
Abstract
Synovial sarcoma is a soft tissue tumor originating from mesenchymal precursor stem cells. It is usually seen in young males and lower extremities. It is only seen in 10% of head and neck region and nasopharynx which is a very unexpected location. We report a rare case treated with radiotherapy and chemotherapy.
Significance Statement
Synovial sarcoma, a malignant and aggressive soft tumor, is an extremely rare condition that occurs in the nasopharynx. There are no clinical and radiologic pathognomonic findings. Histopathology and immunohistochemical studies play an important role in the diagnosis. In addition to surgical excision, neoadjuvant radiotherapy and chemotherapy can also be applied. Follow-up is important for this tumor as it has high local recurrence and poor prognosis.
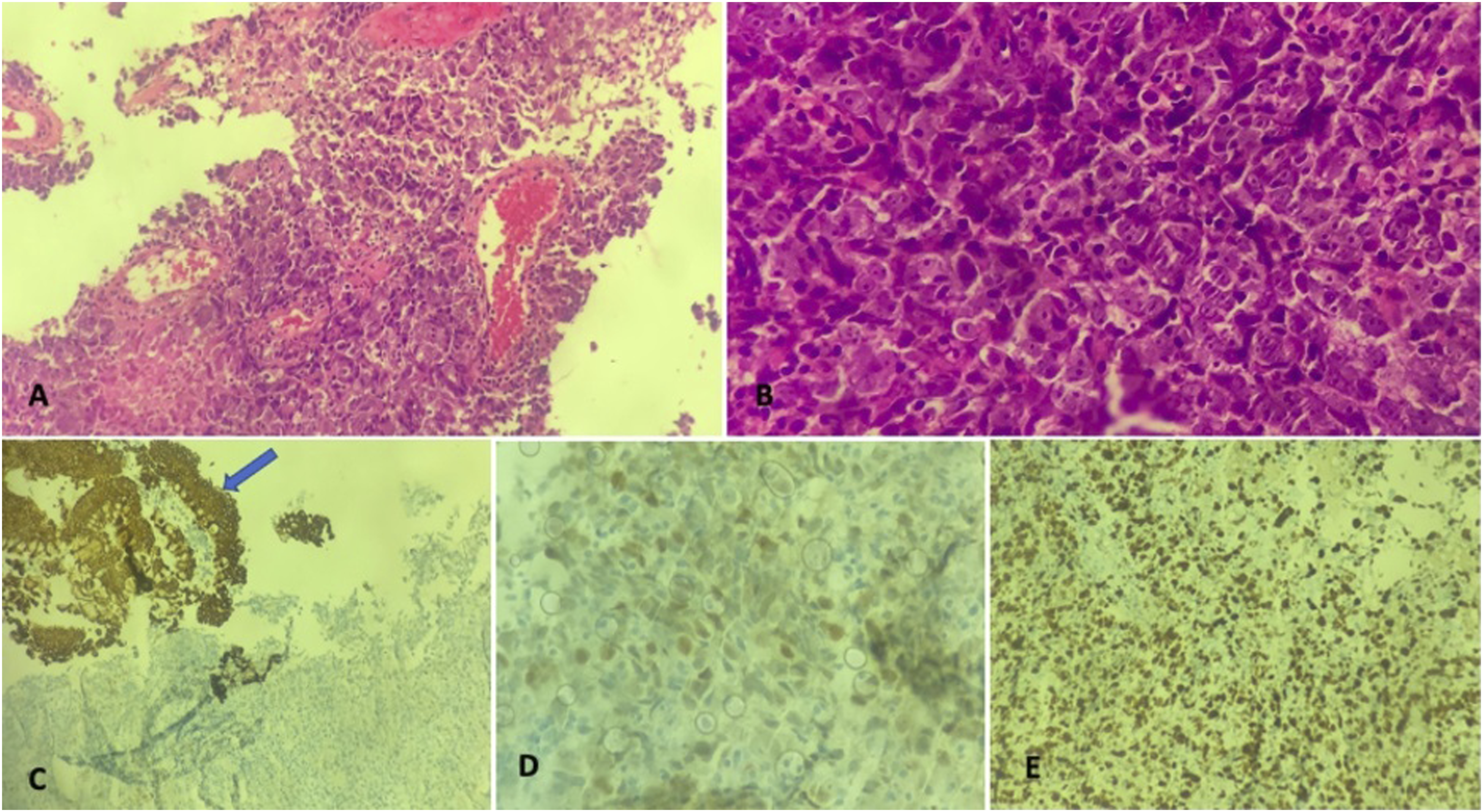
A 66-year-old woman presented to our emergency department with sudden onset of numbness in the right extremities and visual disturbance. She had diabetes mellitus for 2 years but did not take any medication and had no history of trauma. Non-contrast brain computed tomography (CT) was performed with a prediagnosis of cerebrovascular disease. Since no significant pathology was detected, contrast-enhanced brain CT angiography was performed to determine possible vascular occlusion. Thrombolytic treatment was initiated in the patient with no significant pathology. In addition, the images showed a 2.5 × 3 × 3.5 cm hypodense mass lesion on the left posterior wall of the nasopharynx, which protruded into the airway. The lesion was minimally, heterogeneously contrasted and obliterated to the left Rosenmuller fossa. There were also pathologic lymphadenopathy appearances in bilateral cervical areas, the largest of which was 24 × 18 mm in size on the left, containing cystic openings and heterogeneously contrasting. Brain diffusion magnetic resonance (MR) imaging obtained to determine the infarct area also showed marked diffusion restriction in the left part of the nasopharynx (Figure 1). Biopsy was performed with a prediagnosis of nasopharyngeal cancer. Histopathologic and immunohistochemical studies showed that the lesion was composed of malignant spindle cells. The patient was diagnosed as synovial sarcoma due to strong positivity of vimentin, focal positivity of EMA, TLE1, and CD99 positivity (Figure 2). PET-CT revealed no distant metastasis except for cervical lymphadenopathy. The patient did not accept the operation and received radiotherapy and chemotherapy. A control CT scan performed 1 year later showed significant regression in the lesion size. Axial section brain CT angiography image (A) shows a hypodense mass lesion protruding into the airway on the left later-posterior wall of the nasopharynx (asterix). On diffusion-weighted images, the mass is hyperintense on B-1000 series (B) and hypointense on ADC series (C), showing marked restriction (arrows). In A and B, a malignant neoplastic formation consisting of round, oval shaped, hyperchromatic nucleated cells with frequent mitotic activity is observed under the surface epithelium of the nasopharynx. The lesion is Pan-CK negative, while the nasopharyngeal surface epithelium is positive (blue arrow). CD-99 positivity is shown in D and TLE1 positivity is shown in E.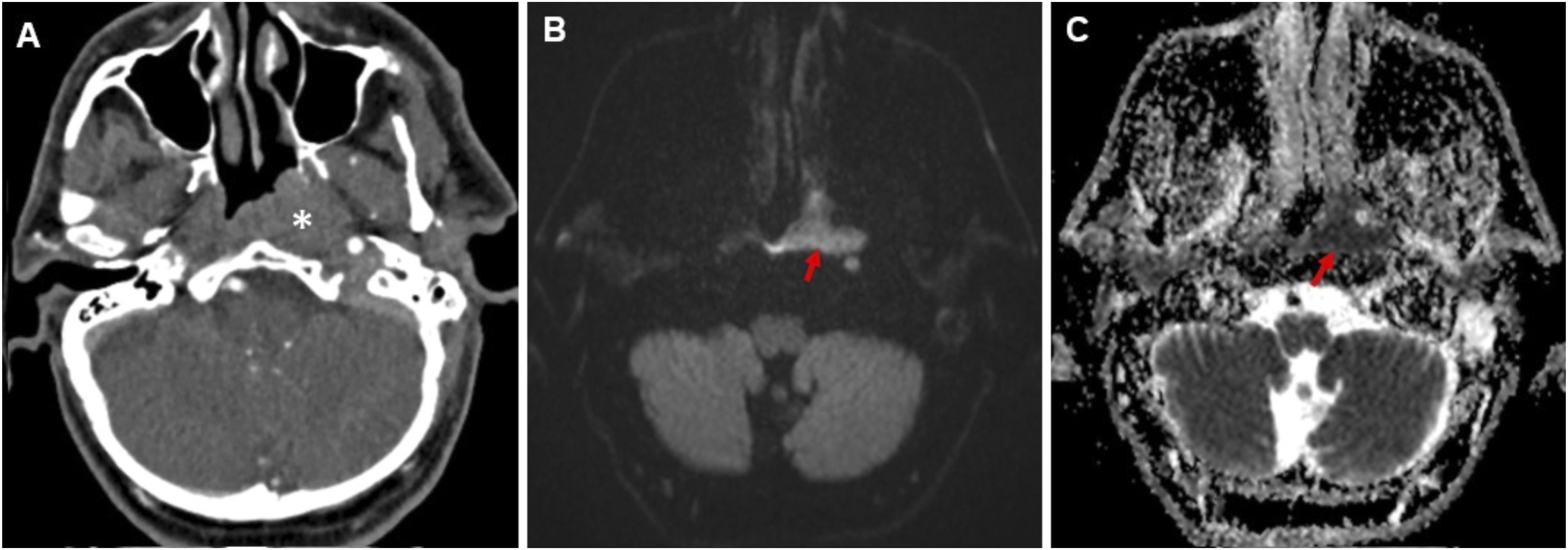
Synovial sarcomas are rare aggressive malignant tumors and constitute 7–10% of all sarcomas. They are usually seen in young males in the lower extremities, especially around the knee. Synovial sarcomas of the head and neck are rare, accounting for 3%. 1 The first case was reported in the pharynx in 1954. 2 Nasopharynx is an extremely rare location and has been reported in the literature on a case-by-case basis. Symptoms vary according to the location and may include pain, dysphagia, epistaxis, and airway obstruction. 3 There are no pathognomonic findings on radiologic imaging. CT and MR images may show hemorrhage, cystic cavities and calcification. However, none of these were present in our case. 1 Histopathologically, there are mainly three types, namely monophasic, biphasic, and poorly differentiated. In immunohistochemical studies, BCL-2, vimentin, EMA and CD-99 are positive, while S100 protein, desmin, SMA, and CD34 expression are negative. 4,5 Although the diagnosis is usually made immunohistochemically, the gold standard is the reciprocal translocation t(x;18)(p11;q11). 3 Five-year survival of synovial sarcoma ranges between 47 and 72% and tends to local recurrence. 4 Treatment consists of surgical excision with radiotherapy and in advanced cases, chemotherapy may be effective. 5
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.