome measure for patients ~8 to 29 years with congenital or acquired ear conditions. It includes ear-specific scales (Appearance; Adverse Effects) and health-related quality-of-life scales (Psychological, Social, School, Appearance-Related Distress), plus single items on ear scars and hearing-aid appearance. Each scale is scored independently by summing item responses and converting to a 0 to 100 score (higher = better); single items are reported as raw responses.
Four weeks after surgery, 2 independent plastic surgeons evaluated the aesthetic outcomes utilizing standardized preoperative and postoperative photographs. A 4-point Likert scale was applied (1 = poor, 2 = fair, 3 = good, 4 = excellent). Evaluation criteria included the integrity of auricular subunit structures, bilateral symmetry, and invisibility of incision scars. Inter-rater reliability was assessed using Cohen’s weighted kappa coefficient.
Statistical Analysis
The length, width, and perimeter of each affected auricle were measured preoperatively, immediately postoperatively, and at follow-up. The measurement methods and standards are illustrated in Figure 3. Statistical analysis was performed using IBM SPSS version 27.0, with quantitative data expressed as mean ± standard deviation. For normally-distributed data, intergroup comparisons were conducted using the independent samples t-test, and intragroup comparisons using the paired t-test. The Mann-Whitney U test was applied for intergroup comparisons of non-normally-distributed data, while the Wilcoxon signed-rank test was used for intragroup comparisons. A P-value of less than .05 was considered statistically significant.

Assessment of the reconstructed ear dimensions. Measurements of ear length, width, and height were obtained for both the reconstructed ear and the unaffected side. a, superior portion of the reconstructed ear; a’, superior portion of the unaffected ear; b, inferior portion of the reconstructed ear; b’, inferior portion of the unaffected ear; c, point where the superior edge of the tragus intersects with a line parallel to the helix of the reconstructed ear; c’, corresponding point on the unaffected ear; L, length of the reconstructed ear; L’, length of the unaffected ear; W, width of the reconstructed ear; W’, width of the unaffected ear; H, height of the reconstructed ear; h’, height of the unaffected ear.
Results
All patients presented with unilateral CTM, including 6 cases involving the left ear and 20 involving the right ear. Each patient underwent auricular reconstruction using a crescent-shaped costal cartilage framework combined with the biomechanical properties of residual auricular cartilage, without prior surgical interventions.
A total of 26 patients (16 males and 10 females) with a mean age of 10.23 ± 3.75 years underwent surgical repair for conchal-type microtia at the Plastic Surgery Hospital, Peking Union Medical College. Among them, 6 cases involved the left ear and 20 the right. The mean follow-up period was 9.43 ± 3.57 months. During follow-up, all reconstructed auricles showed satisfactory repair with excellent morphology and symmetry, and no postoperative complications were observed. Demographic data and results are summarized in Table 1. Inter-rater reliability was assessed using Cohen’s weighted kappa coefficient, which yielded a quadratic weighted κ of .705, indicating substantial agreement.
Patient Characteristics, Aesthetic Outcomes, and Patient Satisfaction.

Of the 26 patients, EAR-Q assessment scores ranging from 18 to 40, which were converted to 35 to 100, with a mean score of 62.23 ± 18.68 (Table 1).
No significant differences were found between the auricular dimensions at the final follow-up and those of the unaffected side. Similarly, no significant differences were observed between the immediate postoperative and final follow-up measurements (Table 2). No complications occurred during or after surgery. The average surgical time was 3.08 ± 0.44 hours (2.00 hours ~ 3.83 hours). Representative cases are shown in Figure 4.
Symmetry Comparison Between the Reconstructed Ear and the Health Ear.


Postoperative view of case 1. An 8-year-old male patient with right conchal-type microtia. (A) Preoperative view of the affected ear. (B) View of the unaffected ear. (C-D) Two-month postoperative observation of the reconstructed ear.
Discussion
The extent and strategy of auricular reconstruction depend on the type and severity of the deformity. Conchal-type microtia is characterized by a deficient helix and scapha, an underdeveloped antihelix, and a narrow external auditory canal, while the earlobe remains intact. Given the relatively-large residual ear and abundant tissue availability, recent research has focused on optimizing surgical techniques to maximize the use of residual skin and cartilage.
Surgeons have explored various techniques15,16,17 including auricular cartilage unfolding, autologous auricular cartilage transplantation, and composite tissue transplantation. However, correction using only residual auricular cartilage may not achieve symmetry with the contralateral ear in size. Harvesting cartilage from the ipsilateral or contralateral concha carries the risk of conchal deformity and often results in suboptimal outcomes in cases with significant structural deficiencies, particularly when reconstructing the scapha and triangular fossa.
In addition to auricular cartilage transplantation, auricular reconstruction using autologous rib cartilage grafting has been recommended for the treatment of CTM. Accordingly, previous studies have primarily focused on modifications to the ear framework and variations in skin incision design to optimize the use of residual tissue. Reported techniques range from complete to partial ear frameworks. Madura et al 10 and Han 18 described a method for reconstructing the helix and antihelix using costal cartilage, emphasizing its value in correcting mild CTM. Many surgeons employ the Nagata technique, which utilizes a complete rib cartilage framework for CTM reconstruction.2,19 -22
In CTM cases, residual auricular structures can be incorporated into the reconstructed ear after appropriate modification. The reconstruction primarily focuses on restoring the helix, antihelix, scaphoid fossa, and cavum concha. In this technique, the residual auricular cartilage is completely dissected, folded posteriorly, and secured to establish the proper conchal height. The edges of the residual cartilage are then used to reconstruct portions of the antihelix and the inferior crus. The prefabricated crescent-shaped framework is subsequently sutured to the margins of the native cartilage to restore the helix, antihelix, and scapha.
The residual auricular cartilage possesses inherent anterior biomechanical properties, offering greater structural support than frameworks composed entirely of costal cartilage. Integrating the native residual cartilage with the partial costal framework allows the reconstructed ear to retain the natural mechanical characteristics of autologous tissue
Compared with techniques that rely solely on auricular or contralateral conchal cartilage, this method achieves more defined contours of the scapha and antihelix. Although it requires a small thoracic donor-site incision (approximately 2.50 cm), the approach substantially reduces the amount of autologous cartilage needed compared with total reconstruction methods. Moreover, it attains a more natural conchal height by utilizing the intrinsic biomechanical properties of the native cartilage.
This study has 2 main limitations. First, the sample size was relatively small. Second, as a retrospective analysis, it did not include a comparison of different surgical techniques for mild CTM. Therefore, the findings only demonstrate that the proposed technique is a feasible approach achieving favorable outcomes. Future clinical research will aim to address this limitation through prospective studies comparing the advantages and disadvantages of various reconstruction methods.
Conclusion
This study utilizes the inherent biomechanical properties of the residual auricular cartilage to reinforce the supplemental costal framework, reducing the risk of collapse and deformation. The proposed technique provides stable projection, symmetrical appearance, and adequate structural support for the reconstructed ear. The combination of a crescent-shaped costal framework with residual auricular cartilage offers a reliable, aesthetically-refined, and technically-efficient approach for the repair of mild CTM.
Footnotes
Acknowledgements
The authors wish to thank Mrs. Liya Du for her photographic contributions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All authors have nothing to disclose. This study was funded by CAMS Innovation Fund for Medical Sciences (Grant 2021-12M-1-001). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethical Approval
Ethics approval was granted by the Ethics Committee of the Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (Protocol No. 2021-166).